Ileal free flap for hypopharynx reconstruction – case series
Luis Fernando Tintinago-Londoño, Estephania Candelo, Tania Guzmán, William Victoria-Morales

TL;DR
This case series explores using ileal free flaps to reconstruct the hypopharynx while preserving the larynx, showing promising results in six patients.
Contribution
The study introduces the ileal free flap as a novel surgical option for hypopharyngeal reconstruction with larynx preservation.
Findings
The ileal free flap achieved 100% graft survival in six cases.
Three patients had normal swallowing function post-surgery.
Two cases with stenosis improved with endoscopic dilation.
Abstract
Reconstructing the hypopharynx while preserving the larynx poses a complex surgical challenge due to the limited space and the high position of the hypopharynx in the neck. We present our experience with hypopharyngeal reconstruction and larynx preservation using an ileal free flap. Six consecutive cases were reported (age range 17–75; 2 females). Indications for surgery were tumor excision, postexcision flap failure, postradiation stenosis, caustic ingestion injury, and cervical esophageal perforation. The larynx was preserved in four cases. Graft survival rate was 100 %. Videofluoroscopic swallowing studies conducted at postoperative day 20–80 were normal in three cases. Two cases presented with stenosis but responded well to endoscopic dilations. Unfortunately, the third case expired due to tumor recurrence. The ileal free flap is a surgical alternative for the reconstruction of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
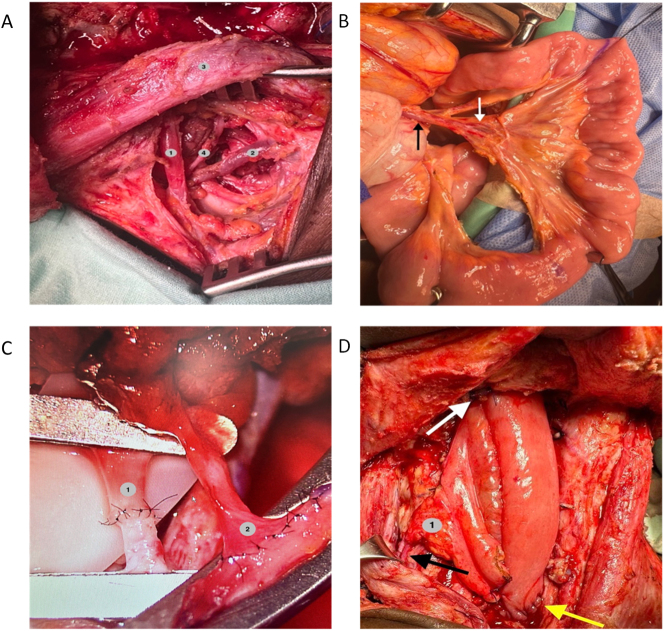 Figure 1
Figure 1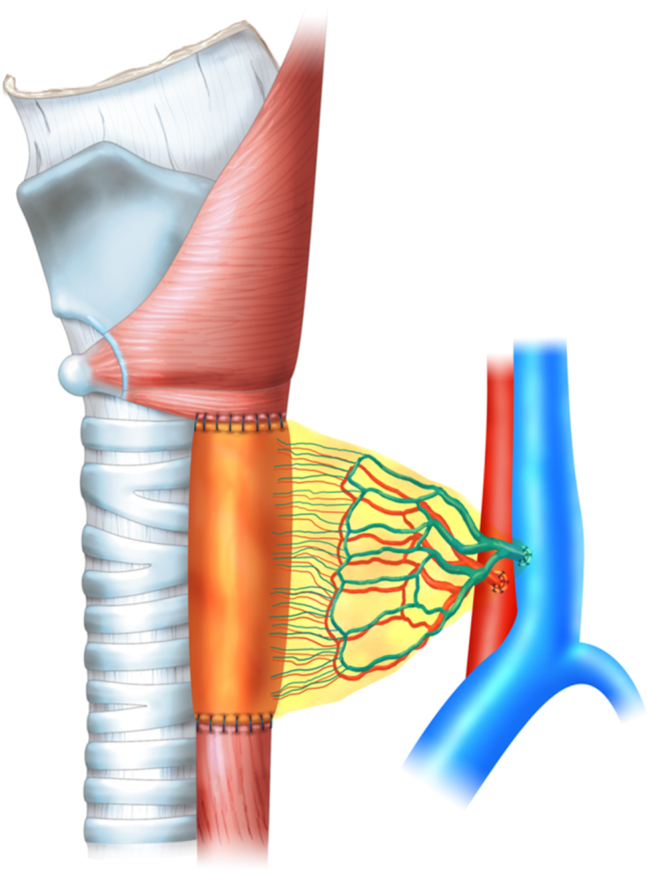 Figure 2
Figure 2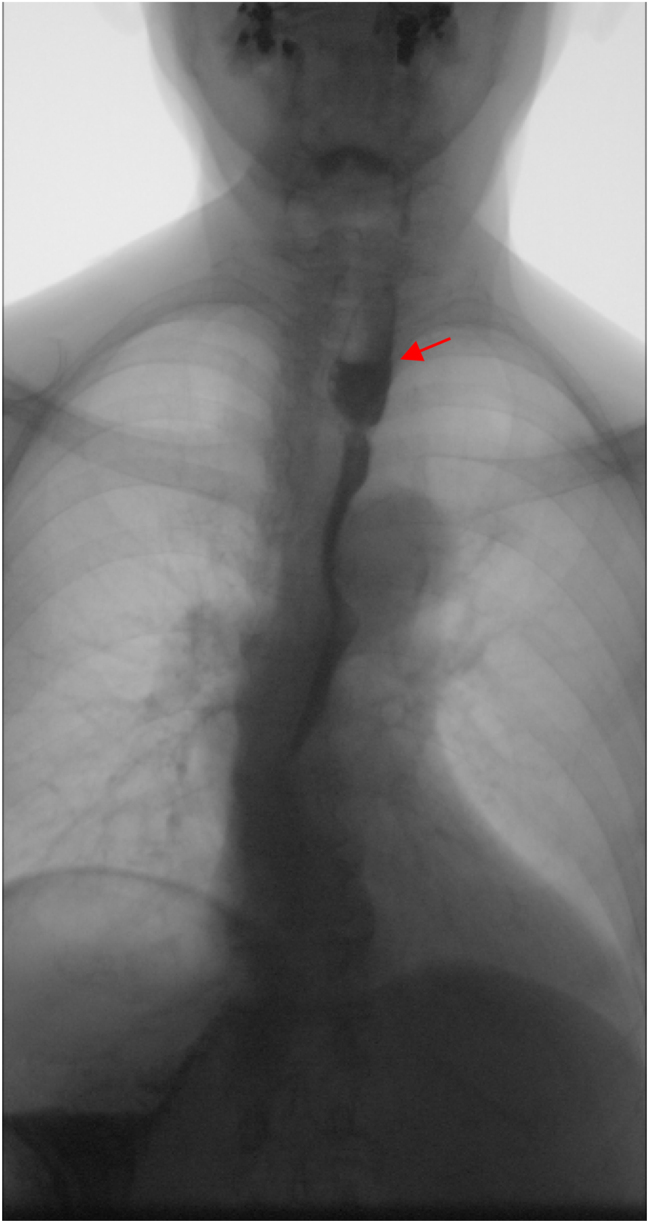 Figure 3
Figure 3| Case | Gender | Age | Past medical history | Indication for surgery | Surgical procedures | Larynx preservation |
|---|---|---|---|---|---|---|
| 1 | Male | 53 | – Esophageal perforation following foreign body ingestion | Esophageal stenosis | – Hypopharyngeal and cervical esophagus resection | Yes |
| – Reconstruction with ileal free flap | ||||||
| 2 | Female | 17 | – Corrosive injury following caustic ingestion | Esophagogastric stenosis | – Esophagogastric resection | Yes |
| – Reconstruction with ileal free flap and colon interposition | ||||||
| 3 | Male | 60 | – Esophageal stenosis following radiotherapy for esophageal cancer | Jejunal free flap failure | – Jejunal free flap resection | Yes |
| – Tumor excision and reconstruction with jejunal free flap | – Reconstruction with ileal free flap | |||||
| 4 | Male | 75 | – Tumor excision of an invasive laryngeal cancer and reconstruction with jejunal free flap | Iatrogenic jejunal free flap stenosis | – Jejunal free flap resection | No |
| – Reconstruction with ileal free flap | ||||||
| 5 | Male | 54 | – Tumor excision of an invasive laryngeal cancer | Tumor excision | – Hypopharyngeal and cervical esophageal resection | No |
| – Reconstruction with ileal free flap | ||||||
| 6 | Female | 73 | – Esophageal stenosis following radiotherapy for esophageal cancer | Esophageal stenosis | – Hypoharyngeal and cervical esophagus resection | Yes |
| – Reconstruction with ileal free flap |
| Case | Esophagoscopy (24–48 h) | Esophagoscopy (10–14 days) | Esophagoscopy (3 months) | Day pasty diet began | Day solid diet began | Videofluoroscopic swallowing study (20–80 days) | Outpatient follow-up (month 1) | Outpatient follow-up (month 6) |
|---|---|---|---|---|---|---|---|---|
| 1 | – Vital 100 % | – Vital 100 % | – Vital 100 % | 15 | 20 | Normal | Diet without restrictions | Diet without restrictions |
| – No stenosis | – No stenosis | – No stenosis | ||||||
| 2 | – Vital 100 % | – Vital 100 % | – Vital 100 % | 20 | 25 | Normal | Diet without restrictions | Diet without restrictions |
| – No stenosis | – No stenosis | – No stenosis | ||||||
| 3 | – Vital 100 % | – Vital 100 % | – Vital 100 % | No | Partial obstruction distal to the ileal free flap (tumor recurrence) | Tolerating liquid diet | Tube feeding due to complete obstruction (tumor recurrence) | |
| – No stenosis | – No stenosis | – No stenosis | ||||||
| 4 | – Vital 100 % | – Vital 100 % | – Vital 100 % | 15 | No | Dysphagia (solids) | Tolerating soft solid diet | Tolerating soft solid diet |
| – Proximal and distal anastomoses edema | – No stenosis | |||||||
| 5 | – Vital 100 % | – Vital 100 % | – Vital 100 % | 14 | 20 | Normal | Diet without restrictions | Diet without restrictions |
| – No stenosis | – No stenosis | – No stenosis | ||||||
| 6 | – Vital 100 % | – Vital 100 % | – Vital 100 % | 81 | 88 | Dysphagia (pasty) | Tube feeding due to dysphagia (liquids) | Diet without restrictions |
| – No stenosis | – No stenosis | – No stenosis |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Trauma Management and Diagnosis · Tracheal and airway disorders
Introduction
Reconstruction of the hypopharynx and cervical esophagus poses significant challenges. While several techniques have been described, few reports of the ileal free flap have been published [1], [2], [3], [4]. We present six cases of hypopharyngeal and cervical esophageal reconstruction with larynx preservation using ileal free flap. Our objective is to demonstrate the feasibility of using this technique for reconstructing the hypopharynx and esophagus, considering the anatomical distinctions of the ileum that make it particularly suitable in select cases, especially when the larynx is preserved.
Surgical technique summary
The surgical procedure began with a median neck incision, extending from the hyoid region to the suprasternal notch, facilitating exposure of the airway. Cervical vessels were meticulously dissected to ensure precision. Special attention was given in cases requiring larynx preservation to prevent any inadvertent damage to the recurrent laryngeal nerves.
For graft harvesting, a median laparotomy was performed, and a segment of the ileum, approximately 20 cm proximal to the ileocecal valve, was identified. The vascular pedicle between the second arches proximal to the surface of the ileum was carefully identified and dissected until reaching a length of 2 cm along its longest axis. The isolated segment was then perfused with a heparin solution, and its proximal end was marked for identification during cervical reconstruction. Restoration of ileal continuity was achieved through an end-to-end anastomosis.
Subsequently, the proximally marked end of the ileum segment was anastomosed to the hypopharynx in a terminolateral fashion with interrupted sutures using nonabsorbable monofilament, and the distal end was similarly anastomosed to the cervical esophagus, thus reconstructing the digestive conduit defect. The remaining peritoneum was placed to cover all the anastomoses, securing it to the operating field and hemostasis was ensured before closing the incision (Figures 1 and 2).
Surgical technique for hypopharynx reconstruction with ileal free flap. (A) Vascular neck dissection. (1) Omohyoid muscle; (2) ascending cervical vein; (3) sternocleidomastoid; (4) transverse cervical artery. (B) Ileal vascular pedicle. Black arrow: ileal vein; white arrow: ileal artery. (C) Microvascular anastomoses. (1) Transverse cervical artery branch-ileal branch anastomoses; (2) ascending cervical vein branch-ileal branch anastomoses. (D) Hypopharynx reconstruction. (1) Omentum; black arrow: vascular anastomoses; white arrow: hypopharyngeal anastomoses; yellow arrow: esophageal anastomoses.
Hypopharyngeal and cervical esophageal reconstruction in larynx-preserved digestive conduit defects.
Case presentation
Six consecutive cases were reported (age range 17–75; 2 females). Tables 1 and 2 summarize patient characteristics and postoperative outcomes. All patients were diagnosed and treated at a tertiary care university hospital in Cali, Colombia between May 2017 and June 2022.
Indications for surgery were tumor excision, post tumor excision jejunal free flap graft failure, postradiation esophageal stenosis, corrosive injury due to caustic ingestion, and cervical esophageal perforation due to foreign body ingestion. The larynx was preserved in four cases.
Postoperative outcomes include (1) graft survival as evidenced on esophagoscopies at postoperative 24–48 h and 10–14 days, (2) onset of swallowing as evidenced by the first successful intake of a pasty diet meal, (3) digestive conduit functioning as evidenced by videofluoroscopic swallowing tests (Figure 3) at postoperative 20–80 days, and (4) the state of deglutition as reported by the patients at first- and sixth-month outpatient follow-ups.
Videofluoroscopic swallowing study at day 72 after hypopharyngeal and cervical esophageal reconstruction. The red arrow points to the patent ileal free flap segment.
Graft survival rate was 100 % and videofluoroscopic swallowing studies at postoperative day 20–80 were normal in three cases. Two abnormal cases presented with stenosis: one at the distal ileo-esophageal anastomosis and the other involving both esophageal anastomotic sites. Both responded well to endoscopic dilations. The third case involved tumor recurrence, causing extrinsic compression of the distal esophagus, requiring tube feeding due to obstruction. The latter patient expired due to tumor recurrence and subsequent malignant hypercalcemia.
The patients initiated oral intake 48 h postoperatively, without experiencing subsequent complications such as wound dehiscence, fistula formation, or peritonitis. At the 3-month follow-up assessment, all grafts demonstrated a 100 % survival rate, with no associated complications.
Discussion
Several reconstruction techniques have been described, including locoregional tubularized island flaps, gastric pull-up, and jejunum free flaps [5], [6], [7], [8]. Our experience suggests that the ileum presents advantages over other tissues for hypopharyngeal reconstruction and larynx preservation. This innovative approach simplifies the surgical process and enhances postoperative outcomes.
While the technique of free jejunum grafting and the radial fasciocutaneos flap have been more extensively documented, advances in microsurgery have enabled the feasibility of hypopharyngeal and cervical esophageal reconstructions using the ileal free flap [3]. In comparison with the radial fasciocutaneous flap, the ileum exhibits peristalsis, facilitating postoperative swallowing recovery. Furthermore, it requires only the anastomosis of its edges, in contrast to the radial flap which requires a third anastomosis [9].
Additionally, the ileum outperforms the jejunum due to its thinner intestinal walls and a diameter similar to that of the cervical esophagus, facilitating a more feasible anastomosis with the walls of the hypopharynx [10]. Furthermore, the dimensions of the ileum make it more technically suitable for accommodating restricted spaces, as notably observed in four of our cases where the larynx was preserved.
No focal necrosis or anastomotic leakages were observed in any of the esophagoscopies. Moreover, 80 % of our patients maintained oral feeding 6 months postoperatively, while the remaining patient required tube feeding due to malignancy recurrence causing extrinsic esophageal obstruction.
The primary limitation of this study is its lack of comparison with another technique, which precludes a definitive assessment of the superiority of the ileal free flap over other tissues. Nevertheless, our findings demonstrate that the ileal free flap serves as an innovative surgical alternative to address complex anatomical challenges in the reconstruction of the hypopharynx and cervical esophagus, particularly in cases where laryngeal preservation is crucial. This is attributed to its anatomical compatibility, facilitating digestive anastomosis with the hypopharynx and leading to favorable clinical outcomes.
Conclusions
The ileal free flap represents a promising and innovative alternative for hypopharyngeal and cervical esophageal reconstruction, particularly in cases where there is limited cervical space, such as when larynx preservation is required. Our study highlights its potential as a technically feasible and successful approach in addressing complex anatomical challenges.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jurkiewicz MJ Vascularized intestinal graft for reconstruction of the cervical esophagus and pharynx Plast Reconstr Surg 1965365091710.1097/00006534-196511000-000025838550 · doi ↗ · pubmed ↗
- 2Harashina T Kakegawa T Imai T Suguro Y Secondary reconstruction of oesophagus with free revascularised ileal transfer Br J Plast Surg 198134172210.1016/0007-1226(81)90088-67459518 · doi ↗ · pubmed ↗
- 3Vavylov VN Ushakov VS Tokarevitch KK Krasnoumov AN Kasyanov IV Semyonov SV Microvascular free transfer in reconstruction of the pharynx and cervical esophagus Ann Plast Surg 199331443610.1097/00000637-199311000-000108285530 · doi ↗ · pubmed ↗
- 4Bax NMA Van Renterghem KM Ileal pedicle grafting for esophageal replacement in children Pediatr Surg Int 2005213697210.1007/s 00383-005-1433-615827751 · doi ↗ · pubmed ↗
- 5Yu P Robb GL Pharyngoesophageal reconstruction with the anterolateral thigh flap: a clinical and functional outcomes study Plast Reconstr Surg 200511618455510.1097/01.prs.0000191179.58054.8016327594 · doi ↗ · pubmed ↗
- 6Kokot N Mazhar K Reder LS Peng GL Sinha UK The supraclavicular artery island flap in head and neck reconstruction: applications and limitations JAMA Otolaryngol Neck Surg 201313912475510.1001/jamaoto.2013.505724158458 · doi ↗ · pubmed ↗
- 7Schusterman MA Shestak K de Vries EJ Swartz W Jones N Johnson J Reconstruction of the cervical esophagus Plast Reconstr Surg 199085162110.1097/00006534-199001000-000042293731 · doi ↗ · pubmed ↗
- 8Baldwin D Gonzalez SR Anand S Esophageal reconstruction Stat Pearlshttps://www.ncbi.nlm.nih.gov/books/NBK 564336/Accessed 15 Nov 202333232006 · pubmed ↗