Beyond cytotoxic T cells: reprogrammed regulatory T cells help facilitate response to dual checkpoint blockade
Tullia C. Bruno, Anthony R. Cillo

TL;DR
This study shows that combining two immunotherapies can reprogram immune cells to fight cancer more effectively.
Contribution
The study reveals that regulatory T cells, not just cytotoxic T cells, are key to the success of dual checkpoint blockade.
Findings
LAG3hi tumor models responded to anti-PD1 + anti-LAG3 but not anti-PD1 alone.
CD4+ regulatory T cells reprogrammed to an inflammatory state in response to combination therapy.
Reprogrammed Tregs were linked to better outcomes in patients with metastatic melanoma.
Abstract
Combination immunotherapies have entered the treatment armamentarium of oncology, but important knowledge gaps remain in our understanding of how these therapeutics work. A recent study by Rolig, Peng, and colleagues has shed new light on how dual blockade of PD1 and LAG3 enhances antitumor immunity. The authors first interrogated LAG3 expression on T cells across murine tumor models, classifying the models as LAG3hi or LAG3lo. Next, they found that LAG3hi models were unresponsive to anti‐PD1 alone but responsive to combination therapy with anti‐PD1 + anti‐LAG3. Surprisingly, the response to anti‐PD1 + anti‐LAG3 in LAG3hi models was associated with reprogramming of CD4+ regulatory T cells (Treg) from the canonically immunosuppressive state to an inflammatory state characterized by loss of expression of the transcription factor Foxp3 and upregulation of transcription factor Tbet.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
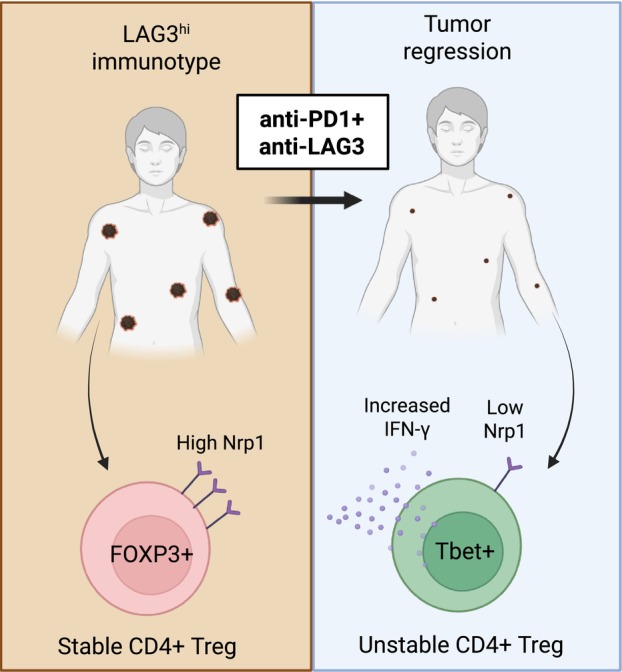 Figure 1
Figure 1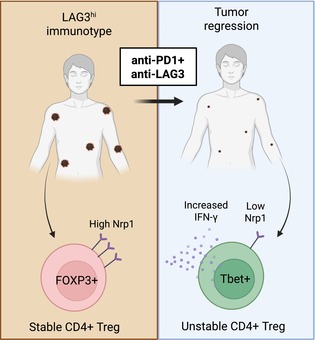 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Cancer Immunotherapy and Biomarkers · Immune Cell Function and Interaction
Immunotherapy (IO) is now routinely used for the treatment of many solid tumors, but not all patients garner a long‐term therapeutic benefit. Thus, combinatorial therapeutics are now being targeted to bolster response rates [1, 2]. Two Food and Drug Administration‐approved regimens that target inhibitory pathways are anti‐PD1/anti‐CTLA4 or anti‐PD1/anti‐LAG3; other regimens and alternative dosing strategies are being actively pursued in various stages of clinical trials. However, despite the strong interest in and clinical efficacy of combination immunotherapies, much remains to be elucidated regarding the biological mechanisms that are associated with clinical benefit in patients. Understanding the mechanisms involved in response and resistance would provide two benefits: (a) insight into the fundamental biology of inhibitory receptor‐mediated suppression of immune function and (b) rational design of optimal combinatorial therapeutic strategies. Ultimately, a better understanding of the mechanisms governing IO response would allow for the development of more efficacious immunotherapeutic strategies.
Rolig, Peng, and colleagues recently added to the growing body of literature on the mechanisms associated with IO response following combination therapy with anti‐PD1 and anti‐LAG3 [3]. This work builds on their previous observation that response to anti‐PD1 monotherapy could be delineated by two peripheral blood immunotypes in patients with urothelial cancer or metastatic melanoma: LAG3^hi^ and LAG3^lo^, with the latter being responsive to anti‐PD1 monotherapy and the former being resistant [4]. To elucidate the mechanisms associated with these immunotypes, the authors evaluated 10 tumor models across two different strains of mice to recapitulate the previously observed human immunotypes. From these studies, mice bearing CT26 and B16F10 tumors resembled the LAG3^hi^ immunotype and those bearing MCA‐205 resembled the LAG3^lo^ immunotype. A key observation surfaced with depletion of either CD8^+^ or CD4^+^ T cells in conjunction with anti‐PD1 + anti‐LAG3 therapy; as expected, depletion of CD8^+^ T cells abrogated the effect of IO, but surprisingly, depletion of CD4^+^ T cells improved survival in the murine CT26 model. This observation suggested that CD4^+^ T cells play a deleterious role in the context of the LAG3^hi^ immunotype and warranted further dissection.
Determining how CD4^+^ T cells contribute to IO resistance was subsequently dissected via interrogation of murine models and patient specimens. Through single‐cell RNAseq experiments and high‐dimensional flow cytometry, responders to combination therapy contained a population of CD4^+^ regulatory T cells (Treg) that upregulated the effector cytokine IFN‐y and the type 1 helper T‐cell‐related transcription factor Tbet with downregulation of Nrp1 (a key driver of Treg stability [5, 6]; Fig. 1). From these data, the authors hypothesized that Treg may be undergoing conversion from stable and suppressive Treg to fragile or ex‐Treg. These Treg states have been described across multiple systems, with stable Treg being the canonical immunosuppressive population, fragile Treg retaining expression of Foxp3 but gaining secretion of IFN‐γ [7], and unstable or ex‐Treg having lost Foxp3 expression entirely and adopted a state similar to conventional helper T cells [8]. Additional experiments were required to identify the Treg state in the responders to combination IO.
To address this question, the authors employed a genetic lineage tracing experiment, where Foxp3 expression was reported by GFP and simultaneously induced permanent expression of YFP. This experiment revealed that a subpopulation of Treg loses Foxp3 expression (that is, are YFP+ GFP–) in mice that respond to combination IO. Previous work has identified a population of Foxp3‐expressing fragile Treg responsible for IO response [7]; this work suggests that simultaneous blockade of LAG3 and PD1 destabilizes Foxp3 expression and leads to ex‐Treg. Finally, the authors performed high‐dimensional flow cytometry in peripheral blood mononuclear cells (PBMC) from a large cohort of metastatic melanoma patients that received anti‐PD1 + anti‐LAG3. Like the mouse model, patients that responded to combination therapy had a subpopulation of Treg with lower FOXP3 MFI and upregulation of Tbet. Overall, the authors found a reprogrammed Treg population that appears to be inflammatory rather than immunosuppressive associated with response to combination IO with anti‐PD1 + anti‐LAG3 in both mice and patients.
The findings from this study prompt several new sets of questions. First, it will be important to assess the degree to which human Treg in the tumor microenvironment mirror the phenotype of tumor infiltrating murine Treg. Second, a potential caveat was the use of subcutaneous tumor inoculation in the murine models, which is associated with differences in antitumor immunity versus orthotopic tumors [9, 10, 11]. Third, these findings build on previous studies in PBMC and suggest that this compartment plays an important role in dictating IO response in a subset of patients. As suggested by the authors, future prospective studies should elucidate whether there are PBMC biomarkers prior to IO that are predictive of initial resistance to anti‐PD1 monotherapy and suggestive of clinical benefit specifically to anti‐PD1 + anti‐LAG3 combination therapy (that is, the LAG3^hi^ immunotype). This prioritization would potentially save patients from being treated with a potentially inefficacious IO and would provide justification for combination therapy and its concomitant increased risk of immune related adverse events. Finally, it would be intriguing to determine whether this LAG3^hi^ immunotype is reflective of patients that will respond to anti‐PD1 + anti‐LAG3 in cancers beyond metastatic melanoma. Identification of a patient population earlier in the disease course that would benefit from combination IO would also be clinically impactful. Overall, Rolig, Peng and colleagues have demonstrated an important role for a population outside of CD8^+^ T cells in response to combination IO, which will help inform future combination IO strategies.
Conflict of interest
TCB serves on the scientific advisory boards of Tabby Therapeutics, Tallac Therapeutics, Galvanize Therapeutics, Mestag Therapeutics, and Kalivir Therapeutics and is a consultant for Galvanize Therapeutics. ARC has no conflicts to declare.
Author contributions
TCB and ARC jointly conceived and wrote this commentary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Larkin J , Chiarion‐Sileni V , Gonzalez R , Grob JJ , Cowey CL , Lao CD , et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373:23–34. 10.1056/NEJ Moa 1504030 26027431 PMC 5698905 · doi ↗ · pubmed ↗
- 2Tawbi HA , Schadendorf D , Lipson EJ , Ascierto PA , Matamala L , Castillo Gutiérrez E , et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386:24–34. 10.1056/NEJ Moa 2109970 34986285 PMC 9844513 · doi ↗ · pubmed ↗
- 3Rolig AS , Peng X , Sturgill ER , Holay N , Kasiewicz M , Mick C , et al. The response to anti‐PD‐1 and anti‐LAG‐3 checkpoint blockade is associated with regulatory T cell reprogramming. Sci Transl Med. 2025;17:eadk 3702. 10.1126/scitranslmed.adk 3702 40203085 PMC 12884954 · doi ↗ · pubmed ↗
- 4Shen R , Postow MA , Adamow M , Arora A , Hannum M , Maher C , et al. LAG‐3 expression on peripheral blood cells identifies patients with poorer outcomes after immune checkpoint blockade. Sci Transl Med. 2021;13:eabf 5107. 10.1126/scitranslmed.abf 5107 34433638 PMC 9254663 · doi ↗ · pubmed ↗
- 5Delgoffe GM , Woo SR , Turnis ME , Gravano DM , Guy C , Overacre AE , et al. Stability and function of regulatory T cells is maintained by a neuropilin‐1‐semaphorin‐4a axis. Nature. 2013;501:252–256. 10.1038/nature 12428 23913274 PMC 3867145 · doi ↗ · pubmed ↗
- 6Chuckran CA , Cillo AR , Moskovitz J , Overacre‐Delgoffe A , Somasundaram AS , Shan F , et al. Prevalence of intratumoral regulatory T cells expressing neuropilin‐1 is associated with poorer outcomes in patients with cancer. Sci Transl Med. 2021;13:eabf 8495. 10.1126/scitranslmed.abf 8495 34878821 PMC 9022491 · doi ↗ · pubmed ↗
- 7Overacre‐Delgoffe AE , Chikina M , Dadey RE , Yano H , Brunazzi EA , Shayan G , et al. Interferon‐gamma drives Treg fragility to promote anti‐tumor immunity. Cell. 2017;169:1130–1141.e 1111. 10.1016/j.cell.2017.05.005 28552348 PMC 5509332 · doi ↗ · pubmed ↗
- 8Zhou X , Bailey‐Bucktrout SL , Jeker LT , Penaranda C , Martínez‐Llordella M , Ashby M , et al. Instability of the transcription factor Foxp 3 leads to the generation of pathogenic memory T cells in vivo. Nat Immunol. 2009;10:1000–1007. 10.1038/ni.1774 19633673 PMC 2729804 · doi ↗ · pubmed ↗