Enterocutaneous Fistula: A Challenging Complication in Cervical Cancer Management
Abigayle Wyer, Mena Louis, Oluwasemilore I Okunlola, Raven Richardson, Timothy J Stevens

TL;DR
A cervical cancer patient developed a rare and severe complication called an enterocutaneous fistula after treatment with bevacizumab and prior pelvic surgery.
Contribution
The paper highlights bevacizumab as a significant risk factor for fistula formation in patients with prior pelvic surgery or radiation therapy.
Findings
Enterocutaneous fistula developed in a cervical cancer patient treated with bevacizumab and prior pelvic surgery.
Bevacizumab disrupts tissue repair and increases fistula risk in susceptible patients.
Conservative management with nutritional support and wound care achieved medical stabilization.
Abstract
A 42-year-old woman with a history of cervical cancer previously treated with radical hysterectomy, lymphadenectomy, and bilateral salpingectomy presented with severe right lower extremity pain, initially attributed to routine chemotherapy-related side effects. Despite symptomatic management, her pain intensified, accompanied by abdominal distention, constipation, and reduced ambulation. Subsequent clinical evaluation revealed a significant abscess extending from the pelvis into the gluteal musculature and thigh. Imaging confirmed that the abscess communicated with a loop of the small bowel, evolving into an enterocutaneous fistula, which manifested as feculent drainage through her thigh incision. Surgical intervention with incision, drainage, and excision of nonviable muscle tissue provided temporary relief but could not entirely resolve the fistula. Microbiological cultures yielded…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
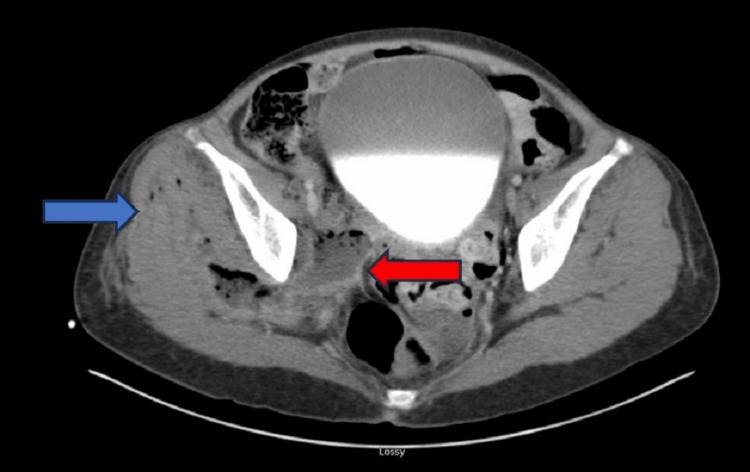 Figure 1
Figure 1 Figure 2
Figure 2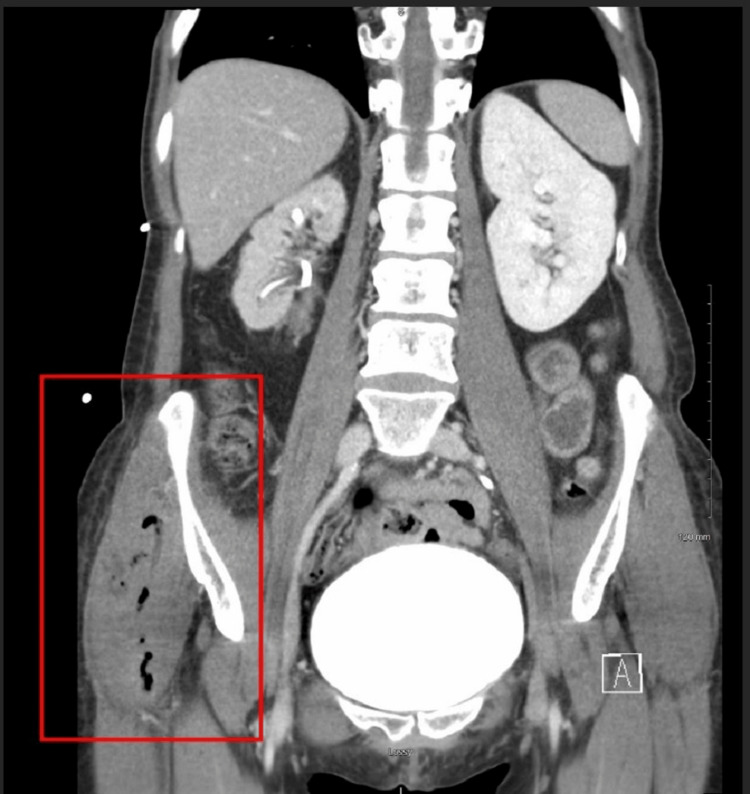 Figure 3
Figure 3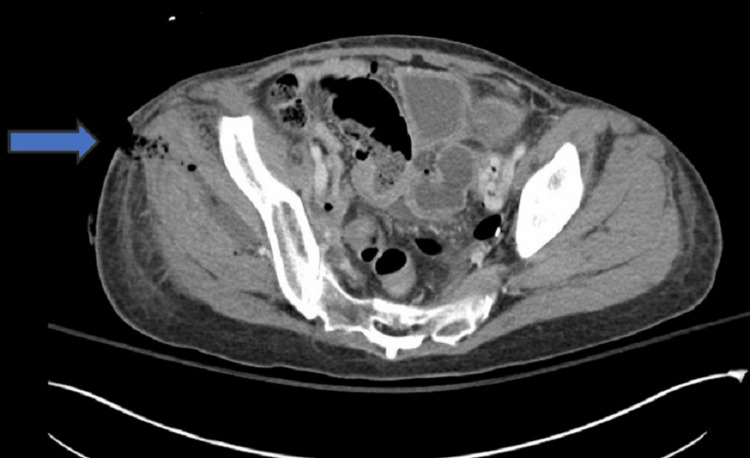 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8| Lab | Value | Reference value |
| Hemoglobin | 10.6 g/dL | 12.0-15.5 g/dL |
| Hematocrit | 32.3% | 36-48% |
| White blood cell count | 9.7 x 103/µL | 4,000-11,000 µL |
| Platelets | 193 x 103/µL | 150,000-450,000 µL |
| Alkaline phosphatase | 122 IU/L | 44-147 IU/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Abdominal Surgery and Complications · Congenital Diaphragmatic Hernia Studies
Introduction
Cervical cancer remains a significant global health issue, representing one of the leading malignancies affecting women worldwide [1]. Although the incidence has declined in countries with effective screening programs, cervical cancer continues to cause substantial morbidity and mortality, especially in populations with limited healthcare access [2]. Treatment for cervical cancer typically involves surgery, radiation, chemotherapy, or a combination of these modalities, depending on the stage and extent of the disease [3]. In advanced or recurrent cervical cancer cases, targeted therapy has emerged as an important adjunct, enhancing survival rates while aiming to maintain the quality of life.
Bevacizumab, a monoclonal antibody targeting vascular endothelial growth factor (VEGF), has significantly impacted the treatment landscape for advanced cervical cancer [4]. Its use, particularly in combination with chemotherapy, has demonstrated improved survival outcomes in patients with recurrent, persistent, or metastatic disease [5]. By inhibiting angiogenesis, bevacizumab disrupts tumor blood supply, thereby impairing growth and metastatic potential [6]. However, its mechanism of action carries inherent risks due to the critical role of VEGF in normal tissue healing and repair processes [7]. Consequently, bevacizumab therapy has been associated with notable adverse effects, including hypertension, proteinuria, hemorrhage, thromboembolic events, and delayed wound healing [8].
Among the serious complications associated with bevacizumab therapy, fistula formation has increasingly garnered attention in clinical oncology [8]. Fistulas, abnormal communications between two epithelial-lined organs or between an organ and the skin, significantly impair patient quality of life and pose substantial therapeutic challenges [9]. This complication arises more frequently in patients treated with bevacizumab, particularly when therapy follows surgery or radiotherapy [10]. The mechanism behind increased fistula formation involves bevacizumab-induced inhibition of angiogenesis, which impairs tissue healing, reduces vascular integrity, and ultimately facilitates fistulous communication through weakened tissue planes [11].
Multiple studies have documented elevated rates of gastrointestinal and genitourinary fistulas among patients receiving bevacizumab in the context of pelvic malignancies, notably cervical and colorectal cancers [12]. The increased risk is especially prominent in those who have undergone pelvic surgery or radiotherapy due to compromised vascular supply and tissue healing capacity in these previously treated regions [13]. Awareness of this complication is essential for timely diagnosis and management, as early detection and intervention may significantly reduce patient morbidity and healthcare burden.
Case presentation
A 42-year-old woman with a history of cervical cancer treated initially with radical abdominal hysterectomy, lymphadenectomy, bilateral salpingectomy, and ovarian transposition in November 2021 presented to the emergency department with severe right leg and abdominal pain. Her cervical cancer had been complicated by a likely localized recurrence around her right ureter, for which she was undergoing chemotherapy. After her second chemotherapy session, she reported worsening right upper leg pain, initially attributed by her oncology team to muscular side effects. Despite the reassurance, the pain progressed, involving her right hip and rendering her unable to ambulate or abduct her right hip. She also experienced abdominal distention and constipation, and reported having no significant bowel movements for approximately one week despite attempting suppositories.
Initial laboratory evaluation revealed mild anemia, normal leukocyte counts, and a normal platelet count. The basic metabolic profile and inflammatory markers were within acceptable limits, except for a mildly elevated alkaline phosphatase (Table 1). Imaging studies performed upon admission demonstrated a complex abscess with fluid and gas collections in the right hemipelvis, extending into the gluteal musculature and communicating with a loop of small bowel. Subsequent cultures from the fluid obtained during the operative intervention grew Bacteroides ovatus, Escherichia coli, and Enterococcus faecium, indicating an intestinal origin. A CT angiography of the lower extremity confirmed significant obturator and gluteal myositis with associated gas and fluid collections, raising concern for a developing enterocutaneous fistula (Figures 1-3).
Axial CT image of the pelvis demonstrating a complex pelvic abscess characterized by fluid and gas collections in the right hemipelvis (blue arrow), extending into the gluteal musculature. Notably, the abscess shows a clear communication with an adjacent loop of small bowel (red arrow)CT: computed tomography
Axial CT image of the pelvis demonstrating a complex pelvic abscess characterized by fluid and gas collections in the right hemipelvis (blue arrow), extending into the gluteal musculatureCT: computed tomography
Coronal CT image of the abdomen and pelvis illustrating a prominent area of fluid and gas collection within the right hemipelvis indicating a pelvic abscess (marked by a red rectangle)CT: computed tomography
The patient was admitted to the acute care surgical service and underwent urgent surgical incision and drainage of the right hip and thigh abscess on hospital day two. Intraoperative findings included extensive subcutaneous edema and multiple loculated pockets of foul-smelling purulent fluid within the muscle compartments, necessitating excision of approximately 4 cm² of nonviable muscle tissue. Despite adequate drainage and initial stabilization, postoperative imaging demonstrated the progression of the fluid collection. It confirmed the presence of a direct fistulous communication between the bowel and the surgical wound, manifesting clinically as feculent drainage from the surgical site (Figures 4-6).
Axial CT image of the pelvis demonstrating progression of the pelvic fluid collection with clear evidence of a fistulous connection between the bowel and the surgical wound. The blue arrows indicate the fistula tractCT: computed tomography
Coronal CT image of the pelvis demonstrating progression of the pelvic fluid collection with clear evidence of a fistulous connection between the bowel and the surgical wound. The blue arrows indicate the fistula tractCT: computed tomography
Clinical photograph showing the surgical wound site on postoperative day 3 with foul-smelling feculent drainage consistent with enterocutaneous fistula output
During hospitalization, the patient developed an overt enterocutaneous fistula, with significant stool output draining through the thigh incision site, requiring management with an external ostomy appliance (Figures 7-8). Persistent abdominal cramps and partial small bowel obstruction further complicated her clinical course. Conservative management was initially pursued to optimize nutritional status and promote healing, but the patient required ongoing analgesic support and wound care. Ultimately, medical stabilization was achieved through supportive measures. She demonstrated gradual improvement and was eventually discharged with ongoing wound management instructions, nutritional support, and close outpatient follow-up.
Clinical photograph on postoperative day 4 showing the fistula managed with an ostomy appliance capturing significant stool output from the wound site
Clinical photograph on postoperative day 18 demonstrating ongoing management of the fistula with an ostomy appliance with continued fistula output
Discussion
Unusual wounds in typical anatomical locations present a diagnostic challenge, especially when they fail to respond to conventional treatments [14]. Chronic or non-healing wounds require clinicians to maintain a broad differential diagnosis, considering possibilities such as underlying infection, malignancy, foreign bodies, immunocompromised states, and, notably, the potential presence of a fistula. Enterocutaneous fistulas, abnormal connections between the gastrointestinal tract and skin, are particularly important to recognize early, as delayed diagnosis significantly increases morbidity and complicates management [15]. Clinicians should suspect fistula formation in any chronic wound exhibiting persistent drainage of fluid with unusual odor, feculent material, gas bubbles, or unexplained skin breakdown despite standard wound care.
When evaluating a patient with a chronic, non-healing wound, detailed patient history and thorough clinical examination are fundamental. A history of previous abdominal or pelvic surgery, radiation therapy, malignancy, inflammatory bowel disease, or recent chemotherapy raises suspicion for an enterocutaneous fistula. Clinical examination findings suggestive of a fistulous communication include persistent drainage, skin irritation, unusual discharge color, and gaseous emissions [16]. Prompt diagnostic imaging, typically contrast-enhanced CT, helps delineate fistulous tracts, localize the source of communication, and identify associated complications such as abscess formation or bowel obstruction. Early imaging has a significant impact on management strategies and patient outcomes.
Management of enterocutaneous fistulas begins with stabilization of the patient, control of sepsis, nutritional optimization, and detailed assessment of wound output and characteristics [17]. Conservative management typically involves initial non-operative strategies, including intravenous antibiotics, nutritional support (often parenteral nutrition), and wound care aimed at controlling drainage and protecting surrounding skin integrity. An ostomy appliance can be used effectively for skin protection and fluid containment, thereby improving patient comfort and quality of life. Non-operative management is particularly valuable early in the clinical course, allowing the fistula to close spontaneously if conditions are optimal, typically within several weeks to months [18].
However, surgical intervention becomes necessary in patients who fail conservative management, exhibit persistent high-output fistulas, uncontrolled sepsis, or progressive nutritional deterioration [19]. The optimal timing of surgical repair is critical, with literature supporting delayed surgical approaches to allow inflammation to subside, nutritional status to improve, and infection to be adequately controlled [19]. Surgical intervention typically involves resection of involved bowel segments, careful closure or diversion of the fistula, and meticulous handling of tissue to promote healing. Surgical decision-making requires individualized assessment, balancing risks associated with immediate intervention against the potential morbidity of prolonged conservative management.
In the context of cervical cancer treatment, chemotherapy, and specifically anti-angiogenic therapy such as bevacizumab, significantly increases the risk of fistula formation, especially in previously irradiated or surgically altered pelvic tissues [5]. Anti-angiogenic agents compromise normal vascular repair mechanisms, impairing wound healing and increasing tissue susceptibility to fistula formation [4]. Recognizing this elevated risk enables clinicians to closely monitor these patients, ensuring early intervention at initial signs of fistula formation, thereby preventing severe complications.
A multidisciplinary approach remains essential for managing complex wounds complicated by fistula formation. Coordinated efforts involving surgeons, wound care specialists, infectious disease experts, dietitians, and oncologists to optimize patient outcomes. Patient education, emphasizing the importance of reporting persistent or unusual symptoms, also plays a significant role.
Patients experiencing chronic wounds complicated by fistula formation often endure significant psychological distress due to prolonged hospitalizations, physical discomfort, altered body image, and impaired social functioning. Addressing the mental health of these patients is essential and requires a compassionate, empathetic approach involving early psychological assessment, emotional support, and counseling services. Establishing open communication, setting realistic expectations, and involving patients actively in decision-making can help restore their sense of autonomy and control. Additionally, integrating mental health professionals into the multidisciplinary team and offering consistent emotional support through peer groups or counseling can significantly improve patients' coping mechanisms, adherence to treatment, and overall quality of life.
Conclusions
This case report emphasizes the significant risk of fistula formation associated with bevacizumab therapy in cervical cancer patients, particularly in those previously treated with pelvic surgery or radiotherapy. Clinicians must remain vigilant, maintaining a high level of suspicion for early symptoms suggestive of this complication. Early identification, timely imaging, and a coordinated multidisciplinary approach are vital to managing these complex clinical situations effectively, thereby minimizing morbidity and improving patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cervical cancer: epidemiology, risk factors and screening Chin J Cancer Res Zhang S Xu H Zhang L Qiao Y 7207283220203344699510.21147/j.issn.1000-9604.2020.06.05PMC 7797226 · doi ↗ · pubmed ↗
- 2Looking back, moving forward: challenges and opportunities for global cervical cancer prevention and control cervical cancer management Viruses Castle PE 13571620243933983410.3390/v 16091357 PMC 11435674 · doi ↗ · pubmed ↗
- 3Cervical cancer therapies: current challenges and future perspectives Tumour Virus Res Burmeister CA Khan SF Schäfer G Mbatani N Adams T Moodley J Prince S 2002381320223546094010.1016/j.tvr.2022.200238 PMC 9062473 · doi ↗ · pubmed ↗
- 4Bevacizumab for the treatment of cervical cancer Expert Opin Biol Ther Bizzarri N Ghirardi V Alessandri F 4074191620162679633210.1517/14712598.2016.1145208 · doi ↗ · pubmed ↗
- 5Bevacizumab for advanced cervical cancer: final overall survival and adverse event analysis of a randomised, controlled, open-label, phase 3 trial (Gynecologic Oncology Group 240)Lancet Tewari KS Sill MW Penson RT 1654166339020172875690210.1016/S 0140-6736(17)31607-0PMC 5714293 · doi ↗ · pubmed ↗
- 6Pembrolizumab plus chemotherapy for advanced and recurrent cervical cancer: final analysis according to bevacizumab use in the randomized KEYNOTE-826 study Ann Oncol Lorusso D Colombo N Dubot C 65753620253939377710.1016/j.annonc.2024.10.002 · doi ↗ · pubmed ↗
- 7Real-world efficacy and safety of bevacizumab single-maintenance therapy following platinum-paclitaxel chemotherapy plus bevacizumab in patients with advanced cervical cancer J Gynecol Oncol Kotaka S Kondo E Kawai Y 6034202310.3802/jgo.2023.34.e 60PMC 1048258637170726 · doi ↗ · pubmed ↗
- 8Incidence of fistula occurrence in patients with cervical cancer treated with bevacizumab: data from real-world clinical practice Int J Clin Oncol Sugiyama T Katsumata N Toita T Ura M Shimizu A Kamijima S Aoki D 151715282720223576094310.1007/s 10147-022-02196-8PMC 9393147 · doi ↗ · pubmed ↗