A cross-sectional study of dietary and urinary soy isoflavones about coal-burning fluorosis in Guizhou, China
Hua Han, Yameng Li, Peimin Li, Lu Liu, Xingting Zheng, Yuanmei Zhang, Min Liu, Xiaogang Zhang, Ling Tang, Manman Gao, Na Tao, Jun Liu

TL;DR
This study found that higher dietary intake of soy isoflavones is linked to a lower risk of coal-burning fluorosis in Guizhou, China.
Contribution
The study is the first to show an epidemiological link between soy isoflavones and reduced coal-burning fluorosis risk.
Findings
Higher dietary soy isoflavone intake was associated with a 39% lower risk of fluorosis.
Daidzein, a type of soy isoflavone, showed a similar protective effect.
Urinary soy isoflavone levels mirrored dietary findings, supporting the association.
Abstract
Previous research showed soy isoflavones have antioxidant properties beneficial to bone health, but no epidemiological studies reported effects of soy isoflavones on fluorosis. Therefore, the aim of this study was to investigate the relationship between soy isoflavones in diet/urine and coal-burning fluorosis. A comprehensive cross-sectional study with 896 participants in Zhijin County, Guizhou, China, assessed dietary intake through face-to-face interviews using a 75-item food frequency questionnaire. Urine samples were analyzed for soy isoflavone concentrations by HPLC. Unconditional logistic regression models were used to calculate odds ratios (ORs) and 95% confidence intervals (CIs) for associations. We observed a significant inverse association between dietary soy isoflavones and fluorosis. The adjusted OR (95% CI) in the highest quartile of intake compared with the lowest was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
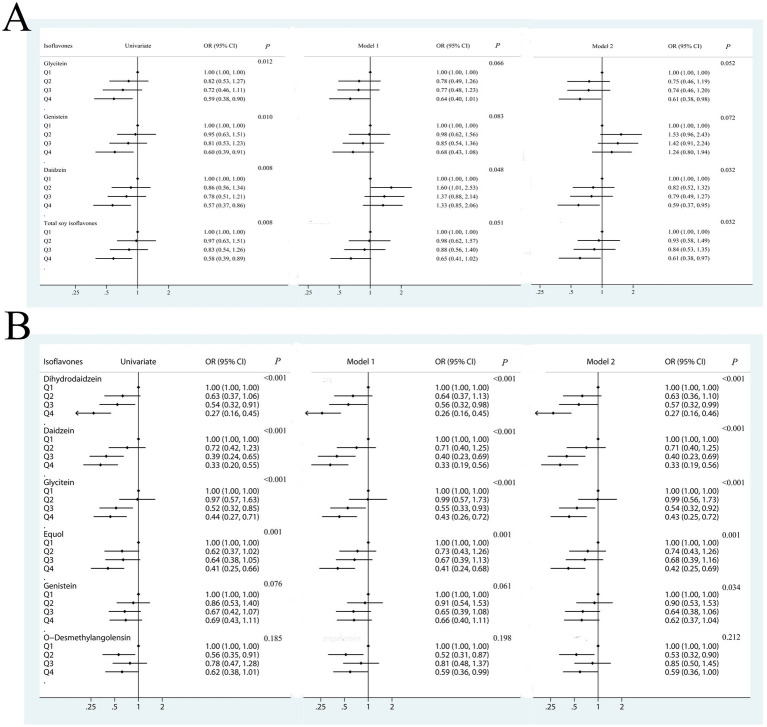 Figure 1
Figure 1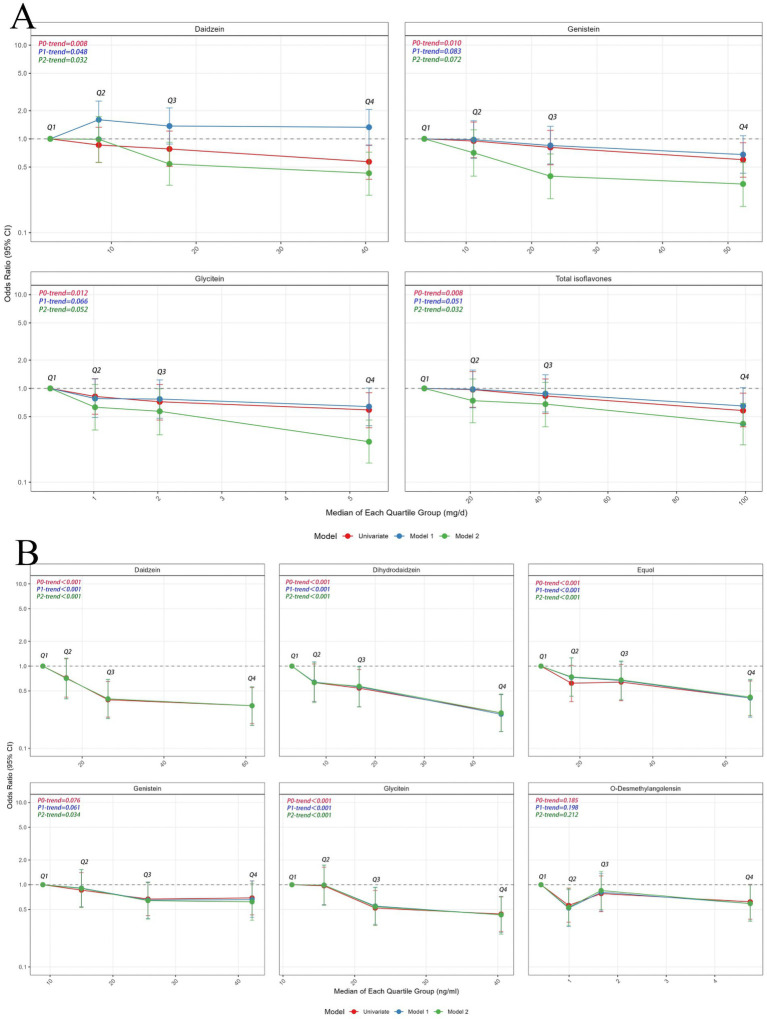 Figure 2
Figure 2| Characteristics | Non-fluorosis ( | Fluorosis ( |
| |
|---|---|---|---|---|
| Age, years (mean ± s) | 47.10 ± 14.52 | 50.32 ± 12.41 | 3.283 | 0.001 |
| Gender, | 2.449 | 0.118 | ||
| Female | 140 (58.09) | 342 (52.21) | ||
| Male | 101 (41.91) | 313 (47.79) | ||
| Marital status, | 4.881 | 0.087 | ||
| Married or cohabitation | 199 (82.60) | 554 (84.60) | ||
| Divorce or separation | 23 (9.50) | 73 (11.10) | ||
| Unmarried | 19 (7.90) | 28 (4.30) | ||
| Educational years, | 60.368 | <0.001 | ||
| ≤3 years | 84 (34.90) | 339 (51.80) | ||
| 4–6 years | 74 (30.70) | 226 (34.50) | ||
| 7–11 years | 55 (22.80) | 76 (11.60) | ||
| ≥12 years | 28 (11.60) | 14 (2.10) | ||
| Income (yuan/per capita/month), | 10.804 | 0.013 | ||
| ≤500 | 9 (3.70) | 62 (9.50) | ||
| 501–2000 | 96 (39.80) | 265 (40.50) | ||
| 2001–4,000 | 64 (26.60) | 178 (27.20) | ||
| >4,000 | 72 (29.90) | 150 (22.90) | ||
| Smoker | 85 (35.30) | 279 (42.60) | 3.920 | 0.048 |
| Alcohol drinker | 73 (30.30) | 204 (31.20) | 0.067 | 0.796 |
| Tea drinker | 90 (37.30) | 250 (38.30) | 0.066 | 0.797 |
| Using an improved stove | 209 (86.70) | 465 (71.30) | 22.554 | <0.001 |
| Fuel type, | 18.301 | <0.001 | ||
| Raw coal | 36 (56.40) | 394 (60.40) | ||
| Mixed coal | 41 (17.00) | 152 (23.30) | ||
| Firewood | 17 (7.10) | 15 (2.30) | ||
| Others | 47 (19.50) | 91 (14.0) | ||
| Using coal to roast grains and chilis | 114 (47.30) | 390 (59.80) | 11.206 | 0.001 |
| Washing dry grains and chilis before use, | 227 (96.20) | 608 (93.80) | 2.905 | 0.234 |
| Total energy intake (kcal/day) | 2538.60 (2008.76, 3210.36) | 2615.86 (1992.06, 3420.85) | 0.737 | 0.461 |
| Calcium intake (mg/day) | 481.91 (335.71, 710.39) | 449.13 (314.42, 655.27) | 1.790 | 0.074 |
| Total protein intake (mg/day) | 72.17 (55.09, 107.84) | 75.47 (54.33, 100.52) | 0.406 | 0.684 |
| Total fat intake (mg/day) | 97.65 (71.94, 147.03) | 101.41 (73.01, 150.86) | 0.567 | 0.571 |
| Corn intake (g/day) | 13.69 (4.72, 28.49) | 13.69 (4.11, 32.87) | 0.286 | 0.775 |
| Dry chilis intake (g/day) | 5.78 (2.41, 12.54) | 5.78 (2.41, 14.46) | 0.537 | 0.591 |
| Urinary fluoride (mg/L) | 1.17 (0.81, 1.65) | 1.41 (1.03, 2.08) | 4.703 | <0.001 |
| Soy isoflavones (mg/day) | 35.39 (16.26, 72.47) | 27.00 (13.82, 55.21) | 2.575 | 0.010 |
| Soy isoflavones | Non-fluorosis group median (25th, 75th) | Fluorosis group median (25th, 75th) |
|
|
|---|---|---|---|---|
| Dietary intake (mg/day) | ||||
| Glycitein | 1.75 (0.87, 3.84) | 1.35 (0.68, 2.87) | 2.771 | 0.006 |
| Genistein | 19.41 (8.84, 39.59) | 14.52 (7.54, 30.69) | 2.580 | 0.010 |
| Daidzein | 14.46 (6.53, 29.03) | 11.26 (5.57, 22.18) | 2.506 | 0.012 |
| Total isoflavones | 35.37 (16.10, 72.22) | 27.38 (13.74, 55.12) | 2.571 | 0.010 |
| Urinary level (ng/mL) | ||||
| Glycitein | 22.78 (14.76, 32.13) | 17.94 (12.84, 26.41) | 4.194 | <0.001 |
| Genistein | 22.75 (12.21, 32.33) | 19.92 (10.99, 31.69) | 1.574 | 0.116 |
| Daidzein | 26.28 (15.82, 44.06) | 18.32 (12.44, 33.09) | 4.956 | <0.001 |
| Dihydrodaidzein | 17.36 (7.01, 39.14) | 9.78 (4.31, 21.36) | 5.167 | <0.001 |
| Equol | 28.57 (16.69, 61.00) | 21.78 (12.03, 39.12) | 3.910 | <0.001 |
| O-Desmethylangolensin | 1.36 (0.79, 2.79) | 1.31 (0.67, 2.30) | 1.230 | 0.219 |
| Soy isoflavones | Quartiles | |||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| Total isoflavones | 0.012 | |||||
| Non-fluorosis/fluorosis | 52/172 | 53/171 | 60/164 | 76/148 | ||
| Female | 1 | 0.95 (0.50, 1.78) | 0.75 (0.40, 1.41) | 0.42 (0.22, 0.80) | 0.017 | |
| Male | 1 | 0.88 (0.42, 1.84) | 0.94 (0.45, 1.99) | 0.84 (0.41, 1.70) | 0.975 | |
| Glycitein | 0.011 | |||||
| Non-fluorosis/fluorosis | 49/175 | 57/167 | 63/161 | 72/152 | ||
| Female | 1 | 0.72 (0.38, 1.38) | 0.82 (0.43, 1.55) | 0.39 (0.20, 0.74) | 0.020 | |
| Male | 1 | 0.74 (0.35, 1.53) | 0.63 (0.30, 1.31) | 0.92 (0.44, 1.91) | 0.987 | |
| Genistein | 0.012 | |||||
| Non-fluorosis/fluorosis | 52/172 | 53/171 | 61/161 | 75/149 | ||
| Female | 1 | 0.93 (0.49, 1.74) | 0.74 (0.40, 1.39) | 0.45 (0.24, 0.86) | 0.030 | |
| Male | 1 | 0.89 (0.42, 1.87) | 0.88 (0.41, 1.85) | 0.89 (0.44, 1.82) | 0.934 | |
| Daidzein | 0.009 | |||||
| Non-fluorosis/fluorosis | 50/174 | 56/168 | 60/164 | 75/149 | ||
| Female | 1 | 0.89 (0.47, 1.69) | 0.70 (0.37, 1.31) | 0.41 (0.21, 0.78) | 0.013 | |
| Male | 1 | 0.74 (0.35, 1.54) | 0.86 (0.40, 1.86) | 0.83 (0.40, 1.69) | 0.916 | |
| Soy isoflavones | Quartiles | |||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| Dihydrodaidzein | 0.109 | |||||
| Non-fluorosis/fluorosis | 29/151 | 42/138 | 47/133 | 74/106 | ||
| Female | 1 | 0.87 (0.40, 1.87) | 0.74 (0.34, 1.59) | 0.28 (0.13, 0.58) | 0.001 | |
| Male | 1 | 0.40 (0.16, 0.95) | 0.37 (0.16, 0.88) | 0.24 (0.10, 0.55) | 0.001 | |
| Daidzein | 0.100 | |||||
| Non-fluorosis/fluorosis | 29/150 | 38/142 | 59/121 | 66/114 | ||
| Female | 1 | 0.62 (0.27, 1.39) | 0.45 (0.20, 1.00) | 0.28 (0.12, 0.61) | 0.003 | |
| Male | 1 | 0.76 (0.32, 1.75) | 0.32 (0.14, 0.71) | 0.38 (0.17, 0.84) | 0.004 | |
| Glycitein | 0.105 | |||||
| Non-fluorosis/fluorosis | 35/ 144 | 36/144 | 57/123 | 64/116 | ||
| Female | 1 | 0.79 (0.37, 1.70) | 0.50 (0.24, 1.06) | 0.44 (0.20, 0.92) | 0.032 | |
| Male | 1 | 1.40 (0.58, 3.39) | 0.58 (0.27, 1.26) | 0.47 (0.22, 0.99) | 0.014 | |
| Equol | 0.308 | |||||
| Non-fluorosis/fluorosis | 33/146 | 48/132 | 47/133 | 64/116 | ||
| Female | 1 | 0.87 (0.42, 1.82) | 0.85 (0.40, 1.77) | 0.55 (0.27, 1.11) | 0.191 | |
| Male | 1 | 0.51 (0.21, 1.21) | 0.44 (0.18, 1.03) | 0.26 (0.11, 0.61) | 0.002 | |
| Genistein | 0.055 | |||||
| Non-fluorosis/fluorosis | 40/ 139 | 45/135 | 54/126 | 53/127 | ||
| Female | 1 | 0.90 (0.43, 1.92) | 0.50 (0.25, 1.02) | 0.59 (0.28, 1.20) | 0.122 | |
| Male | 1 | 0.94 (0.44, 2.00) | 0.90 (0.41, 1.94) | 0.69 (0.32, 1.48) | 0.375 | |
| O-Desmethylangolensin | 0.018 | |||||
| Non-fluorosis/fluorosis | 37/142 | 57/123 | 45/135 | 53/127 | ||
| Female | 1 | 0.58 (0.28, 1.20) | 1.25 (0.60, 2.61) | 0.38 (0.18, 0.79) | 0.154 | |
| Male | 1 | 0.51 (0.23, 1.12) | 0.56 (0.25, 1.28) | 1.01 (0.44, 2.28) | 0.771 | |
| Soy isoflavones | Q1 | Q2 | Q3 | Q4 |
|
|---|---|---|---|---|---|
| Dietary intake (mg/day) | |||||
| Non-DF/DF | 56/168 | 72/152 | 80/144 | 89/135 | |
| Glycitein | 1 | 0.64 (0.41, 1.00) | 0.62 (0.39, 0.96) | 0.52 (0.33, 0.82) | 0.007 |
| Non-DF/DF | 59/165 | 68/156 | 77/147 | 93/131 | |
| Genistein | 1 | 0.79 (0.51, 1.23) | 0.68 (0.43, 1.06) | 0.55 (0.35, 0.85) | 0.007 |
| Non-DF/DF | 58/166 | 70/154 | 76/148 | 93/131 | |
| Daidzein | 1 | 0.74 (0.48, 1.16) | 0.68 (0.43, 1.06) | 0.51 (0.33, 0.80) | 0.004 |
| Non-DF/DF | 59/165 | 68/156 | 76/148 | 94/130 | |
| Total soy isoflavones | 1 | 0.79 (0.50, 1.23) | 0.70 (0.45, 1.10) | 0.51 (0.33, 0.80) | 0.003 |
| Urinary isoflavones (ng/mL) | |||||
| Non-DF/DF | 46/134 | 47/133 | 69/111 | 76/104 | |
| Glycitein | 1 | 0.97 (0.58, 1.62) | 0.56 (0.34, 0.92) | 0.46 (0.28, 0.75) | <0.001 |
| Non-DF/DF | 56/124 | 57/123 | 63/117 | 62/118 | |
| Genistein | 1 | 1.01 (0.62, 1.64) | 0.78 (0.48, 1.26) | 0.78 (0.48, 1.26) | 0.204 |
| Non-DF/DF | 39/141 | 54/126 | 67/113 | 78/102 | |
| Daidzein | 1 | 0.60 (0.36, 1.01) | 0.44 (0.26, 0.74) | 0.34 (0.21, 0.57) | <0.001 |
| Non-DF/DF | 42/138 | 53/127 | 58/122 | 84/96 | |
| Dihydrodaidzein | 1 | 0.73 (0.44, 1.21) | 0.65 (0.39, 1.08) | 0.34 (0.21, 0.56) | <0.001 |
| Non-DF/DF | 46/134 | 57/123 | 60/120 | 75/105 | |
| Equol | 1 | 0.85 (0.51, 1.3) | 0.71 (0.43, 1.17) | 0.48 (0.30, 0.78) | 0.002 |
| Non-DF/DF | 52/128 | 65/115 | 54/126 | 67/113 | |
| O-Desmethylangolensin | 1 | 0.67 (0.42, 1.09) | 1.00 (0.61, 1.63) | 0.67 (0.41, 1.08) | 0.300 |
| Soy isoflavones | Q1 | Q2 | Q3 | Q4 |
|
|---|---|---|---|---|---|
| Dietary intake (mg/day) | |||||
| Non-SF/SF | 124/100 | 137/87 | 159/65 | 154/70 | |
| Glycitein | 1 | 0.75 (0.49, 1.14) | 0.49 (0.31, 0.76) | 0.61 (0.39, 0.95) | 0.007 |
| Non-SF/SF | 121/103 | 143/81 | 156/68 | 154/70 | |
| Genistein | 1 | 0.65 (0.43, 0.99) | 0.51 (0.33, 0.79) | 0.60 (0.39, 0.93) | 0.012 |
| Non-SF/SF | 121/103 | 144/80 | 160/64 | 149/75 | |
| Daidzein | 1 | 0.64 (0.42, 0.97) | 0.47 (0.30, 0.74) | 0.64 (0.42, 0.99) | 0.020 |
| Non-SF/SF | 121/103 | 145/79 | 156/68 | 152/72 | |
| Total soy isoflavones | 1 | 0.61 (0.40, 0.94) | 0.51 (0.33, 0.79) | 0.60 (0.39, 0.93) | 0.015 |
| Urinary isoflavones (ng/mL) | |||||
| Non-SF/SF | 112/68 | 105/75 | 123/57 | 126/54 | |
| Glycitein | 1 | 1.13 (0.71, 1.80) | 0.67 (0.41, 1.08) | 0.66 (0.41, 1.07) | 0.023 |
| Non-SF/SF | 112/68 | 124/56 | 111/69 | 119/61 | |
| Genistein | 1 | 0.86 (0.53, 1.40) | 1.14 (0.72, 1.82) | 0.92 (0.57, 1.48) | 0.951 |
| Non-SF/SF | 108/72 | 105/75 | 117/63 | 136/44 | |
| Daidzein | 1 | 1.10 (0.69, 1.76) | 0.80 (0.49, 1.29) | 0.49 (0.30, 0.80) | 0.002 |
| Non-SF/SF | 97/83 | 115/65 | 119/61 | 134/46 | |
| Dihydrodaidzein | 1 | 0.70 (0.44, 1.12) | 0.68 (0.43, 1.09) | 0.42 (0.26, 0.63) | 0.001 |
| Non-SF/SF | 107/73 | 104/76 | 123/57 | 132/48 | |
| Equol | 1 | 1.11 (0.70, 1.77) | 0.68 (0.42, 1.09) | 0.56 (0.35, 0.91) | 0.005 |
| Non-SF/SF | 112/68 | 120/60 | 116/64 | 118/62 | |
| O-Desmethylangolensn | 1 | 0.83 (0.52, 1.34) | 1.01 (0.63, 1.61) | 0.88 (0.55, 1.41) | 0.806 |
- —National Natural Science Foundation of China10.13039/501100001809
- —Joint Funding of Zunyi Medical University and Zunyi Science and Technology and Big Data Bureau for Scientific and Technological Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFluoride Effects and Removal · Folate and B Vitamins Research · Phytoestrogen effects and research
Introduction
1
Endemic fluorosis is a condition caused by exposure to high concentrations of fluoride in the environment, primarily manifested as dental fluorosis and skeletal fluorosis. Furthermore, in recent years, theories regarding the pathogenesis of systemic damage induced by endemic fluorosis have emerged (1). This condition has a prevalent range that spans across 13 provinces, with a concentration in areas such as Yunnan, Guizhou, and Sichuan, affecting over 34.3 million people and posing as a worldwide public health issue (2, 3). Although the cases of fluorosis from coal-burning have been reduced through the using of improved stoves and awareness education, the prevalence of fluorosis is still high (4–7). Therefore, further prevention and control of fluorosis is needed.
Soy isoflavones are derived from soy foods, a secondary metabolite in the process of soybean growth, which has antioxidant biological activity and can alleviate cellular oxidative stress (8). Studies have shown that soy isoflavones have a protective effect against oxidative stress-related diseases due to their antioxidant activity, in addition to being closely associated with bone health (9, 10). A large number of observational studies have shown that the higher the intake of soy isoflavones, the higher the bone mineral density (BMD) or the lower the bone resorption markers (11). The latest meta-analyses showed that soy isoflavones exert beneficial effects on bone formation markers that can prevent osteoporosis-related bone loss in any weight status or treatment duration (12–14). Isoflavones may benefit bone because they have positive effects on the osteoblast cell (favoring proliferation, differentiation and mineralization) and hinder osteoclast and adipocyte generation (15, 16). Fluorosis is a disease affecting mainly skeletal system and oxidative stress has been considered as an important pathogenesis of endemic fluorosis (17). Based on the positive effects of soy isoflavones on bone health and antioxidant activity, it is suggested that soy isoflavones may have a certain beneficial effect on fluorosis. Furthermore, animal experiments have found that soy isoflavones can inhibit the lipid peroxidation of liver tissue, enhance the antioxidant capacity, and have protective effects on oxidative damage in fluorosis rats (18), but no epidemiological study has confirmed it.
Therefore, we conducted a cross-sectional study to investigate the associations of external (dietary intake) and internal (urine) exposure levels with fluorosis in coal-burning fluorosis areas of Guizhou, China.
Materials and methods
2
Study subjects
2.1
A population-based cross-sectional study was conducted in a coal-burning area of Zhijin County, Guizhou Province, China. We used a two-stage, clustered random sampling method to ensure the representativeness of the target population. The three towns of Chadian, Chengguan, and Puweng were randomly selected from 10 towns in Zhijin County. Then, we randomly further selected four villages from each selected town. The 12 villages selected for the study were Dazai, Ganhe, Gaofeng, Guihua, Guohua, Hehua, Hualuo, Jiangyan, Moda, Shangzai, Yutang, and Xianfeng. Participants who have lived in Zhijin County for at least 10 years and aged 18–75 years were recruited. Participants were excluded if they had a prior history of cancer, coronary heart disease, stroke, gout, or kidney disease. They were also excluded if their dietary habits had manifestly changed during the previous 5 years, or if they had chronic diseases that might affect their dietary habits, such as gastritis, diabetes, and hypertension. In addition, the participants with incomplete questionnaire information were also excluded. Finally, a total of 896 participants were successfully interviewed out of 1,101 recruited. The urine samples of 720 subjects were obtained from the 896 participants interviewed. It was reported the prevalence of coal-burning fluorosis in Guizhou was 35% (19), allowable error d = 0.15p, and significance level α = 0.05; . The sample size was estimated to be 318 cases based on the sample size estimation formula for cross-sectional studies.
All of the coal-burning fluorosis cases were diagnosed by the Zhijin County Disease Control and Prevention Center according to the Chinese Diagnostic Criteria of Dental Fluorosis (WS/T208-2011, China) and the Chinese Diagnostic Criteria of Endemic Skeletal Fluorosis (WS/T 192-2008, China) (20). Specifically, dental fluorosis was confirmed in individuals with a documented history of excessive fluoride exposure during tooth development, presenting with at least one enamel defect: white non-removable opacities, intrinsic brown/black-brown discoloration, or pitted/map-like hypoplasia. Similarly, skeletal fluorosis was diagnosed in individuals with a documented history of residence in an endemic fluorosis area, presenting with persistent resting pain in ≥3 bony/joint sites (unaffected by weather), joint limitation/neurological deficits (limb deformities, paralysis). Dental fluorosis and skeletal fluorosis were identified by a professional doctor in Zhijin Center for Disease Control and Prevention. Concurrently, non-fluorosis was defined as the absence of pathological changes in individuals, such as dental fluorosis or skeletal fluorosis, despite long-term living in fluorosis area.
This study complied with the Declaration of Helsinki guidelines and was approved by the Zunyi Medical University Medical Ethics Committee (No. 2014-1-003), with all participants providing written informed consent. Using cluster sampling of villages in coal-burning fluorosis-endemic areas, we ensured comprehensive representation of the target population. This approach, combined with a broad age range, redundant sample size, and standardized diagnostics, effectively mitigated selection bias.
Data collection pertaining to diet and lifestyle
2.2
Interviews were conducted by trained interviewers who administered a structured questionnaire in a personal interview. The content of the questionnaire included: (1) socio-demographic characteristics (age, gender, ethnicity, marital status, and education level); (2) lifestyle habits (use of improved stoves, domestic fuel type, use of coal to roast grains and chilies, and washing dry grains and chilies before use); (3) dietary habits in the year before the interview; (4) relevant disease history (hypertension, diabetes, gout, hepatocirrhosis, heart-related diseases). Dietary intake of nutrients intake was collected through a valid and reliable Food-Frequency Questionnaire (FFQ) (21) and assessed never, daily, weekly, monthly, or yearly frequency intake of each food item over the last year. The 75-items FFQ involved seven categories including fruits, animal food, cereals, beans and their products, vegetables, algae and nuts, drinks and soup. The FFQ covered virtually all soy foods that are habitual consumed in the study population, including firm tofu, soft tofu, bean curd skin, soy drink, tofu pudding and fresh and dried soybeans. Energy, soy isoflavones, genistein, daidzein and glycitein and other nutrient intakes were calculated using the Chinese Food Composition Database (22).
Detection of urinary levels of soy isoflavones
2.3
Level of glycitein, genistein, daidzein, dihydrodaidzein, equol, and O-desmethylangolensin in the urine were detected using a high-performance liquid chromatography (HPLC) methods. Briefly, Urine samples were extracted by ethyl acetate after deconjugation by β-glucuronidase/sodium acetate. After nitrogen drying, the extract was reconstituted in mobile phase solution for analysis. The HPLC system consisted of a C18 stationary phase extraction (5 μm, 4.60 mm × 250 mm) column, and separation of soy isoflavones was achieved by gradient elution with the mobile phase of methanol-ethyl acetate at a flow rate of 1.0 mL/min. Soy isoflavones were detected from the UV absorbance at 254 nm. The standards of glycitein, genistein, daidzein, dihydrodaidzein, equol, O-desmethylangolensin and β-glucuronidase were purchased from Sigma Chemical Company (St. Louis, MO, United States).
Statistical analysis
2.4
The data were coded and doubly entered by two data clerks into Epi-Data version 3.1 to avoid clerical errors using side-by-side comparison, and the data were then exported to SPSS for windows version 18 statistical software.
Continuous variables were expressed as mean (M) and SD (s) or median (P25, P75), while categorical variables were expressed as numbers and percentages. Dietary intake of soy isoflavones showed skewed distribution, which was classified into quartiles, and the lowest quartile was used as the reference category. Logistic regression model was used to estimate the relationship between dietary intake of soy isoflavones and coal-burning fluorosis, and the odds ratio (OR) and 95% confidence interval (95% CI) were calculated. The multivariate models were used to adjust the potential confounding factors, such as age, gender, ethnicity, marital status, education level, smoking, alcohol drinking, tea drinking, improved stove use, fuel type and using coal to roast grains and chilies, washing dry grains and chilies before use (Model 1). Subsequent models were adjusted for dietary factors, such as roasted chili consumption, dietary calcium intake, total energy intake, and roasted corn intake (Model 2). Stratified analysis was performed by sex (male/female) to explore whether the association between soy isoflavones and fluorosis was modified. Subgroup analyses for dental fluorosis or skeletal fluorosis were performed for the relationships between soy isoflavones and fluorosis. We also performed sensitivity analysis to assess whether the results of primary analysis were driven by type of fluorosis. All p-values were two tailed, and the level of significance was set at ≤ 0.05.
Results
3
General characteristics of subjects
3.1
Of the 896 participants (414 men and 482 women), 655 were diagnosed with endemic fluorosis and 241 without fluorosis. Table 1 shows the baseline demographic characteristics of the study subjects and selected risk factors for endemic fluorosis. The mean (±) age of fluorosis group was 50.32 years old (±12.41 years old), and that of non-fluorosis group was 47.10 years old (±14.52 years old). Compared with non-fluorosis subjects, fluorosis patients tended to have lower levels of education and annual household income. Moreover, fluorosis patients were less likely to use improved cook stoves, were more likely to use coal to roast grains and chilis, and use mixed coal fuel types. Compared with non-fluorosis subjects, the intake of soy isoflavone in fluorosis patients was lower, and the level of urinary fluoride was higher.
Comparison of dietary and urinary isoflavones in participants with fluorosis and non-fluorosis
3.2
Compared with fluorosis patients, the dietary intake of soy isoflavones was higher in non-fluorosis subjects, and the intake of genistein was the largest in the subclass of soy isoflavones. In addition, compared with fluorosis patients, the contents of soy isoflavone and daidzein metabolites in urine of non-fluorinated subjects were higher, and equol content was the highest in urine (Table 2).
Associations between dietary soy isoflavones and coal-burning fluorosis
3.3
Figure 1A presents the ORs and 95% CIs for fluorosis according to quartiles of dietary soy isoflavone intakes. The quartiles of dietary intake of soy isoflavones from low to high were 6.64 mg/day, 20.72 mg/day, 41.84 mg/day, 99.29 mg/day. With the increase of intake, the proportion of non-fluorosis poisoning increased. Univariate analysis showed that the OR value decreased gradually with the increase of nutrient intake, and the difference between the highest quartile and the lowest quartile of nutrient intake was statistically significant (p = 0.008). After further adjustment for dietary factors such as total energy, calcium intake, grains intake, and dry chilis intake, the negative associations between soy isoflavone intake and the risk of developing coal-burning fluorosis were not changed. The ORs for fluorosis occurrence in the highest quartile compared with the lowest quartile of intake 0.59 (95% CI: 0.37–0.95) for daidzein, 0.61 (95% CI: 0.38–0.97) for total soy isoflavones. Figure 2A indicates the higher dietary intake of daidzein and total isoflavones, the lower the occurrence of fluorosis (both p-trend = 0.032).
Odds ratios (ORs) and 95% CIs of fluorosis for quartiles of soy isoflavones. (A) ORs and 95% CIs of fluorosis for quartiles of dietary intake of soy isoflavones. (B) ORs and 95% CIs of fluorosis for quartiles of urinary level of soy isoflavones. OR, odds ratio; CI, confidence interval. Quartile 1 was the reference quartile. The multivariate logistic regression model was used to estimate the association between dietary intake of soy isoflavones and fluorosis. Model 1: OR was adjusted for covariates, such as age, sex, marital status, education level, income, smoking status, alcohol drinking status, tea drinking status, using coal to roast grains or chili, washing dry grains or chili before use, fuel type, and using improved stove. Model 2: OR was adjusted for the various above confounders and calcium intake, roasted chili and grains consumption, and total energy intake.
Dose–response relationship plots for soy isoflavone and occurrence of fluorosis. (A) Dose–response relationship plots for dietary of soy isoflavone and occurrence of fluorosis. (B) Dose–response relationship plots for urinary level of soy isoflavone and occurrence of fluorosis. CI, confidence interval. Q, quartile. Q1–Q4 represent four equal groups of dietary soy isoflavone intake (Q1 = lowest to Q4 = highest) and their medians. p-trend: test the dose–response trend between isoflavone intake and fluorosis risk. Univariate (red plot): univariate model: no covariates were adjusted. Model 1 (blue plot) adjusted for age, sex, marital status, education level, income, smoking status, alcohol drinking status, tea drinking status, using coal to roast grains or chili, washing dry grains or chili before use, fuel type, and using improved stove. Model 2 (green plot) adjusted for the various above confounders and calcium intake, roasted chili and grains consumption, and total energy intake.
Associations between urinary soy isoflavones and coal-burning fluorosis
3.4
For the six soy isoflavone subgroups, compared to the lowest quartile of urinary isoflavone, the ORs for fluorosis occurrence in the highest quartile were 0.27 (95% CI: 0.16–0.0.46) for dihydrodaidzein, 0.33 (95% CI: 0.19–0.56) for daidzein, 0.43 (95% CI: 0.25–0.72) for glycitein and 0.42 (95% CI: 0.25–0.69) for equol (Figure 1B). Figure 2B shows the higher levels of dihydrodaidzein, daidzein, glycitein and equol in the urine, the lower the occurrence of fluorosis after adjusting for various dietary and non-dietary factors (p-trend <0.001–0.034). In contrast, no statistical association was observed between O-desmethylangolensin and fluorosis (p-trend = 0.666).
Sex-stratified analysis of the relationship between soy isoflavone and coal-burning fluorosis
3.5
As shown in Table 3 subgroup analysis showed there were negative associations of total soy isoflavones, glycitein, genistein and daidzein with fluorosis in women (p = 0.013–0.030), but not in men. We observed interactions between dietary soy isoflavone and gender on fluorosis, such as daidzein (p-interaction = 0.009), genistein (p-interaction = 0.012), glycitein (p-interaction = 0.011), total isoflavones (p-interaction = 0.012). Furthermore, there were interactions between urinary O-desmethylangolensin and fluorosis (p-interaction = 0.018) (Table 4 and Supplementary Figure 1). These results indicated effects of different types of soy isoflavones on fluorosis may be vary between men and women.
Multivariate analysis of soy isoflavone and dental fluorosis and skeletal fluorosis
3.6
Fluorosis was divided into dental fluorosis and skeletal fluorosis, thus sensitivity analysis was conducted to assess whether the results of primary analysis were driven by type of fluorosis. Results showed associations of dietary intake and urinary levels of soy isoflavone with dental fluorosis and skeletal fluorosis were in line with fluorosis (Tables 5, 6).
Discussion
4
Summary of main findings
4.1
To the best of our knowledge, we firstly assessed the association of soy isoflavones with fluorosis. We observed that dietary intake of soy isoflavones, glycitein, daidzein and genistein were negatively associated with fluorosis. Additionally, the higher the urinary level of glycitein, daidzein, dihydrodaidzein and equol, were associated a lower occurrence of coal-burning fluorosis. Biomarkers are invaluable for providing objective, precise, and biologically relevant measures of nutrient status. Urinary isoflavone levels reflect metabolic processing and excretion, not merely dietary intake. Inter-individual metabolic differences must be considered, as they substantially influence urinary levels. However, the assessment of dietary soy isoflavones through FFQ can reflect the dietary levels of long-term habits, which is very important for exploring the relationship between dietary isoflavone and disease. In the present study, we investigated both dietary and urinary exposure of soy isoflavones, and we found both internal and external exposure levels of soy isoflavones was negatively associated the occurrence of fluorosis. These rigorous findings suggested that higher exposure level of soy isoflavones is associated with the lower the risk of coal-burning fluorosis. An experimental animal study on the effects of multi-nutrient intervention in coal-burning fluorosis on dental fluorosis, bone fluoride and urinary fluoride in female rats suggested that multi-element plus soy intervention resulted in lower bone fluoride levels (23). This may be attributed to the fact that soy foods are rich in soy isoflavones. A five-year cohort study (n = 1,587) found a 1.95% reduction in bone mineral density (BMD) and a 69% increased risk of osteoporosis (95% CI: 1.09, 2.61) in the lowest group compared to the highest quartile of soy isoflavones (≥62.64 mg/day) (24). In addition, studies have shown that increasing the intake of soy products, soy protein or soy isoflavones can improve bone resorption or reduce bone loss (14, 25). A recent meta-analysis of 26 randomized controlled trials (n = 2,652) also found that supplementation of soy isoflavones had a strong beneficial effect on estrogen deficient bone loss in women (26), and intervention of soy isoflavones can effectively improve lumbar spine and total femur bone mineral density in women (27, 28). Therefore, both observational and interventional studies have shown that soy isoflavones have beneficial effects on bone health. In this study, dietary and urinary soy isoflavones were found to be negatively correlated with fluorosis, which proves that the beneficial effects of soy isoflavones on bone health may antagonize the effects of fluorosis on bone injury. It is acknowledged that urinary isoflavone levels reflect metabolic processes and excretion rather than intake alone, and inter-individual metabolic variations affect these levels, which will be addressed in future studies.
Explanation of biological mechanisms
4.2
Excessive fluoride induces oxidative stress in bone tissues by increasing the content of reactive oxygen species (ROS) and lipid peroxides (MDA) in bone tissues and reducing the activity of antioxidant enzymes (20, 29). Although oxidative stress indicators were not directly measured, the antioxidant properties of isoflavones allow us to infer that they alleviate fluorosis by reducing oxidative stress damage. Soy isoflavones can affect fluorosis through their antioxidant properties because they are well-documented antioxidant substances. In recent years, studies have shown that soy isoflavones significantly elevated total antioxidant capacity and superoxide dismutase enzyme activities, decreased malondialdehyde level, promoting antioxidant element nuclear erythroid-2-related factor 2, and its downstream targets, including heme oxygenase 1, and quinone oxidoreductase 1 protein expressions (30). Furthermore, isoflavones can enhance bone formation and inhibit bone resorption by influencing the cell signaling pathways of osteoblast and osteoclast differentiation, including the Wnt-β-catenin and BMP pathways that stimulate bone formation (31). In addition, studies have shown that soy isoflavones are phytoestrogens with physiological functions such as preventing osteoporosis, increasing bone density and bone strength in rats with osteoporotic fractures, promoting the expression of vascular endothelial growth factor and osteoprotegerin at the fracture end, improving the histological environment, and promoting the healing of osteoporotic fractures (32, 33). Notably, although we detected dietary and urinary soy isoflavones and used multivariate analyses to demonstrate negative association, we did not measure urinary bone turnover markers, limiting direct evidence for bone health conclusions. Overall, the negative associations between soy isoflavones and fluorosis may be justified based on the fact that they act as antioxidants to reduce oxidative stress damage and have a positive effect on fluorosis. However, further studies are needed to elucidate the pathophysiological mechanism.
Gender-specific associations and the role of estrogen
4.3
In this study, stratified analysis showed soy isoflavones may be inversely associated with fluorosis in women, but not in men, indicating associations between soy isoflavones and fluorosis may be modified by gender. Some related studies have shown that the reduction of BMD loss by soy protein is mainly due to the phytoestrogenic effects of soy isoflavones (34, 35). A clinical study has shown that soy isoflavones can improve bone mineral density and prevent bone calcium loss in postmenopausal women, and soy isoflavones can also significantly slow down the bone turnover rate in postmenopausal women, which is beneficial to maintaining the dynamic balance of bone resorption-bone formation, and has the effect of preventing and treating osteoporosis in postmenopausal women (36). Sex-specific associations were also observed in other studies, such as colorectal cancer (37) and type 2 diabetes (38). The bases for the sex-specific effects may be soy isoflavones have at least two hydroxyl functions in opposite positions on the molecule, which mimics effect of estradiol. This may be attributed to the interaction between estrogen receptor expression levels in women and the phytoestrogenic effects of the isoflavones. Isoflavones not only act as weak estrogens but also compete with endogenous estrogen for binding to the estrogen receptor (39). ERα activates intracellular phosphorylation pathways including PI3K/Akt and NF-κB and exerting its biological effect (40). Additionally, menopausal status as a potentially important confounder in interpreting sex-specific findings. Postmenopausal women experience estrogen decline, whereas studies have demonstrated that soy isoflavone supplementation improves menopausal symptoms and postmenopausal bone health (41–43). Thus, postmenopausal estrogen decline can be partially offset by soy isoflavones acting as phytoestrogens. However, it was regrettable that we did not collect this status due to the estrogen levels of women gradually decrease after menopause. Future epidemiological studies need to determine whether estrogen biomarkers or menopausal status affect the effects of soy isoflavones on fluorosis risk.
Study limitations and directions for future research
4.4
Although this study has built upon existing literature, it is not without limitations. First, the cross-sectional design inherently restricts our ability to establish a causal relationship between isoflavones and fluorosis. However, we implemented stringent inclusion and exclusion criteria during participant recruitment to mitigate potential reverse causality to some extent. Second, while the Food Frequency Questionnaire (FFQ) may introduce measurement errors, the questionnaire utilized in this study has been validated, and we conducted a multifactorial analysis to minimize the influence of these errors on our findings. Third, although patients diagnosed with fluorosis may alter their dietary habits, such changes do not result in misclassification of their fluorosis status, allowing for some degree of generalizability of our results. Fourth, gender-stratified analysis was conducted, female menopausal status was not stratified due to we did not collect menopausal status during the investigation. Potential hormonal influences on the observed relationships was not explored. Future studies should collect data on menopausal status to clarify hormone-related effects. Additionally, we did not measure urinary bone turnover markers, limiting direct evidence for bone health conclusions. Finally, although we adjusted for major sociodemographic characteristics, lifestyle factors, dietary factors, confounding by unknown or unmeasured factors cannot be completely ruled out, such as hormonal level, bone turnover markers. Future research should focus on these issues. (1) Individual metabolic variations affect urinary soy isoflavone levels, how do metabolism-related gene polymorphisms affect the association between soy isoflavones and fluorosis? (2) How do menopausal status or hormone levels affect the association between soy isoflavones and fluorosis? (3) How do bone turnover markers affect the association between soy isoflavones and fluorosis? Therefore, In the future, large-scale prospective studies should be carried out to collect menopausal status, detect levels of hormone and bone turnover marker, and determine gene of the metabolic pathway and bone turnover, in order to clarify their roles in the relationship between soy isoflavones and fluorosis. Moreover, further studies are needed to elucidate the pathophysiological mechanism by animal intervention experiments.
Conclusion
5
The higher exposure level of soy isoflavones is associated with the lower the risk of coal-burning fluorosis. The study provides evidence-based support for developing dietary recommendations incorporating soy isoflavones to help reduce fluorosis risk in endemic areas. Thus, we advocate increasing dietary soy isoflavone intake, particularly in coal-burning fluorosis areas. Food manufacturers should develop high-isoflavone fortified foods for high-risk population. Multi-sectoral collaboration is needed to implement prevention strategies at the grassroots level, complemented by health education to enhance public self-protection awareness.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zeng A Li H Hu X Yang M Mu M Chen Y. Fibroma development in rats with dental fluorosis: activation pathways of endoplasmic reticulum stress and mitochondria. J Zunyi Med Univ. (2021) 44:433–9. doi: 10.14169/j.cnki.zunyixuebao.2021.0071 · doi ↗
- 2Zhou J Sun D Wei W. Necessity to pay attention to the effects of low fluoride on human health: an overview of skeletal and non-skeletal damages in epidemiologic investigations and laboratory studies. Biol Trace Elem Res. (2023) 201:1627–38. doi: 10.1007/s 12011-022-03302-7, PMID: 35661326 · doi ↗ · pubmed ↗
- 3Guan Z Wu C Qi X. Evaluation of the health status of the population in coal fired fluorosis areas in Guizhou Province after comprehensive management. J Guizhou Med Univ. (2018) 43:1124–8. doi: 10.19367/j.cnki.1000-2707.2018.10.001 · doi ↗
- 4Fan S. The current situation of endemic fluorosis prevention and control in China during the 13th five-year plan period. OEM. (2020) 37:1219–23. doi: 10.13213/j.cnki.jeom.2020.20274 · doi ↗
- 5Wang X Gao J Li C Song L Zhang X Pan X. Changes of fluorine exposure level of population in endemic fluorosis areas caused by coal burning in Guizhou Province. E&H. (2020) 37:620–2. doi: 10.16241/j.cnki.1001-5914.2020.07.012 · doi ↗
- 6Wang M Shen H Chen X Li Y Zhou X La C. Meta-analysis on the effectiveness of health education interventions for endemic fluorosis in China. CJCED: Chin J Control Endem Dis. (2024) 39:16–9.
- 7Jianyang G Hongchen W Zhiqi Z Jingfu W Haiqing L. Review on health impacts from domestic coal burning: emphasis on endemic fluorosis in Guizhou province, Southwest China. RECT. (2021):258. doi: 10.1007/398_2021_7134625836 · doi ↗ · pubmed ↗
- 8Huo X Wang S Chen Z. Effect of soy isoflavones on oxidative hydrogen peroxide-induced stress in IPEC-J 2 cells. CJAVS: Guangdong J Anim Vet Sci. (2021) 46:37–40.