Endoscopic Removal of Impacted Barium Stools Using a Snare and a Long Hood: A Rare Complication Following Upper Gastrointestinal Barium X‐ray Radiography (With Video)
Takaaki Kishino, Naoki Okamoto, Kohei Fukumoto

TL;DR
A rare case of bowel blockage from barium contrast was successfully treated with endoscopic removal, avoiding surgery.
Contribution
Demonstrates endoscopic treatment as an effective alternative to surgery for barium impaction.
Findings
Endoscopic removal using a snare and long hood successfully treated colonic obstruction from barium impaction.
No serious complications like bowel perforation occurred during the procedure.
Highlights the importance of patient awareness and prompt medical attention for such rare complications.
Abstract
Barium sulfate is widely used as a radiographic contrast medium in upper gastrointestinal barium X‐ray radiography for cancer screening in Japan. Although generally considered safe, rare complications such as bowel obstruction due to impacted barium stools can occur. We report the case of a healthy 41‐year‐old woman who developed colonic obstruction following upper gastrointestinal barium X‐ray radiography. Endoscopic treatment was attempted using a snare and a long hood to fragment and remove the barium mass. The impacted stools were successfully removed endoscopically, and there were no serious complications such as bowel perforation or generalized peritonitis that would require surgery. This case demonstrates that endoscopic removal can be an effective and less invasive treatment option for barium impaction, which carries a risk of requiring surgical intervention. Although patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
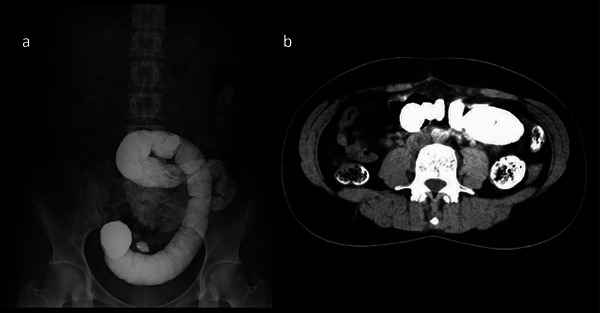 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2 FIGURE 3
FIGURE 3| Reference | Year | Sex | Age | Comorbidities/Medical history | Time from barium study to onset | Clinical presentation | Site of obstruction | Endoscopic devices used | Endoscopic outcome | Additional treatment | Clinical outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cheney [1] | 1994 | Male | 69 | End‐stage renal disease on dialysis | 3 days | Abdominal pain with distension and vomiting | Descending colon | Water irrigation and snare | Unsuccessful | Water irrigation via a decompression tube | Recovery |
| McDonnell [2] | 1997 | Female | 54 | Lung cancer; Billroth II gastric resection | 10 days | Diffuse abdominal tenderness, but no peritoneal signs | Sigmoid colon | Not recorded | Unsuccessful | Sigmoid colectomy with a Hartmann's procedure for perforation | Recovery |
| Kurer [3] | 2007 | Female | 64 | Ulcerative colitis | 9 months | Abdominal pain | Descending colon | Water‐jet | Successful | None | Recovery |
| Thosani [4] | 2014 | Female | 39 | Scleroderma | 7 days | Nausea, vomiting, abdominal pain, and obstipation | Sigmoid colon | Water‐jet and biopsy forceps | Successful | None | Recovery |
| Shaughnessy [5] | 2015 | Female | 86 | Billroth II gastric resection | 1 week | Diffuse abdominal pain and distension; septic shock | Descending colon | Not recorded | Unsuccessful | Total colectomy with end‐ileostomy | Recovery |
| Iida [6] | 2017 | Female | 45 | Chronic constipation | 7 days | Lower abdominal pain without peritoneal signs | Sigmoid colon | Water‐jet, net, and snare | Successful | None | Recovery |
| Vieiro [7] | 2023 | Female | 62 | Not recorded | Not recorded | Abdominal pain, nausea, and constipation | Descending colon | Water irrigation and snare | Successful | None | Recovery |
| Sharpe [8] | 2024 | Female | 67 | Diabetes mellitus; Schizoaffective disorder | Not recorded | Diffuse abdominal tenderness with guarding | Sigmoid colon | Not recorded | Unsuccessful | Left colectomy with Hartmann's procedure for sigmoid colon perforation | Recovery |
| This case | 2025 | Female | 41 | Open appendectomy; Cesarean section | 7 days | Severe lower abdominal pain; tenderness without peritonitis | Sigmoid colon | Water‐jet, long hood, and snare | Successful | None | Recovery |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Foreign Body Medical Cases · Appendicitis Diagnosis and Management
Introduction
1
Barium sulfate is a commonly used radiographic contrast medium in examinations for gastrointestinal diseases, including in population‐based gastric cancer screening programs in Japan [1]. The incidence of complications in a barium study is low [1, 2], but rare complications have been reported, including intestinal obstruction [3, 4, 5, 6, 7, 8] and subsequent perforation [3, 4, 5] caused by impaction of barium stools (barolith). The Japanese Society of Gastrointestinal Cancer Screening (JSGCS) has conducted a national survey on complications associated with upper gastrointestinal barium X‐ray radiography screening. In the 2021 survey, bowel obstruction was reported in three cases out of 3,077,580 screenings, and intestinal perforation in two cases [9].
A barolith is a dense, hard mass formed from inspissated barium mixed with feces and can lead to intestinal obstruction [7]. When conservative management fails, surgical intervention is often necessary [2, 3, 6, 8, 10], and there are reports of fatal complications such as intestinal perforation [3]. However, endoscopic management is not well established, and reports in the literature remain scarce. Here, we present a case in which impacted barium stools were endoscopically removed in a healthy woman, thereby avoiding surgical intervention.
Case Report
2
A healthy 41‐year‐old woman underwent an upper gastrointestinal barium X‐ray radiography as part of routine cancer screening. She had a past medical history of open abdominal surgery for appendicitis at age 6 and a Cesarean section at age 28. Other than these, she had no significant medical history and no tendency toward constipation. She passed a small amount of stool the day after the procedure, but subsequently developed constipation. Seven days later, she presented to our hospital with severe lower abdominal pain. On admission, her vital signs were as follows: body temperature, 35.8°C; blood pressure, 112/53 mmHg; and pulse rate, 64 bpm. Physical examination revealed abdominal distension and tenderness without peritoneal signs. Surgical scars were observed in the right lower abdomen and lower midline region. Blood test results on admission revealed mild anemia, with a hemoglobin level of 10.6 g/dL and a hematocrit of 33.9%. However, inflammatory markers were not elevated; the white blood cell count was 8.21×10^9^/L, and C‐reactive protein was 0.01 mg/dL. No other significant abnormalities were noted in the remaining laboratory parameters (Table S1).
Abdominal X‐ray and contrast‐enhanced computed tomography revealed a large amount of retained barium in the sigmoid colon with no evidence of free air (Figure 1). Due to the risk of perforation or generalized peritonitis from increasing intraluminal pressure, we performed an urgent colonoscopy to remove the barium impaction without prior bowel preparation.
Abdominal X‐ray and contrast‐enhanced computed tomography revealed a large amount of retained barium in the sigmoid colon without evidence of free air. (a) Abdominal X‐ray, (b) Abdominal computed tomography.
The colonoscopy was performed using a water‐jet colonoscope (PCF‐Q260AZI; Olympus) fitted with a long hood (MAJ‐663, Olympus; outer diameter 15.8 mm) (Figure 2a,b). The barium stools were found to be impacted at a sharp bend in the sigmoid colon. We used a 25‐mm snare (Snare Master [SD‐210U‐25], Olympus; Figure 2c) to mechanically fragment the mass, which was then suctioned into the hood cup and removed (Video S1). The long hood, which has no side holes, allowed for effective suction of the barium debris with strong negative pressure.
(a) A long hood (distal attachment, MAJ‐663; Olympus). (b) A water‐jet scope (PCF‐Q260AZI; Olympus) with the long hood. (c) A snare with a loop diameter of 25 mm (Snare Master [SD‐210U‐25]; Olympus).
By repeatedly fragmenting and suctioning the stools, most of the impaction was cleared in approximately 60 min. Endoscopic observation confirmed that the obstruction was resolved, and the lumen was adequately decompressed, although some residual barium remained (Figure 3). It also revealed no significant bowel narrowing or stiffness in the sigmoid colon, suggestive of adhesions. The patient's abdominal pain improved immediately post‐procedure. However, she developed localized peritonitis in the left lower quadrant the next day, characterized by tenderness with localized peritoneal signs and elevated inflammatory markers in blood tests (white blood cell count: 18.08 × 10^9^/L and C‐reactive protein: 10.2 mg/dL) (Table S1). Abdominal X‐ray showed no free air. Based on the clinical course, we diagnosed localized peritonitis secondary to ischemic colitis due to bowel obstruction. She was managed conservatively with antibiotics. She recovered without further complications and was discharged on day 5 of hospitalization.
Abdominal X‐ray after treatment.
Discussion
3
Barium‐induced colonic obstruction is rare [2]. In a systematic review conducted by Kurer et al., only 31 patients with barolith impaction were identified between 1950 and 2006. According to this review, in cases where the site of obstruction was specified, more than half occurred in the left colon (i.e., the descending or sigmoid colon). This may be attributed to the narrowing of the colonic lumen as it progresses distally, allowing baroliths to accumulate as barium mixes with intestinal contents. Barium‐induced colonic obstruction is usually reported in elderly or bedridden patients with underlying bowel motility disorders [2, 8]. However, this case demonstrates that this complication can occur even in healthy individuals with no history of constipation but a history of open abdominal surgery.
For treatment, conservative management such as fasting, laxatives, or enemas is generally the first‐line approach [7]. If ineffective, or if complications such as perforation or generalized peritonitis are present, surgical interventions such as colectomy or colostomy are considered [3, 4, 5]. According to the aforementioned systematic review, approximately one‐third of the reported cases (11/31) were successfully managed with conservative measures, including the use of laxatives. Notably, surgery was required in nearly half of the patients (14/31). Even more interestingly, endoscopic dissolution was attempted in only three cases. Based on these findings, we conducted a review of case reports describing endoscopic treatment for barium‐induced colonic obstruction (Table 1). Including the present case, a total of nine cases of endoscopic treatment have been reported, with the site of obstruction located in the left colon in all cases. Among the nine cases, endoscopic removal was successful in five, while three of the four unsuccessful cases required surgical intervention. These findings suggest that endoscopic treatment is technically challenging and carries a high risk of requiring surgery. Moreover, since all successful cases showed no signs of peritoneal irritation, endoscopic treatment should be limited to patients with stable vital signs and no clinical or radiological evidence of generalized peritonitis or perforation. In this case, given the severity of symptoms and the risk of progression to perforation or generalized peritonitis, we determined that early endoscopic decompression was necessary. Although the patient developed localized peritonitis secondary to ischemic colitis due to bowel obstruction after the endoscopic procedure, her abdominal pain improved, and surgical intervention was avoided. Therefore, timely endoscopic intervention was considered a valuable treatment option for avoiding surgical intervention.
To date, there have been only a few reports on endoscopic treatment for barium impaction [3, 7, 8], and a considerable proportion of these attempts have been unsuccessful [3, 8]. This case report is particularly valuable as it presents a detailed presentation of the endoscopic procedure with video. Because of the high viscosity and density of barium, endoscopic removal is technically challenging. However, the combination of mechanical fragmentation using a snare and strong suction through a long hood without side holes proved effective in this case. We believe that this technique may also be applicable for the endoscopic removal of fecal impaction.
Barium can remain in the colon for several days to months [4], and impaction may occur even in patients with no prior constipation or bowel disease if the elimination of barolith is delayed. Patients are generally advised to hydrate and take laxatives after undergoing barium examinations. They are also instructed to seek medical attention if they do not have sufficient bowel movements. Although this patient had received these instructions, she did not visit a hospital despite having little to no bowel movement during that time, and sought medical attention when severe abdominal pain developed seven days after the examination. Therefore, it is important to ensure patients fully understand the risks and the importance of seeking care for prolonged constipation or abdominal pain [8].
In conclusion, we advocate for accumulating more case reports and procedural experiences to establish effective techniques and indications for endoscopic treatment, as well as appropriate patient management, for such rare complications.
Ethics Statement
The patient in this case report was treated within the standard scope of care under Japan's national health insurance. Informed consent was obtained from the patient for the medical treatment and procedures described. For the purpose of publication, all accompanying images and videos have been anonymized to ensure that the individual cannot be identified.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: Laboratory data.
Video S1: Endoscopic removal of impacted barium stools using a snare and a long hood.The video shows the process of removing the impacted barium stools endoscopically. The barium stools were impacted at a sharp bend in the sigmoid colon. First, we cut the stools with the snare. The fragmented stools were then suctioned into a long hood cup and removed. By repeating the same procedure, most of the stools were removed in 60 min.
Supporting File 3: deo270182‐sup‐0001‐SuppMat.docx
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1C. Hamashima , “Systematic Review Group and Guideline Development Group for Gastric Cancer Screening Guidelines. Update Version of the Japanese Guidelines for Gastric Cancer Screening,” Japanese Journal of Clinical Oncology 48 (2018): 673–683.29889263 10.1093/jjco/hyy 077 · doi ↗ · pubmed ↗
- 2M. A. Kurer , C. Davey , and S. Chintapatla , “Intestinal Obstruction From Inspissated Barium (Barolith): A Systematic Review of all Cases From 1950 to 2006,” Colorectal Disease 10 (2008): 431–439.18355376 10.1111/j.1463-1318.2008.01503.x · doi ↗ · pubmed ↗
- 3B. Sharpe , J. Switzer , and W. Mathews , “Surgical Management of Barium Impaction: A Case Report,” Cureus 16 (2024): e 61111.38919233 10.7759/cureus.61111 PMC 11197058 · doi ↗ · pubmed ↗
- 4S. Matsuo , S. Eguchi , T. Azuma , et al., “An Unusual Perforation of the Colon: Report of Two Cases,” Surgery Today 32 (2002): 836–839.12203068 10.1007/s 005950200163 · doi ↗ · pubmed ↗
- 5T. Kitajima , K. Tomizawa , Y. Hanaoka , et al., “Anastomotic Stenosis of the Descending Colon Caused by Barium Granuloma Formation Following Barium Peritonitis: Report of a Case,” Surgery Today 44 (2014): 2153–2156.23955478 10.1007/s 00595-013-0696-0PMC 4194026 · doi ↗ · pubmed ↗
- 6M. S. Noor , H. Liu , B. Joutovsky , et al., “Surgical Management of Intestinal Obstruction Secondary to Barium Impaction: Two Exemplary Cases,” Cureus 16 (2024): e 76301.39850195 10.7759/cureus.76301 PMC 11755390 · doi ↗ · pubmed ↗
- 7M. V. Vieiro Medina , M. de la Fuente Bartolomé , C. García Vásquez , et al., “Intestinal Obstruction Due to Bariolith Impaction,” Spanish Journal of Digestive Diseases 115 (2023): 519–520.10.17235/reed.2022.9084/202236043557 · doi ↗ · pubmed ↗
- 8G. F. Shaughnessy , P. Cho , and D. L. Francis , “A Rare Complication of a Barium‐contrast Study,” Clinical Gastroenterology and Hepatology 13 (2015): e 67–e 68.25576476 10.1016/j.cgh.2014.12.029 · doi ↗ · pubmed ↗