Anesthetic Management for Valve-in-Valve Transcatheter Aortic Valve Replacement (TAVR) After Primary TAVR Failure With Mixed Aortic Valve Dysfunction
John Choi, Jennifer Shmukler, Derek He

TL;DR
This paper describes a successful redo TAVR procedure in a high-risk patient using detailed imaging, real-time guidance, and proactive strategies to ensure safety and recovery.
Contribution
The paper presents a novel anesthetic and procedural approach for high-risk redo TAVR with mixed aortic valve dysfunction.
Findings
Detailed preoperative imaging and real-time TEE guidance ensured successful valve deployment and hemodynamic stability.
Proactive vasoactive strategies countered pacing-induced hypotension and enabled fast-track recovery.
Post-deployment imaging confirmed no complications and immediate improvement in valve function.
Abstract
Redo valve-in-valve transcatheter aortic valve replacement (TAVR) confronts anesthesiologists with compounded hemodynamic and neurologic risk. We managed an 85-year-old male with severe mixed prosthetic aortic dysfunction whose pre-procedural transthoracic echocardiogram showed a peak velocity of 3.7 m/s⁻¹, a mean gradient of 24 mm Hg, an effective orifice area of 0.8 cm², and a posteriorly directed, eccentric regurgitant jet filling >50% of the left ventricular outflow tract. The failure was suspected to have been caused by structural valve deterioration within five years after the initial TAVR. CT confirmed adequate coronary heights and true-lumen dimensions for a 26 mm Sapien 3 Ultra Resilia valve. General anesthesia was induced with 20 mg of etomidate and 200 mcg of fentanyl and maintained with low-dose propofol (50-100 mcg/kg/min) and remifentanil (0.05-0.1 mcg/kg/min), permitting…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
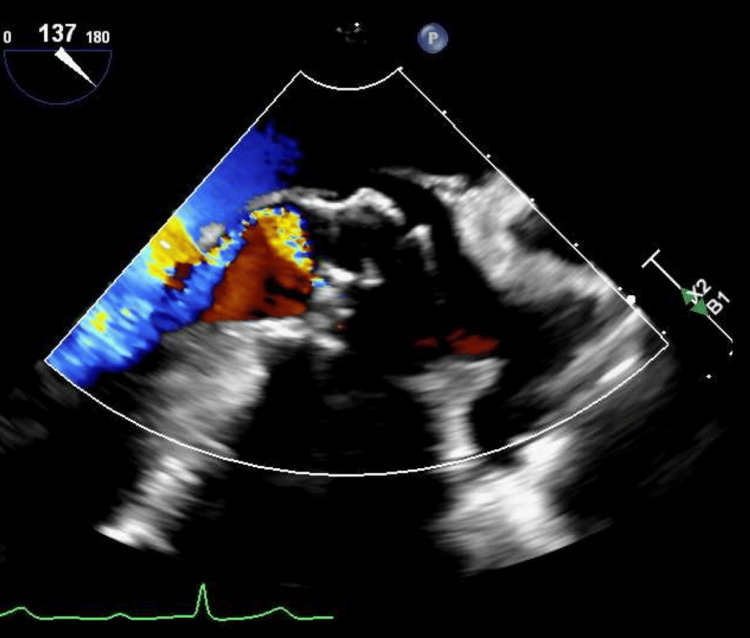 Figure 1
Figure 1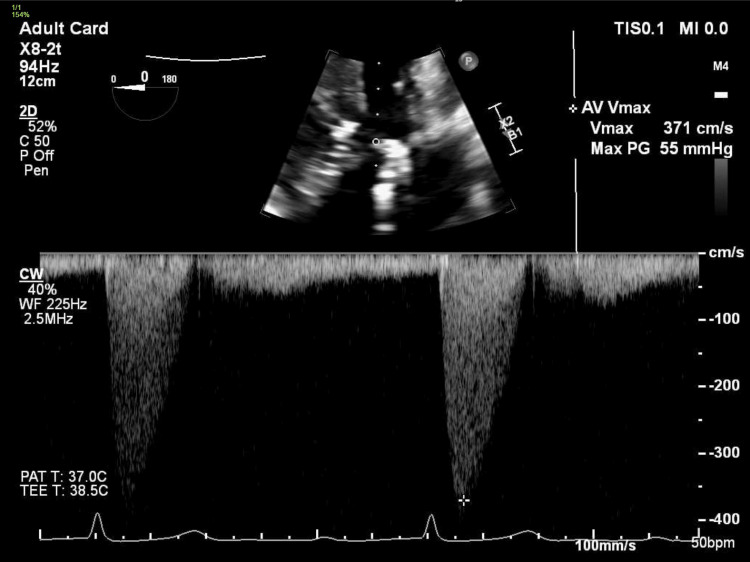 Figure 2
Figure 2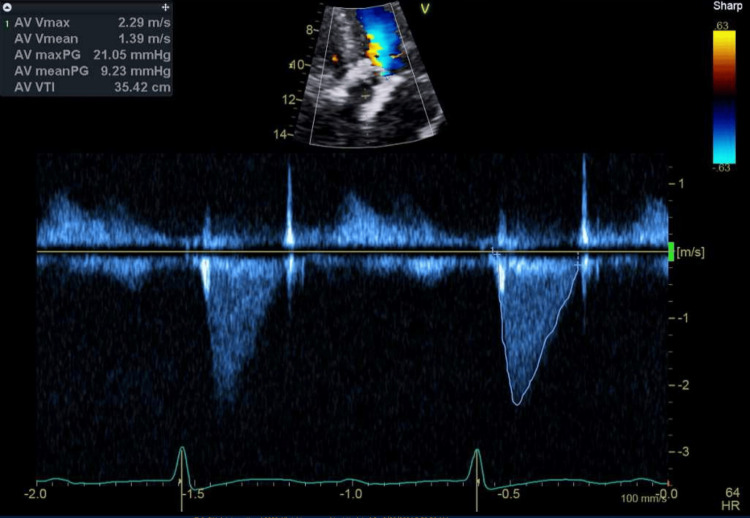 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
Introduction
Valve-in-valve transcatheter aortic valve replacement (TAVR) has become a critical intervention for patients whose initial TAVR fails due to structural valve deterioration, malposition, or mixed stenosis and regurgitation, offering a less invasive alternative to surgical explantation in high-risk populations [1]. Although redo transcatheter aortic valve replacement (TAVR) comprises only 0.5-0.7% of all TAVR procedures, contemporary multicenter registries report technical success rates exceeding 90%, with mid-term survival comparable to that of first-time TAVR but with distinct procedural risks such as coronary obstruction and patient-prosthesis mismatch [1,2].
As the indications for TAVR broaden to include lower-risk and younger patients, anesthetic practice has gradually shifted from routine general anesthesia (GA) to monitored anesthesia care (MAC) with conscious sedation in straightforward cases [3]. However, complex ViV redo procedures, particularly in elderly patients with mixed aortic stenosis and regurgitation, frequently necessitate GA augmented by transesophageal echocardiography (TEE) and advanced hemodynamic monitoring to promptly detect and manage rapid hemodynamic swings during induction, rapid ventricular pacing, and valve deployment [4]. Valve-in-valve transcatheter aortic valve replacement (ViV TAVR) has become a critical intervention for patients whose initial TAVR fails due to structural valve deterioration, malposition, or mixed stenosis and regurgitation, offering a less invasive alternative to surgical explantation in high-risk populations [1]. Although redo TAVR comprises only 0.5-0.7% of all TAVR procedures, contemporary multicenter registries report technical success rates exceeding 90%, with mid-term survival comparable to that of first-time TAVR but with distinct procedural risks such as coronary obstruction and patient-prosthesis mismatch [1,2].
As the indications for TAVR broaden to include lower-risk and younger patients, anesthetic practice has gradually shifted from routine general anesthesia (GA) to monitored anesthesia care (MAC) with conscious sedation in straightforward cases [3]. However, complex ViV redo procedures, particularly in elderly patients with mixed aortic stenosis and regurgitation, frequently necessitate GA augmented by transesophageal echocardiography (TEE) and advanced hemodynamic monitoring to promptly detect and manage rapid hemodynamic swings during induction, rapid ventricular pacing, and valve deployment [4].
Optimal anesthetic management hinges on the selection of induction agents with minimal cardiovascular depression (e.g., etomidate, fentanyl), proactive vasopressor strategies during pacing, and continuous TEE to assess ventricular function and valve position in real time [3,5]. Tailoring these approaches to patients with limited cardiac reserve and multiple comorbidities is essential to minimize perioperative morbidity and mortality.
In this report, we detail the perioperative anesthetic considerations and approaches employed for an 85-year-old man undergoing ViV TAVR after primary TAVR failure resulting in severe mixed aortic stenosis and insufficiency, with the aim of guiding anesthesiologists managing similar high-risk scenarios. Optimal anesthetic management hinges on the selection of induction agents with minimal cardiovascular depression (e.g., etomidate, fentanyl), proactive vasopressor strategies during pacing, and continuous TEE to assess ventricular function and valve position in real time [3,5]. Tailoring these approaches to patients with limited cardiac reserve and multiple comorbidities is essential to minimize perioperative morbidity and mortality.
In this report, we detail the perioperative anesthetic considerations and approaches employed for an 85-year-old man undergoing ViV TAVR after primary TAVR failure resulting in severe mixed aortic stenosis and insufficiency, with the aim of guiding anesthesiologists managing similar high-risk scenarios.
Case presentation
An 85-year-old man with a history of hypertension, hyperlipidemia, type 2 diabetes mellitus (A1c 6.5%), heart failure with preserved ejection fraction (LVEF 50% in August 2024), three-vessel coronary artery disease, chronic lacunar strokes, proximal basilar artery stenosis, subacute subdural hematoma one month prior, and prior TAVR (Edwards S3 26 mm in 2019) presented with progressive dyspnea on exertion and fatigue. Transthoracic echocardiography revealed moderate transvalvular aortic stenosis with moderate regurgitation (Figures 1, 2). Given his age, comorbidities, and an STS-PROM of 3.0% for surgical aortic valve replacement (AVR), he was deemed a poor surgical candidate. He underwent several days of medical optimization, primarily aggressive diuresis, to relieve volume overload and improve respiratory symptoms before proceeding to valve-in-valve TAVR.
TEE in midesophageal long axis view showing moderate to severe aortic insufficiency with turbulent, transvalvular posteriorly directed eccentric jet.
TEE in deep gastric view showing peak anterograde velocity through aortic valve of 3.7 m/s, consistent with moderate aortic stenosis.
In the hybrid operating room, standard ASA monitors were applied, and a 20-gauge left radial arterial line was placed for beat-to-beat hemodynamic monitoring. A single 14-gauge peripheral IV was established in the left antecubital fossa. After preoxygenation, general endotracheal anesthesia was induced, and the trachea was secured with an 8.0 mm cuffed endotracheal tube. Following intubation, the interventional team placed a 7 Fr femoral venous sheath in the right groin. A bispectral index (BIS) sensor was applied to guide anesthetic depth. General anesthesia was selected because complex ViV deployment required continuous TEE guidance, controlled ventilation for precise valve positioning, and immediate hemodynamic rescue capability during prolonged rapid-pacing runs, which are needs that conscious sedation could not reliably meet in this frail patient.
Anesthesia was maintained with propofol (50-100 µg/kg/min) and remifentanil (0.05-0.2 µg/kg/min) infusions for rapid titration. Norepinephrine and epinephrine infusions were prepared; norepinephrine was titrated to maintain systolic blood pressure at the patient’s baseline (≈140 mm Hg), given his extensive coronary artery disease. Epinephrine infusion was initiated during rapid pacing runs to support cardiac output, and intermittent norepinephrine boluses were administered to counteract pacing-induced hypotension.
Transesophageal echocardiography provided continuous assessment of ventricular function and valve deployment. After systemic heparinization with a heparin dose of 80 IU/kg and ACT > 250 s, rapid ventricular pacing at 180 bpm was first employed during balloon valvuloplasty of the failed Sapien 3 frame to minimize movement. A second pacing run then facilitated deployment of the 26 mm Sapien 3 Ultra Resilia valve within the prior prosthesis. Throughout both balloon and valve deployment runs, epinephrine infusion and norepinephrine boluses maintained hemodynamic stability. Post-deployment TEE demonstrated coaxial alignment, full frame expansion, normal leaflet excursion, no thrombus, and trivial central regurgitation without paravalvular leak.
Following successful valve deployment and confirmation of position and function by TEE and aortic root angiography (no paravalvular leak), all sheaths were removed and percutaneous closure achieved. Total procedure time was 110 min (skin-to-skin), fluoroscopy time 14 min, and contrast volume 82 mL of iso-osmolar iodixanol. The patient emerged smoothly from anesthesia, was extubated in the hybrid suite, and was transferred to the cardiac intensive care unit on minimal norepinephrine support. He required no further vasoactive support and was mobilized on postoperative day one. A follow-up echocardiogram confirmed stable valve function, with the new valve demonstrating good leaflet mobility and central flow with mild central transvalvular regurgitation, with measurements consistent with excellent hemodynamic results (Figure 3). The patient was discharged home on postoperative day two in stable condition.
TEE in deep gastric view showing peak transaortic velocity of 2.3 m/sec, consistent with mild aortic stenosis and improved hemodynamics.
Discussion
Redo ViV TAVR presents unique anesthetic challenges due to the combination of advanced age, multiple comorbidities, and mixed aortic valve dysfunction. While monitored anesthesia care with conscious sedation is increasingly employed for primary TAVR in low-risk patients, complex ViV procedures, especially in octogenarians with limited cardiac reserve, often warrant general anesthesia (GA) to facilitate transesophageal echocardiography (TEE) guidance and rapid intervention for hemodynamic instability [6]. Comparative studies suggest that GA may be associated with longer procedural times but affords greater control over airway and hemodynamics, potentially improving safety during rapid ventricular pacing and valve deployment [6,7].
Rapid ventricular pacing (RVP) is integral to both balloon valvuloplasty and valve deployment, as it transiently reduces cardiac output to minimize prosthesis migration. However, RVP induces abrupt hypotension that must be anticipated and managed proactively. In our case, an epinephrine infusion during pacing runs, supplemented by intermittent norepinephrine boluses, stabilized systemic pressures and maintained coronary perfusion in the setting of three-vessel disease [8]. Continuous TEE monitoring allowed real-time assessment of ventricular function and immediate detection of paravalvular leak, guiding fluid and vasoactive therapy [9].
Moreover, implementation of cerebral oximetry monitoring provided additional safety by detecting regional desaturations during hypotensive episodes, which was particularly valuable given the patient’s history of cerebrovascular disease and basilar artery stenosis [10]. The strategy of early extubation and fast-track recovery aligns with enhanced recovery protocols in TAVR and may contribute to shorter ICU stays and earlier mobilization without increasing respiratory complications [11].
Future research should aim to define optimal anesthetic protocols for ViV TAVR, balancing sedation depth, hemodynamic stability, and neuroprotection in patients with high cerebrovascular risk. Multidisciplinary planning remains essential to anticipate procedural risks and streamline perioperative care for these complex cases.
Conclusions
In conclusion, this case shows that redo valve-in-valve TAVR in a frail octogenarian can be completed safely when anesthesia is tightly integrated with detailed pre-procedural imaging. Transthoracic echocardiography and multidetector CT clarified valve sizing, coronary clearance, and procedural risks, while continuous intra-operative TEE and cerebral oximetry guided real-time decisions. An induction sequence using etomidate and fentanyl, followed by low-dose propofol and remifentanil, minimized myocardial depression; baseline norepinephrine with epinephrine supplementation during rapid-pacing runs preserved coronary and cerebral perfusion. These measures maintained hemodynamic stability, allowed extubation in the hybrid suite, reduced postoperative vasoactive requirements, and supported discharge on postoperative day two. Clinicians facing similar redo TAVR cases should emphasize comprehensive imaging, cardiovascularly gentle induction, anticipatory vasoactive therapy timed to pacing, real-time TEE surveillance, and multimodal neuro-monitoring to optimize safety and promote fast-track recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Redo-transcatheter aortic valve replacement procedural optimization and patient selection: from bench to clinical practice J Clin Med Sava RI Garot P Benamer H 14202510.3390/jcm 14082770 PMC 1202793240283600 · doi ↗ · pubmed ↗
- 2Transcatheter valve-in-valve implantation for degenerated bioprosthetic aortic and mitral valves Expert Rev Med Devices Gallo M Dvir D Demertzis S 7497581320162735937210.1080/17434440.2016.1207521 · doi ↗ · pubmed ↗
- 3Anesthetic management for transcatheter aortic valve replacement: a national anesthesia clinical outcomes registry analysis Ann Card Anaesth Hayanga HK Woods KE Thibault DP 29352620233672258510.4103/aca.aca_311_20PMC 9997468 · doi ↗ · pubmed ↗
- 4The effect of anesthesia type on outcomes in patients undergoing transcatheter aortic valve replacement J Cardiothorac Vasc Anesth Abbett SK Urman RD Resor CD Brovman EY 4294353520213302381510.1053/j.jvca.2020.09.083 · doi ↗ · pubmed ↗
- 5Hemodynamic outcomes after valve-in-valve transcatheter aortic valve replacement: a single-center experience Ann Cardiothorac Surg Kherallah RY Koneru S Krajcer Z 6306401020213473369010.21037/acs-2021-tviv-131PMC 8505917 · doi ↗ · pubmed ↗
- 6Monitored anesthesia care versus general anesthesia for transcatheter aortic valve replacement Innovations (Phila) Holmes HR Falasa M Neal D 4014081720223621774810.1177/15569845221124113 · doi ↗ · pubmed ↗
- 7Early clinical and echocardiographic outcomes after SAPIEN 3 transcatheter aortic valve replacement in inoperable, high-risk and intermediate-risk patients with aortic stenosis Eur Heart J Kodali S Thourani VH White J 225222623720162719010110.1093/eurheartj/ehw 112PMC 6392433 · doi ↗ · pubmed ↗
- 8Optimizing anesthetic selection in transcatheter aortic valve replacement: striking a delicate balance between efficacy and minimal intervention Cardiol Res Pract Fadah K Khalafi S Corey M 4217162202420243845491710.1155/2024/4217162 PMC 10919973 · doi ↗ · pubmed ↗