Stillbirth Without Viability: An Intrapartum Diagnosis of Twin Reversed Arterial Perfusion (TRAP) Sequence in Monochorionic Twin Pregnancy
Sujata Siwatch, Rohan Sodhi, Gaurav Khastgir, Pooja Sikka

TL;DR
A rare case of TRAP sequence in a twin pregnancy is reported, highlighting the importance of prenatal care and the classification of stillbirths.
Contribution
The paper presents a clinical case of TRAP sequence diagnosed during labor, emphasizing diagnostic and classification challenges.
Findings
TRAP sequence was diagnosed during intrapartum delivery of a monochorionic twin pregnancy.
The case underscores the need for early antenatal ultrasonography in twin pregnancies.
It raises questions about stillbirth classification in cases of nonviable twins.
Abstract
Twin reversed arterial perfusion (TRAP) sequence is a rare complication of monochorionic twin pregnancies, characterised by a nonviable acardiac twin perfused by a structurally normal "pump" twin. We report a case of a 33-year-old woman, G4P2012, who presented at 29 weeks in advanced labour with a history of inadequate antenatal care. She delivered a live male neonate, followed by the unexpected delivery of an intrauterine mass initially suspected to be a fibroid. Further evaluation revealed the mass to be an acardiac twin, and placental examination confirmed monochorionic diamniotic placentation, establishing the diagnosis of TRAP sequence. This case highlights the critical importance of early and detailed antenatal ultrasonography in twin pregnancies. It also raises important questions regarding the classification of stillbirths in the context of severe congenital anomalies…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
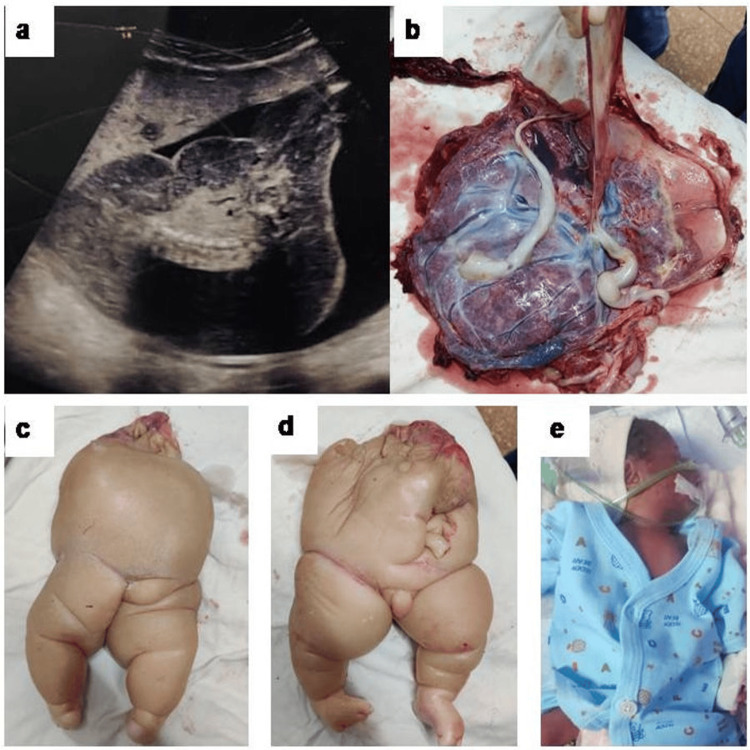 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAssisted Reproductive Technology and Twin Pregnancy · Prenatal Screening and Diagnostics · Ectopic Pregnancy Diagnosis and Management
Introduction
Twin reversed arterial perfusion (TRAP) sequence is a rare congenital anomaly unique to monochorionic twin pregnancies, characterised by a structurally normal "pump" twin and a severely malformed "acardiac" twin that lacks a functional heart. It is estimated to occur in one in 35,000 pregnancies and represents about 1% of all monochorionic twin gestations [1]. With improved imaging and assisted reproduction, the reported incidence is increasing [2]. The acardiac twin, being nonviable, survives solely on reversed arterial perfusion from the pump twin, which is at risk of high-output cardiac failure, preterm labour, and other complications [1]. Early diagnosis is essential to optimise outcomes. We present a unique case of TRAP sequence diagnosed only after vaginal delivery of the pump twin at 29 weeks, due to inadequate antenatal care. With advances in medical facilities improving the viability of preterm babies, the gestational cut-off for defining a stillbirth is decreasing [3]. However, definitions can be confusing, as seen in our case of a twin pregnancy with an acardiac twin that has no chance of viability. Should this be labelled a stillbirth, knowing it is not viable at birth? Our case highlights the importance of thorough ultrasound examinations and vigilant monitoring in twin pregnancies. It also prompts a reconsideration of the criteria used to define stillbirths in infants with malformations incompatible with life.
Case presentation
A 33-year-old woman, G4P2012, presented at 29 weeks in advanced labour. She had two previous vaginal deliveries at term and a spontaneous first trimester abortion. Her antenatal care was notably inadequate, limited to two self-initiated ultrasound scans. The first, performed at 11 weeks, revealed a twin gestation: one live foetus and one missed abortion. A subsequent scan at 22 weeks identified a single live foetus consistent with gestational age, along with a fundal fibroid.
On presentation, her per vaginal findings revealed a fully dilated cervix with the vertex at -2 station and she soon vaginally delivered a live male neonate weighing 1147 grams (Figure 1E). Following delivery, a firm, smooth mass was palpated through the cervix. A provisional diagnosis of a fundal fibroid was considered. Upon reviewing the earlier scans, suspicion was raised for a twin gestation with an acardiac twin.
Ultrasonographic and gross images of the acardiac twin and pump twina) Ultrasound picture of acardiac twin seen as a large heterogenous intrauterine mass with spine-like calcificationb) Monochorionic diamniotic placentac-d) Acardiac twine) Pump twin
Bedside ultrasonography (USG) revealed a 15 x 10 cm hypo-heteroechoic intrauterine mass with spine-like calcifications and areas of vascularity (Figure 1A). Vaginal exploration under general anaesthesia led to the delivery of an acardiac twin weighing 1133 grams (Figures 1C-1D). Examination of the placenta confirmed monochorionic diamniotic placentation (Figure 1B), consistent with the diagnosis of TRAP sequence. The newborn was shifted to the Neonatal Intensive Care Unit (NICU) after birth, but succumbed at 30 hours of life due to prematurity-related complications. The immediate postpartum period was uneventful, and the mother was discharged on the fourth postnatal day.
Discussion
TRAP sequence is a rare congenital anomaly characterised by the presence of a structurally normal "pump" twin and an anomalous "acardiac" twin, often lacking a functional heart and other vital organs. It usually occurs in monozygotic twins, with a frequency of one in 35,000 pregnancies and is common in female twins [1]. However, with advancements in USG, prenatal diagnosis and assisted conception, van Gemert et al. report the incidence to be rising towards 2.6% of monochorionic pregnancies [2]. Acardiac foetuses are classified as acephalus (60-75%) with absent head and upper body; anceps (~10%) with partial development including a rudimentary head; acormus (~5%) with only a head; amorphus (~20%) with no recognisable structures and myelacephalus with a partially developed head with identifiable upper limbs [4-6].
The etiopathogenesis involves abnormal placental arterio-arterial vascular communication between twins, leading to an imbalance of interfoetal circulation. [7]. Unequal embryonic splitting and genetic abnormalities leading to defective embryogenesis have also been hypothesised [8,9]. The pump twin receives high-pressure blood flow, while the perfused twin suffers from reversed deoxygenated blood flow, impairing its development. Without a functioning heart, the acardiac twin relies on the pump twin’s circulation in a parasitic way.
Early diagnosis is crucial for deciding therapy and planning the ideal time of delivery. The characteristic ultrasound feature is the reversed blood flow into the acardiac twin via its umbilical artery, observed with colour Doppler ultrasound. Additionally, important findings include a foetus with multiple severe malformations, subcutaneous oedema, large fluid accumulations, and an absence of a heart [1].
Moore et al. have described a regression equation to deduce the weight (in grams) of the anomalous twin [10]. A key prognostic factor is the ratio of acardiac twin weight to donor twin weight (%). When this ratio exceeds 70%, preterm delivery occurs in 90%, polyhydramnios in 40%, and congestive heart failure in 30% [11]. However, estimating the weight of the acardiac twin is difficult. A low pulsatility index in the donor twin's umbilical artery on colour Doppler indicates a poor prognosis.
The pump twin with cardiac activity has a high risk for congestive cardiac failure. Other complications include preterm labour and premature rupture of membranes secondary to uterine overdistension. It may also suffer from hypoxia and growth restriction due to deoxygenated blood entering it via the vascular anastomotic channels. These factors contribute to a high perinatal mortality rate of around 55% for the pump twin [12]. Early diagnosis allows time for intrauterine radiofrequency ablation (RFA) and prevents complications for the viable twin [13].
Currently, there is no established consensus regarding the ideal time of delivery. Some authors have suggested adopting a conservative management approach in case the weight ratio is less than 70% and there is no evidence of heart failure in the pump twin [14]. Weekly ultrasonography is recommended in these cases. In cases with radiological evidence of heart failure, polyhydramnios or features of hydrops foetalis, an aggressive early first-trimester intervention is recommended [8]. Platt et al. were the first to suggest an interventional approach [15]. There are several approaches targeted at occluding or destroying the aberrant arteriovenous connections. These include alcohol embolisation, RFA, microwave ablation, thermocoagulation, laser coagulation and high intensity focused ultrasound [7,16,17]. However, studies have demonstrated that RFA is the most effective with a high safety index [7].
A stillbirth is a baby born without signs of life as indicated by the absence of breathing, heartbeat, or definite movements of voluntary muscles beyond a specified gestational age threshold. The definition of stillbirths has been evolving. With the advancement of medical facilities, as the ability to salvage preterm neonates is improving, the gestational cutoff for defining a ‘stillbirth’ is reducing [3]. However, cases like the TRAP sequence challenge these definitions. The acardiac twin, while technically born without signs of life, is nonviable by nature of its malformation. Whether such births should be recorded as stillbirths remains debatable and invites reconsideration of classification criteria for congenital anomalies incompatible with life.
Conclusions
Our case demonstrates a TRAP sequence in monochorionic gestation, diagnosed after delivery of the first twin. Adequate antenatal care, early diagnosis and management would have avoided the complications of the trapped acardiac twin. This highlights the need for detailed USG and close monitoring in twin pregnancies. It also provokes a re-examination of the criteria for defining stillbirths in babies with malformations incompatible with life. A multidisciplinary approach involving obstetricians, radiologists and neonatologists is essential for optimising outcomes of the pump twin and for planning the appropriate time of delivery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Twin reversed arterial perfusion sequence: prenatal diagnosis and treatment Matern Fetal Med Ye X Wang J Lu J Li N Ding W Fu Y Chen M 262267420224040669610.1097/FM 9.0000000000000172 PMC 12087880 · doi ↗ · pubmed ↗
- 2Acardiac twin pregnancies part VI: why does acardiac twinning occur only in the first trimester?Birth Defects Res van Gemert MJ Ross MG van den Wijngaard JP Nikkels PG 68769511320213358060710.1002/bdr 2.1882 PMC 8247889 · doi ↗ · pubmed ↗
- 3A review of stillbirth definitions: a rationale for change Eur J Obstet Gynecol Reprod Biol Kelly K Meaney S Leitao S O'Donoghue K 23524525620213324837910.1016/j.ejogrb.2020.11.015 · doi ↗ · pubmed ↗
- 4The acardiac monster. A review of the world literature and presentation of 2 cases Am J Obstet Gynecol Napolitani FD Schreiber I 5825898019601372774710.1016/s 0002-9378(16)36520-6 · doi ↗ · pubmed ↗
- 5Conservative management in a case of uncomplicated trap sequence: a case report and brief literature review J Prenat Med Pepe F Teodoro MC Luca C Privitera F 2934920152735869510.11138/jpm/2015.9.3.029PMC 4909109 · doi ↗ · pubmed ↗
- 6Fetus amorphus: report of a case Surg Gynecol Obstet Simonds J 171179411925
- 7Twin reversed arterial perfusion sequence: current treatment options Int J Womens Health Vitucci A Fichera A Fratelli N Sartori E Prefumo F 4354431220203254725110.2147/IJWH.S 214254 PMC 7266514 · doi ↗ · pubmed ↗
- 8The monozygotic twinning process, the twin-twin transfusion syndrome and acardiac twins Placenta Benirschke K 9239283020091974866710.1016/j.placenta.2009.08.009 · doi ↗ · pubmed ↗