Prevalence and impact of sarcopenia on urinary incontinence in localized prostate cancer patients undergoing laparoscopic radical prostatectomy
Tengfei Gu, Jie Li, Dan Wu, Ting Chen, Yongtao Pan, Qinzhou Yu, Jing Sha

TL;DR
This study shows that sarcopenia, or low muscle mass, is common in prostate cancer patients and increases the risk of urinary incontinence after surgery.
Contribution
The study identifies sarcopenia as an independent predictor of urinary incontinence after laparoscopic radical prostatectomy.
Findings
Sarcopenia was found in 40.86% of localized prostate cancer patients.
Patients with sarcopenia had significantly higher urinary incontinence rates at 3 and 6 months post-surgery.
Sarcopenia remained an independent predictor of incontinence after adjusting for confounding factors.
Abstract
This research seeks to assess the prevalence of sarcopenia in patients diagnosed with localized prostate cancer and to investigate the influence of sarcopenia on the incidence of urinary incontinence following laparoscopic radical prostatectomy. A cohort of 350 patients, diagnosed with prostate cancer and having undergone laparoscopic radical prostatectomy at our hospital’s urology department between January 2022 and December 2023, was selected for this study. The cohort comprised 215 patients classified as low to intermediate risk and 135 patients classified as high risk. Participants were categorized into two groups: the sarcopenia group (n = 143) and the non-sarcopenia group (n = 207). The study aimed to summarize the prevalence of sarcopenia among patients with localized prostate cancer and to compare the incidence of urinary incontinence immediately post-surgery, as well as at…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
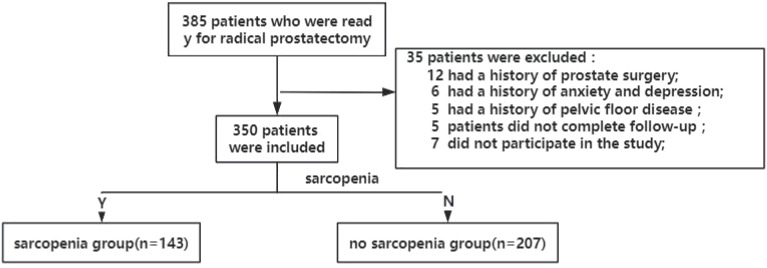 Figure 1
Figure 1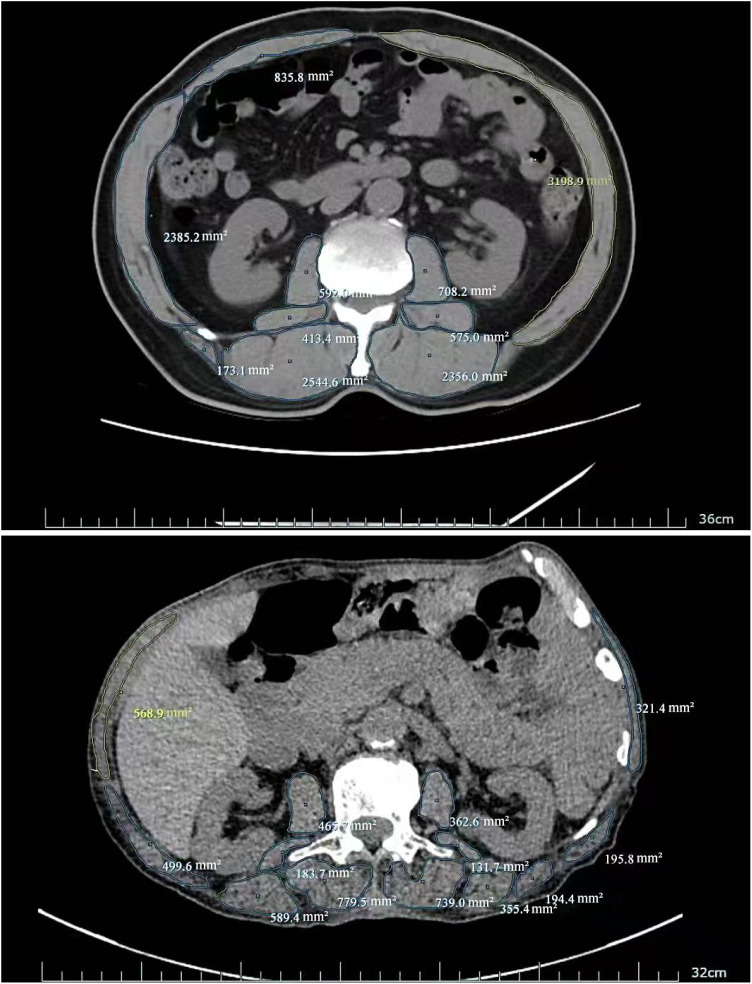 Figure 2
Figure 2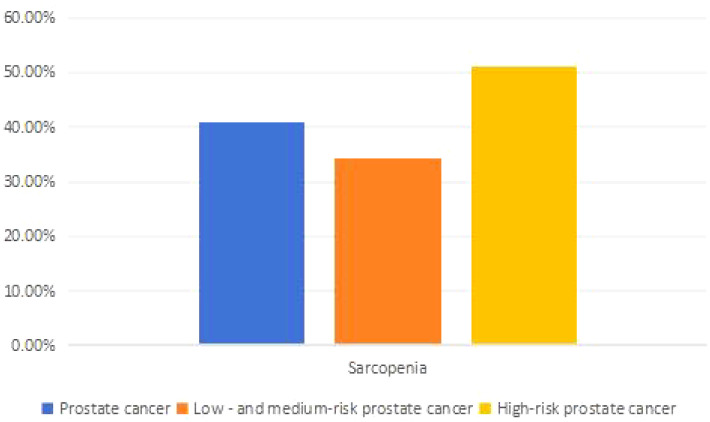 Figure 3
Figure 3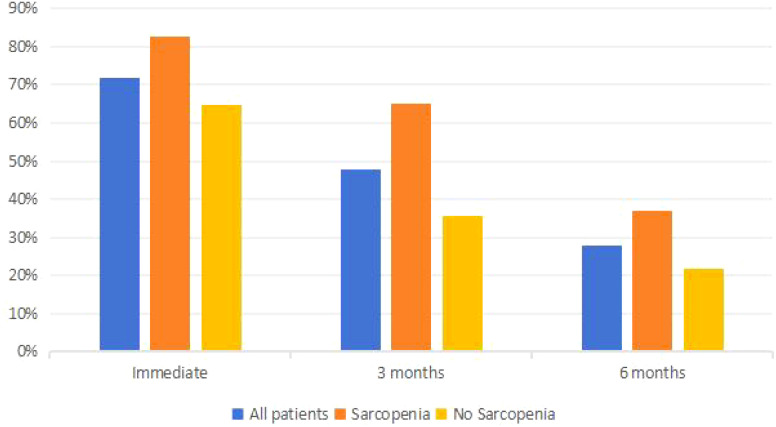 Figure 4
Figure 4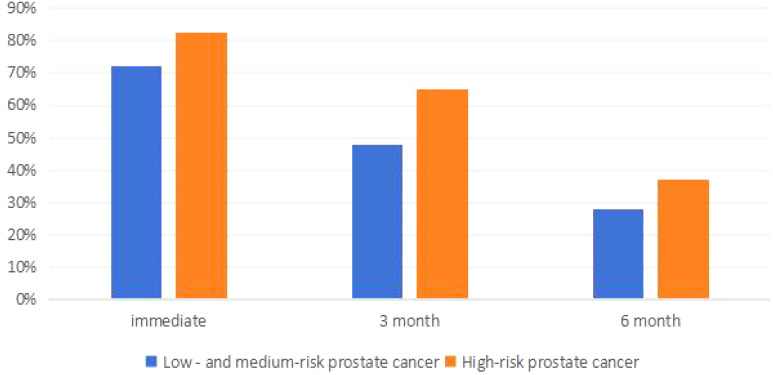 Figure 5
Figure 5| Index | Sarcopenia group (n=143) | No Sarcopenia group (n=207) | t or x2 | P |
|---|---|---|---|---|
| Age (year) | 75.65±7.35 | 74.83±7.59 | 2.784 | 0.042 |
| BMI (kg/m2) | 25.37±3.89 | 25.46±7.64 | 1.864 | 0.059 |
| Education | 0.054 | 0.718 | ||
| illiteracy | 13 (9.09%) | 23 (11.11%) | ||
| primary | 82 (57.34%) | 122 (58.94%) | ||
| junior | 33 (23.08%) | 44 (21.26%) | ||
| senior | 15 (10.49%) | 18 (8.69%) | ||
| Insurance | 0.322 | 0.56 | ||
| rural | 72 (50.32%) | 97 (47.10%) | ||
| urban | 71 (49.68%) | 110 (52.90%) | ||
| Income (thousand) | 5.001 | 0.025 | ||
| <50 | 101 (70.97%) | 122 (58.94%) | ||
| 50-100 | 32 (22.58%) | 62 (29.95%) | ||
| >100 | 10 (6.45%) | 23 (11.11%) | ||
| Comorbidities | 35 (24.48%) | 29 (14.19%) | 6.200 | 0.013 |
| coronary heart disease | 4 (3.22%) | 17 (8.39%) | 3.775 | 0.052 |
| cerebral infarction | 8 (5.81%) | 21 (10.32%) | 2.132 | 0.144 |
| hypertension | 66 (46.45%) | 89 (43.23%) | 0.326 | 0.568 |
| Smoking | 0.298 | 0.585 | ||
| Yes | 102 (71.33%) | 142 (68.59%) | ||
| No | 41 (28.67%) | 65 (41.41%) | ||
| Drinking | 0.417 | 0.518 | ||
| Yes | 98 (68.53%) | 135 (65.22%) | ||
| No | 45 (31.47%) | 72 (34.78%) | ||
| prostate volume (ml) | 62.71±9.05 | 62.47±6.73 | 1.234 | 0.214 |
| PSA (>20 ng/ml) | 1.168 | 0.280 | ||
| Yes | 34 (23.78%) | 60 (28.99%) | ||
| No | 109 (76.22%) | 147 (71.01%) | ||
| Gleason score (>7) | 0.690 | 0.406 | ||
| Yes | 45 (31.47%) | 74 (35.75%) | ||
| No | 98 (68.53%) | 133 (64.25%) | ||
| TMN staging (>T2b) | 1.907 | 0.167 | ||
| Yes | 43 (30.07%) | 77 (37.19%) | ||
| No | 100 (69.93%) | 130 (62.81%) | ||
| Neoadjuvant | 0.08 | 0.778 | ||
| Yes | 32 (22.58%) | 49 (23.87%) | ||
| No | 111 (77.42%) | 158 (76.13%) | ||
| Pelvic floor function | 60.95±11.26 | 79.29±6.19 | 17.721 | <0.001 |
| Index | Prostate cancer | Low and medium risk prostate cancer (n=215) | High risk prostate cancer (n=135) | x2 | P |
|---|---|---|---|---|---|
| Sarcopenia | 143 (40.86%) | 74 (34.42%) | 69 (51.11%) | 9.563 | 0.002 |
| Non-sarcopenia | 207 (59.14%) | 141 (65.58%) | 66 (48.89%) |
| Time | All patients | Sarcopenia group (n=143) | No Sarcopenia group (n=207) | x2 | P |
|---|---|---|---|---|---|
| immediately | 252 (72%) | 118 (82.52%) | 134 (64.73%) | 13.267 | <0.001 |
| 3 months | 167 (47.81%) | 93 (65.03%) | 134 (64.73%) | 29.076 | <0.001 |
| 6 months | 98 (28%) | 53 (37.06%) | 45 (21.74%) | 9.851 | 0.002 |
| Time | Low and medium risk prostate cancer (n=215) | High risk prostate cancer (n=135) | x2 | P |
|---|---|---|---|---|
| immediately | 128 (59.53%) | 124 (91.85%) | 42.961 | <0.001 |
| 3 months | 70 (32.56%) | 97 (71.85%) | 51.324 | <0.001 |
| 6 months | 35 (16.28%) | 63 (46.67%) | 37.984 | <0.001 |
| Time | Low and medium risk with sarcopenia (n=74) | Low and medium risk without sarcopenia (n=141) | x2 | P | High risk with sarcopenia (n=69) | High risk without sarcopenia (n=66) | x2 | P |
|---|---|---|---|---|---|---|---|---|
| immediately | 51 (68.92%) | 77 (54.61%) | 4.125 | 0.049 | 67 (97.10%) | 57 (86.36%) | 5.197 | 0.023 |
| 3 months | 40 (54.05%) | 30 (21.28%) | 23.745 | 0.001 | 53 (76.81%) | 44 (66.67%) | 1.717 | 0.190 |
| 6 months | 14 (18.92%) | 21 (14.89%) | 0.577 | 0.448 | 39 (56.52%) | 24 (36.36%) | 5.507 | 0.019 |
| Influencing factor | Univariable analysis | Multivariable analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | P | OR | 95%CI | P | |
| High-risk prostate cancer | 0.358 | 0.231-0.556 | <0.001 | 0.384 | 0.244-0.604 | <0.001 |
| sarcopenia | 0.448 | 0.290-0.691 | <0.001 | 0.320 | 0.187-0.546 | <0.001 |
| Age > 70 years | 1.084 | 0.712-1.650 | 0.708 | |||
| Smoking | 0.890 | 0.585-1.354 | 0.586 | |||
| Drinking | 0.817 | 0.537-1.243 | 0.345 | |||
| BMI>25kg/m2 | 0.742 | 0.484-1.138 | 0.172 | |||
| Prostate volume > 60ml | 0.888 | 0.582-1.354 | 0.581 | |||
| hypertension | 0.890 | 0.585-1.354 | 0.586 | |||
| diabetes | 0.946 | 0.622-1.440 | 0.796 | |||
| Hyperlipidemia | 1.084 | 0.712-1.650 | 0.708 | |||
| Pelvic floor function score | 0.852 | 0.823-0.883 | <0.001 | 0.970 | 0.950-0.991 | 0.005 |
| Influencing factor | Univariable analysis | Multivariable analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | P | OR | 95%CI | P | |
| High-risk prostate cancer | 0.539 | 0.336-0.864 | 0.01 | 0.635 | 0.370-1.088 | 0.098 |
| sarcopenia | 0.175 | 0.105-0.291 | <0.001 | 0.398 | 0.224-0.708 | 0.002 |
| Age > 70 years | 0.499 | 0.307-0.809 | 0.005 | 0.525 | 0.300-0.919 | 0.064 |
| Smoking | 0.650 | 0.406-1.040 | 0.073 | |||
| Drinking | 0.715 | 0.447-1.144 | 0.162 | |||
| BMI>25kg/m2 | 0.872 | 0.541-1.406 | 0.575 | |||
| Prostate volume > 60ml | 1.142 | 0.715-1.824 | 0.679 | |||
| hypertension | 0.650 | 0.406-1.040 | 0.073 | |||
| diabetes | 0.427 | 0.262-0.696 | 0.001 | 0.523 | 0.301-0.910 | 0.022 |
| Hyperlipidemia | 0.499 | 0.307-0.809 | 0.075 | |||
| Pelvic floor function score | 1.099 | 1.067-1.132 | <0.001 | 0.855 | 0.825-0.885 | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutrition and Health in Aging · Frailty in Older Adults · Colorectal Cancer Surgical Treatments
Introduction
Prostate cancer (PCa) represents the most prevalent malignant neoplasm within the male genitourinary system and is the second most common cancer affecting men globally, surpassed only by lung cancer. According to statistics from the World Health Organization (WHO), 1.46 million new cases of prostate cancer were diagnosed in 2022, accompanied by 394,200 reported deaths (1). Radical prostatectomy (RP) is a standard therapeutic intervention for localized prostate cancer and is extensively utilized worldwide. Urinary incontinence (UI) emerges as the most frequent complication post-radical prostatectomy, with incidence rates reported between 5% and 60% (2). Research indicates that the likelihood of urinary incontinence escalates with advancing patient age, thereby substantially affecting both quality of life and confidence in treatment outcomes (3, 4).
Sarcopenia is a condition characterized by a progressive and generalized decline in skeletal muscle mass and strength, which substantially increases the risk of adverse health outcomes (5). The prevalence of sarcopenia escalates with advancing age, with statistical data indicating a prevalence of approximately 5% to 13% among individuals aged 60 to 70 years, and 11% to 50% among those aged over 80 years (6). In cancer patients, heightened protein catabolism and diminished protein synthesis significantly augment the incidence of sarcopenia (7). The prevalence of cancer-associated sarcopenia ranges from 12.5% to 72.2%, adversely impacting the quality of life of cancer patients and being closely linked to cancer prognosis (8). Meta-analyses reveal that the overall incidence of sarcopenia in patients with prostate cancer is approximately 43%, with early-stage prostate cancer patients exhibiting an incidence rate of about 31.8% (9). Research suggests that a reduction in pelvic muscle mass and strength may be associated with the onset of urinary incontinence following radical prostatectomy for prostate cancer (10). Consequently, this study was designed to investigate the prevalence of sarcopenia among patients with prostate cancer and to examine its impact on the incidence of urinary incontinence following radical prostatectomy.
Materials and methods
Patients
This study was designed prospectively and received approval from the Ethics Committee of Lishui Central Hospital in Zhejiang Province, China. Initially, 385 patients diagnosed with prostate cancer were recruited, all of whom underwent laparoscopic radical prostatectomy performed by the same surgeon between January 2022 and December 2023. A postoperative follow-up period of six months was implemented, during which clinical data were systematically collected. The inclusion criteria comprised a biopsy-confirmed diagnosis of prostate adenocarcinoma, imaging evidence of localized prostate cancer, and an anticipated life expectancy exceeding ten years. Exclusion criteria encompassed a history of lower urinary tract surgery, mental illness, severe comorbidities precluding surgical tolerance, spinal cord injury or other neurological disorders, pelvic floor dysfunction, inability to comply with follow-up requirements, and unwillingness to participate in the study. Based on these criteria, 35 patients were excluded, resulting in a final cohort of 350 prostate cancer patients included in the study. The cohort of 350 patients was stratified into two groups—those with sarcopenia and those without—according to established sarcopenia criteria. Each patient underwent laparoscopic radical prostatectomy performed by the same surgeon, and postoperative outcomes, specifically the incidence of urinary incontinence and recovery status, were monitored over a six-month period. Figure 1 illustrates the flowchart detailing the criteria for patient inclusion and exclusion in this study.
Flowchart of patients in this study.
Methods
Upon admission, all patients diagnosed with prostate cancer underwent comprehensive evaluations, including a full abdominal dual-energy computed tomography (CT) scan, a grip strength assessment, and a walking test to evaluate sarcopenia, alongside pelvic floor function tests to assess pelvic floor status. Following the exclusion of any surgical contraindications, a single surgeon conducted a non-nerve-sparing laparoscopic radical prostatectomy, incorporating routine urethral suspension and posterior urethral reconstruction. Postoperative follow-up was conducted for a duration of six months. The one-hour pad test was employed to assess the incidence of urinary incontinence immediately after the surgical procedure, as well as at three and six months postoperatively, in order to analyze the influence of sarcopenia on urinary incontinence subsequent to laparoscopic radical prostatectomy.
Assessments
Diagnostic criteria for sarcopenia are as follows: ① Muscle mass: Skeletal muscle index at the L3 vertebra level is less than 40.8 cm²/m²; ② Muscle strength: Grip strength is less than 28 kg; ③ Physical function: Walking speed is ≤ 1 m/s.
Diagnostic categories:Presumptive sarcopenia: Criterion①; Sarcopenia: Criterion①+②or Criterion①+③; Severe sarcopenia: Criterion①+②+③ (11); Pelvic floor function assessment: The MaLiande biofeedback device(Nanjing McLand Medical Technology Co., LTD,Nanjing,China)is used to evaluate a patient’s pelvic floor function; a score of less than 80 indicates the presence of pelvic floor dysfunction, with lower scores suggesting poorer pelvic floor function.
One-hour pad test: Place a pre-weighed dry pad at the perineum; during the initial 15 minutes, the patient drinks 500ml of water and rests in bed. For the next 30 minutes, the patient walks and goes up and down stairs. In the subsequent 15 minutes, the patient should sit and stand 10 times, cough forcefully 10 times, run for 1 minute, pick up 5 small objects from the floor, and then wash hands with tap water for 1 minute. At the end of the 60-minute test, weigh the pad and instruct the patient to urinate and record the urine volume. Result interpretation: Negative: <1g, mild leakage: 2-10g, moderate leakage: 10-50g, severe leakage: >50g.
Statistical analysis
SPSS22.0 was used to perform statistical analysis on the data. Normally distributed measurement data were expressed as mean ± standard deviation (x ± SD), independent sample t test was used for comparison between groups, and skewed distribution measurement data were expressed as median (minimum value~maximum value), using the Mann-Whitney U test. Categorical data are expressed as percentages (%) and analyzed using the x^2^ test or Fisher’s exact test. Univariable and multivariable logistic regression analyses were performed to identify influence factors of UI 3 and 6 months after surgery. P<0.05 is considered statistically significant.
Results
Comparison of baseline data between the two groups
There were no significant differences between the two groups in body mass index, smoking, drinking, prostate volume, education level, type of medical insurance, PSA, Gleason score, TMN staging and neoadjuvant therapy(P > 0.05).There were statistical differences in age, income, diabetes rate and pelvic floor function scores between the two groups(P<0.05).as shown in Table 1.
The incidence of sarcopenia in prostate cancer patients with different risk stratifications
The incidence of sarcopenia among all prostate cancer patients is 40.86%. Among them, the incidence of sarcopenia in patients with low to intermediate-risk prostate cancer is 34.42%, while it is 51.11% in high-risk prostate cancer patients. There is a statistically significant difference in the incidence of sarcopenia among prostate cancer patients with different risk stratifications (P<0.05). See Table 2 and Figure 2 for details.
Skeletal muscle area at L3 vertebral level (No Sarcopenia vs Sarcopenia:13788.2mm2vs 5391.1mm2).
Comparison of occurrence of urinary incontinence between two groups
The postoperative urinary incontinence rates for all patients immediately, at 3 months, and at 6 months were 72%, 47.81%, and 28%, respectively. Among sarcopenia patients, the rates were 82.52%, 65.02%, and 37.06%, while for non-sarcopenia patients, the rates were 64.73%, 35.75%, and 21.74%, respectively. The incidence of postoperative urinary incontinence in sarcopenia patients was significantly higher than in non-sarcopenia patients (P<0.05). For more details, see Table 3 and Figure 3.
Occurrence of urinary incontinence in different risk prostate cancer.
Comparison of postoperative urinary incontinence in patients with different risk stratified prostate cancer
The incidence of urinary incontinence immediately post-operatively and at 3 months and 6 months for patients with low to intermediate-risk prostate cancer was 72%, 47.81%, and 28%, respectively, whereas for high-risk prostate cancer patients, it was 82.52%, 65.03%, and 37.06%, respectively, significantly higher than that of low to intermediate-risk patients (P<0.05). Refer to Table 4 and Figure 4 for details. Among low to intermediate-risk prostate cancer patients with sarcopenia, the incidence of urinary incontinence immediately post-operatively and at 3 months was significantly higher at 68.92% and 54.05% compared to those without sarcopenia, which was 54.61% and 21.28% (P<0.05). However, there was no significant difference in the incidence of urinary incontinence between the two groups at 6 months post-operatively, being 18.92% and 14.89%, respectively (P>0.05). For high-risk patients with sarcopenia, the incidence of urinary incontinence immediately post-operatively and at 6 months was higher compared to those without sarcopenia, at 97.10%, 56.52% and 86.36%, 36.36%, respectively (P<0.05) (Figure 5 and Table 5).
Occurrence of urinary incontinence in both groups.
Comparison of postoperative urinary incontinence in patients with different risk stratified prostate cancer.
Analysis of risk factors of urinary incontinence after radical prostate cancer surgery
Univariate and multivariate logistic regression analyses for postoperative urinary incontinence at 3 and 6 months showed that at 3 months, high-risk prostate cancer, sarcopenia, and pelvic floor function scores were risk factors for urinary incontinence after radical prostatectomy. At 6 months, univariate analysis revealed high-risk prostate cancer, sarcopenia, pelvic floor function scores, diabetes, and advanced age as risk factors, while multivariate analysis identified sarcopenia, pelvic floor function scores, and diabetes as independent risk factors for urinary incontinence. See Tables 6, 7 for details.
Discussion
Laparoscopic radical prostatectomy is a primary therapeutic intervention for localized prostate cancer. A significant postoperative complication of this procedure is urinary incontinence, which adversely impacts patients’ quality of life and can induce anxiety and concern among patients and their families, potentially leading to doubts regarding the surgery’s overall efficacy (12). The etiology of postoperative urinary incontinence is multifaceted, with numerous studies indicating that factors such as tumor staging, surgical techniques, preservation of pelvic floor structures, and retention of functional urethra influence its incidence (13–16). Sarcopenia, a condition prevalent among cancer patients, significantly impairs skeletal muscle function and has been shown in multiple studies to affect the entire continuum of prostate cancer treatment, particularly in advanced stages (17, 18). Does sarcopenia affect urinary incontinence following radical prostate cancer surgery? Our study examined the presence of sarcopenia in prostate cancer patients and its impact on urinary incontinence post-surgery. Our study identified that 40.86% of prostate cancer patients exhibited sarcopenia, a finding consistent with previous research, where meta-analyses have reported an overall sarcopenia prevalence of approximately 43% among prostate cancer patients, and an incidence rate of around 31.8% in early-stage cases (9). Comparative analysis between prostate cancer patients with and without sarcopenia revealed no statistically significant differences in tumor characteristics, body mass index (BMI), educational attainment, type of medical insurance, smoking and alcohol consumption history, or the presence of coronary heart disease and hyperlipidemia. Nonetheless, individuals in the sarcopenia cohort were generally older, had lower income levels, exhibited a higher prevalence of diabetes, and demonstrated reduced pelvic floor function scores compared to those without sarcopenia. Literature (19) suggests that the incidence of sarcopenia escalates with advancing age, and socioeconomic status may influence nutritional intake, thereby affecting sarcopenia prevalence. Additionally, diabetes has been implicated in the deterioration of muscle function, thereby exacerbating sarcopenia. Our findings corroborate existing evidence (20) suggesting that sarcopenia adversely impacts pelvic floor muscle function.
In this study, the overall incidence of sarcopenia among prostate cancer patients was found to be 40.86%. Notably, the incidence was significantly elevated in patients with high-risk prostate cancer compared to those with medium or low risk, aligning with findings from previous research. Several studies (8, 9) have indicated that the prevalence of sarcopenia is markedly higher in patients with advanced-stage tumors compared to those with early-stage tumors. This phenomenon may be attributed to the progressive catabolic effects of the tumor, which result in a reduction of the patient’s muscle mass. Longitudinal studies on prostate cancer patients have demonstrated that, as the disease advances, the probability of developing sarcopenia increases substantially during the course of treatment.
In this study, we observed that the incidence of immediate urinary incontinence following radical prostatectomy was as high as 72% among all patients. However, with the progression of postoperative time, symptoms of urinary incontinence showed gradual improvement, with the incidence decreasing to approximately 28% at six months post-surgery, aligning with findings from previous studies (12). Some researchers have employed robot-assisted radical prostatectomy, achieving long-term postoperative urinary incontinence rates of less than 10% (21). We conducted a further analysis of patients based on the presence of sarcopenia. Patients with prostate cancer who also had sarcopenia exhibited higher rates of both immediate postoperative urinary incontinence and incontinence at six months compared to those without sarcopenia. This suggests that sarcopenia increases the likelihood of urinary incontinence following radical prostatectomy, corroborating previous research findings (22). In patients with low to intermediate-risk prostate cancer, the presence of sarcopenia is associated with a significantly increased incidence of short-term postoperative urinary incontinence compared to those without sarcopenia. However, at six months postoperatively, the prevalence of urinary incontinence converges between the two groups, suggesting that sarcopenia does not have a significant long-term impact on urinary incontinence in this patient cohort, although it does adversely affect short-term urinary control recovery following surgery. Conversely, in patients with high-risk prostate cancer, those with sarcopenia exhibit a consistently higher incidence of urinary incontinence at all evaluated time points compared to their non-sarcopenic counterparts. This observation implies that sarcopenia exerts a more pronounced influence on urinary incontinence in high-risk patients, potentially due to the more extensive surgical resection required in this group, which may compromise pelvic floor muscle function, thereby increasing the likelihood of postoperative urinary incontinence and impeding the restoration of urinary function.
In this study, we conducted an analysis of the risk factors associated with postoperative urinary incontinence among all patients. At three months following surgery, both univariate and multivariate regression analyses identified high-risk prostate cancer, sarcopenia, and pelvic floor dysfunction as independent risk factors for urinary incontinence. In comparison to medium- and low-risk prostate cancer, high-risk prostate cancer necessitates a more extensive surgical excision, which results in greater disruption to the pelvic floor structure and function, thereby elevating the risk of postoperative urinary incontinence. At six months following surgery, our analysis of risk factors for urinary incontinence identified, through univariate analysis, that high-risk prostate cancer, sarcopenia, age over 70, diabetes, and pelvic floor dysfunction were associated with increased risk. However, multivariate analysis revealed that only sarcopenia, diabetes, and pelvic floor dysfunction emerged as independent risk factors, whereas prostate cancer risk stratification and age did not significantly influence the long-term incidence of urinary incontinence. Diabetes is known to affect peripheral vascular and nerve function, which in turn can impair skeletal muscle function. Research indicates that skeletal muscle function deteriorates more rapidly in diabetic patients compared to non-diabetic individuals (23). Sarcopenia has a substantial impact on the function and recovery of pelvic floor muscles. The pelvic floor function score serves as a quantitative measure of pelvic muscle function, with the score reflecting the condition of pelvic muscle function and influencing the likelihood of postoperative urinary incontinence.
The study investigated the incidence of urinary incontinence following laparoscopic radical prostatectomy and examined the associated risk factors. The findings identified sarcopenia as an independent risk factor for persistent postoperative urinary incontinence. Nonetheless, the analysis process presented certain limitations. Specifically, the severity of sarcopenia was not stratified, leaving it unclear whether varying degrees of sarcopenia exert differential impacts on the incidence of urinary incontinence. Furthermore, the factor analysis concerning the risk of urinary incontinence lacked comprehensiveness, potentially influencing the study’s outcomes. Despite these limitations, the data collection and analysis were executed with rigor, rendering the findings reliable. The recognition of sarcopenia as an independent risk factor for urinary incontinence post-radical prostatectomy can inform strategies for the prevention and management of urinary incontinence in this patient population.
In conclusion, this study determined that approximately 40% of prostate cancer patients exhibit sarcopenia, with a notably higher prevalence among those with high-risk prostate cancer compared to individuals with low to medium risk. Sarcopenia serves as an independent risk factor impacting the incidence of urinary incontinence following radical prostatectomy and influences the recovery trajectory of incontinence. Consequently, In patients with sarcopenia, implementing perioperative rehabilitation strategies may reduce the incidence of postoperative incontinence, bearing significant clinical implications for improving treatment efficacy and the quality of life for patients experiencing urinary incontinence after laparoscopic radical prostatectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F Laversanne M Sung H Ferlay J Siegel RL Soerjomataram I. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2024). doi: 10.3322/caac.21834 38572751 · doi ↗ · pubmed ↗
- 2Machioka K Kadono Y Naito R Nakashima K Iijima M Kawaguchi S. Evaluating urinary incontinence before and after radical prostatectomy using the international consultation on incontinence questionnaire-short form. Neurourol Urodyn. (2019) 38:726–33. doi: 10.1002/nau.23907 30576037 · doi ↗ · pubmed ↗
- 3Nam KH Shim J Kim HY. Factors influencing self-esteem after radical prostatectomy in older adult patients. Geriatr Nurs. (2022) 43:206–12. doi: 10.1016/j.gerinurse.2021.11.023 34923311 · doi ↗ · pubmed ↗
- 4Zeng J Zhou S Luan W Du Y Wu J. Symptom trajectories and influencing factors of prostate cancer following radical prostatectomy in Chinese patients. Ann Palliat Med. (2021) 10:7747–58. doi: 10.21037/apm-21-1229 34353062 · doi ↗ · pubmed ↗
- 5Zhang FM Wu HF Shi HP Yu Z Zhuang CL. Sarcopenia and Malignancies: epidemiology, clinical classification and implications. Ageing Res Rev. (2023) 91:102057. doi: 10.1016/j.arr.2023.102057 37666432 · doi ↗ · pubmed ↗
- 6Vogele D Otto S Sollmann N Haggenmüller B Wolf D Beer M. Sarcopenia - definition, radiological diagnosis, clinical significance. Rofo. (2023) 195:393–405.36630983 10.1055/a-1990-0201 · doi ↗ · pubmed ↗
- 7Prado CM Purcell SA Laviano A. Nutrition interventions to treat low muscle mass in cancer. J Cachexia Sarcopenia Muscle. (2020) 11:366–80. doi: 10.1002/jcsm.12525 PMC 711351031916411 · doi ↗ · pubmed ↗
- 8Zhang FM Song CH Guo ZQ Yu Z Weng M Zhou FX. Sarcopenia prevalence in patients with cancer and association with adverse prognosis: A nationwide survey on common cancers. Nutrition. (2023) 114:112107. doi: 10.1016/j.nut.2023.112107 37356170 · doi ↗ · pubmed ↗