Evaluating the Impact of Audits and Re-audits on Adherence to the Ottawa Knee Rules in a High-Volume UK Trauma Centre
Hamza Ahmed, Aima Gilani, Farah Mazhar, Marium Rizwan, Aarish Azeem, Abdur Rehman

TL;DR
This study shows that education significantly improved adherence to the Ottawa Knee Rules for reducing unnecessary knee X-rays in a UK hospital.
Contribution
Demonstrates the effectiveness of educational interventions in improving clinical guideline adherence in trauma care.
Findings
Compliance with OKR criteria increased from 41% to 91% after educational interventions.
Specific indicators like inability to bear weight and isolated patellar tenderness saw significant improvements.
Sustained training and audits are needed to maintain high adherence to clinical guidelines.
Abstract
Background The Ottawa Knee Rules (OKR) are a validated clinical decision-making tool designed to minimise unnecessary radiographs in knee trauma, thereby reducing radiation exposure, optimising resource utilisation, and streamlining patient management. This study audits and re-audits the clinical compliance with OKR in radiography referrals by the Orthopaedic and Emergency Department (ED) teams at Salford Royal NHS Foundation Trust. Methodology A two-cycle retrospective audit was conducted, examining knee X-ray request forms submitted between October 2023 and March 2024 (Cycle 1) and March 2024 and September 2024 (Cycle 2). Each request was evaluated against the OKR criteria and cross-referenced with corresponding clinical notes. Target compliance was 100%. Educational interventions were implemented after Cycle 1 to improve adherence. Results In Cycle 1, only 41% of referrals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
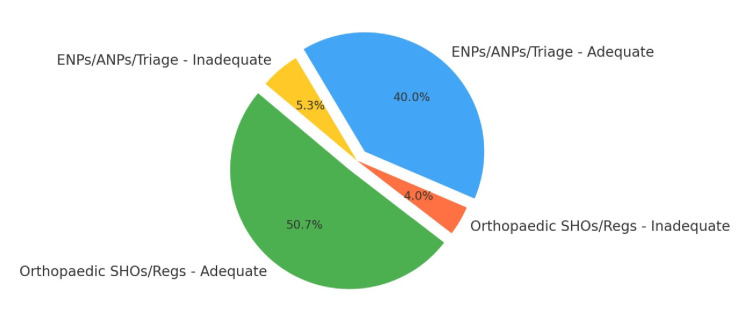 Figure 1
Figure 1| Group | Adequate | % Adequate | Inadequate | % Inadequate |
| Orthopaedic SHOs/Regs | 15 | 35.7% | 27 | 64.3% |
| ENPs/ANPs/Triage | 11 | 52.4% | 10 | 47.6% |
| Group | Adequate | % Adequate | Inadequate | % Inadequate |
| Orthopaedic SHOs/Regs | 38 | 92.9% | 3 | 7.1% |
| ENPs/ANPs/Triage | 30 | 88.2% | 4 | 11.8% |
| Criterion | Cycle 1 | Cycle 2 |
| Age ≥55 years | 52% | 62% |
| Fibular head tenderness | 3% | 68% |
| Isolated patellar tenderness | 13% | 72% |
| Inability to flex to 90° | 3% | 65% |
| Inability to bear weight (four steps) | 14% | 57% |
| At least one criterion met | 41% | 91% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Sports injuries and prevention · Nursing Roles and Practices
Introduction
Trauma-related knee injuries constitute a significant portion of emergency and orthopaedic assessments. Clinical decision-making tools such as the Ottawa Knee Rules (OKR) are essential to prevent unnecessary imaging while maintaining diagnostic accuracy. First developed in Ottawa, Canada, in 1995, OKR have demonstrated excellent sensitivity for identifying clinically significant fractures and have since been validated globally across diverse patient populations [1,2].
The OKR recommend radiographs only when certain post-injury clinical features are present, including advanced age, isolated patellar tenderness, fibular head tenderness, inability to flex the knee to 90 degrees, and inability to bear weight both immediately and in the emergency department for four steps. These rules are endorsed by the National Institute for Health and Care Excellence (NICE) and the Royal College of Radiologists (RCR), particularly within the iRefer Guidelines [3,4].
Despite widespread awareness, anecdotal observations at our institution suggested inconsistent documentation of OKR criteria in imaging requests. This audit aimed to quantify compliance levels, assess documentation adequacy, and implement targeted interventions to address gaps in knowledge and practice.
Materials and methods
Objectives
The audit aimed to assess clinical compliance with the OKR in X-ray referrals for acute knee trauma and evaluate the adequacy of clinical information provided in electronic request forms. A further objective was to determine the effectiveness of an educational intervention in improving compliance, followed by a re-audit to assess subsequent changes.
Study design
A retrospective two-cycle clinical audit was conducted. All knee radiograph requests made via the Electronic Patient Record system for patients presenting with acute knee trauma were included. Clinical notes were accessed and cross-referenced to confirm documentation.
Exclusion criteria
Patients were excluded if they were under 18 years of age, had injuries more than seven days old, presented with altered consciousness, had paraplegia or multiple lower limb fractures, were pregnant, or had only superficial or soft tissue injuries.
Data collection
Cycle 1 was conducted from October 2023 to March 2024 and included 63 patients after applying the exclusion criteria. Cycle 2 was conducted from March 2024 to September 2024 and included 75 patients post-exclusion. Referrals were reviewed for documentation of any OKR criteria. Subgroup analysis was conducted according to referrer designation, which included senior house officers (SHOs), registrars, emergency nurse practitioners (ENPs), advanced nurse practitioners (ANPs), and triage nurses.
Interventions post-Cycle 1
Following the first cycle, several educational interventions were implemented. These included visual aids (posters and leaflets) in clinical areas, presentations during departmental meetings, informal and formal teaching sessions, and email communication summarising the OKR.
Results
Referrer documentation compliance
The adequacy of documentation for each referrer group improved significantly from Cycle 1 to Cycle 2 (Tables 1, 2). Orthopaedic doctors and nurse practitioners both showed notable increases in appropriate documentation of OKR criteria.
Compliance with specific OKR criteria
Substantial improvement was noted across all five OKR criteria between the two cycles (Table 3).
Pie chart: OKR compliance by referrer type (Cycle 2)
Figure 1 shows the OKR documentation compliance of different referrer types in Cycle 2.
OKR documentation compliance by referrer type Cycle 2.OKR: Ottawa Knee Rules; SHO: senior house officer; ENP: emergency nurse practitioner; ANP: advanced nurse practitioner
Chi-square test for association
A chi-square test revealed a statistically significant association between the audit cycle and adequacy of OKR documentation (p < 0.01), suggesting the educational interventions were effective in improving compliance.
Interpretation of audit cycles
In Cycle 1, only 41% of radiograph referrals documented at least one OKR criterion. Among these, fibular head tenderness and inability to flex to 90° were rarely noted (both 3%), indicating significant knowledge or documentation gaps. In contrast, age ≥55 years had the highest frequency (52%), likely due to its routine presence in demographic data.
Following the educational intervention, Cycle 2 showed a marked improvement to 91% compliance. The most dramatic improvements were seen in isolated patellar tenderness (from 13% to 72%), fibular head tenderness (from 3% to 68%), and the inability to flex (from 3% to 65%). These suggest the interventions effectively addressed the components of the OKR that were previously ignored or not paid attention to.
Referrer comparison
Orthopaedic doctors showed a considerable improvement from 35.7% to 92.9% in portraying adequate documentation. Nurse practitioners and triage staff also improved significantly (52.4% to 88.2%), indicating that the multi-professional format of training was successful.
Discussion
This audit reinforces the clinical importance of the OKR and demonstrates that structured, low-cost educational interventions can yield significant improvements in adherence among both medical and nursing staff. The increase in documentation compliance from 41% to 91% suggests a substantial shift in the behaviour with regards to clinical practice, aligning with previous findings that multidisciplinary reinforcement enhances clinical decision tool adoption [5-7].
Several studies have emphasised the sensitivity of OKR (nearing 100%) for identifying fractures, with notable reductions in unnecessary radiographs when applied systematically [6]. Our findings throw light on those of Beutel et al. [1], who highlighted inconsistent documentation as a key barrier to OKR compliance. This was in particular for high-volume trauma centres. Similar to our audit, their intervention-driven study noted that education significantly increased both documentation rates and appropriate imaging decisions.
In addition to this, the improvement in fibular head tenderness and patellar tenderness documentation suggests that these lesser-known OKR elements are not something that people look at in routine, and hence, they require deliberate teaching. This mirrors findings by Cheung et al. [5], who identified these specific criteria as frequently overlooked in practice. Therefore, our results provide evidence that education must target not just the existence of OKR but the application of each component individually.
The greater improvement seen among orthopaedic junior doctors compared to ENPs and triage nurses may also reflect variation in prior exposure to clinical decision rules. Jalili and Gharebaghi [8] found that ongoing mentorship and involvement in audit processes reinforced longer-term compliance, a principle which could be applied to sustain our target goal of 100% compliance. This will lead to reductions in radiographs that are not needed, which is necessary to prevent radiation exposure to the patients [9].
Despite these improvements, 9% of Cycle 2 referrals still lacked adequate documentation. This may be explained by the rapid rotation of junior medical staff, variable IT proficiency, or insufficient reinforcement at the point of care. Integration of OKR prompts into electronic request systems, as recommended by NICE RCR’s iRefer guidelines [3,4], could further standardise practice and reduce reliance on individual memory.
Another noteworthy limitation is our reliance on documentation rather than real-time observation, which may have underestimated true clinical compliance. While this is a common limitation in retrospective audits [10], future studies might incorporate direct observation or simulation-based assessments to summarise the findings. Finally, the single-centre nature of our audit limits generalizability; however, the simplicity of the intervention and consistency of outcome improvements suggest that similar models could be replicated in comparable trauma units.
Conclusions
This study demonstrates that simple, targeted educational interventions can significantly enhance clinical adherence to the OKR within acute trauma settings. By improving documentation and compliance among both medical and nursing staff, we observed a marked reduction in unnecessary radiographic investigations, and this was in line with evidence-based guidelines. The improvements observed across all five OKR criteria, particularly in the historically under-documented areas of fibular head tenderness and patellar tenderness, underscore the effectiveness of complex educational approaches. These results not only validate the OKR as a reliable tool for clinical decision-making but also highlight the critical role of continuous professional development, visual prompts, and regular audit cycles in ensuring we comply with the rules. We recommend that further steps include integration of OKR prompts into electronic requesting systems, mandatory induction teaching for new staff, and institutional policy reinforcement through local clinical governance. A standardised audit tool, such as the checklist provided in the appendix, may assist other departments in adopting similar quality improvement strategies. Ultimately, adopting consistent OKR adherence can streamline patient care, reduce healthcare costs, and enhance patient safety.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The Ottawa Knee Rule: examining use in an academic emergency department West J Emerg Med Beutel BG Trehan SK Shalvoy RM Mello MJ 3663721320122325171710.5811/westjem.2012.2.6892 PMC 3523897 · doi ↗ · pubmed ↗
- 2Validation of the Ottawa Knee Rules Ann Emerg Med Emparanza JI Aginaga JR 3643683820011157479110.1067/mem.2001.118011 · doi ↗ · pubmed ↗
- 3i Refer Guidelines: T 22 Knee Trauma Royal College of Radiologists London Royal College of Radiologists 2017 https://www.rcr.ac.uk/media/bgtlnafo/rcr-audits_radiography-for-knee-trauma-compliance-with-the-ottawa-knee-rule_july-2022.docx
- 4NICE Clinical Knowledge Summary. Knee pain - assessment 6 2025 2025 https://cks.nice.org.uk/topics/knee-pain-assessment/
- 5Diagnostic accuracy and reproducibility of the Ottawa Knee Rule vs the Pittsburgh Decision Rule Am J Emerg Med Cheung TC Tank Y Breederveld RS Tuinebreijer WE de Lange-de Klerk ES Derksen RJ 6416453120132339933210.1016/j.ajem.2012.11.003 · doi ↗ · pubmed ↗
- 6The Ottawa knee rules - a useful clinical decision tool Aust Fam Physician Yao K Haque T 223224412012 https://pubmed.ncbi.nlm.nih.gov/22472684/22472684 · pubmed ↗
- 7Validation of the Ottawa Knee Rule in children: a multicenter study Ann Emerg Med Bulloch B Neto G Plint A 48554220031282712310.1067/mem.2003.196 · doi ↗ · pubmed ↗
- 8Validation of the Ottawa Knee Rule in Iran: a prospective study Emerg Med J Jalili M Gharebaghi H 8498512720102037873910.1136/emj.2009.080267 · doi ↗ · pubmed ↗