Molecular identification of Mycobacterium bovis in patients with tuberculosis attending a tertiary care hospital in South India
Imola Jamir, Noyal Mariya Joseph, Rachana Kannambath, Pradeep Kumar

TL;DR
The study found that Mycobacterium bovis is rare among tuberculosis cases in a South Indian hospital, suggesting it poses little public health risk there.
Contribution
The paper provides empirical evidence on the low prevalence of M. bovis in TB patients in South India using molecular diagnostics.
Findings
All pulmonary TB samples were identified as M. tuberculosis or M. canettii.
Only 1% of extrapulmonary TB samples were M. bovis BCG.
M. bovis appears to be uncommon in the studied Indian population.
Abstract
Mycobacterium (M.) bovis is a member of Mycobacterium tuberculosis complex (MTBC). Clinical infection caused by M. bovis is indistinguishable from other MTBC and could pose a potential challenge for control of TB epidemic due to its zoonotic nature. Availability of reliable molecular diagnostic methods such as Genotype MTBC based on line probe assay (LPA) paves way for reliable differentiation of M. bovis from other MTBC. To determine the proportion of Mycobacterium bovis among the Mycobacterium tuberculosis complex isolates from patients with tuberculosis. In our study, we analysed MGIT positive cultures and performed Line probe assay (LPA) for identification of MTBC isolates. Total of 206 patient samples were taken, 104 pulmonary and 102 from extrapulmonary sites. M.tuberculosis/M.canettii was isolated in all pulmonary specimens (100%). Among 102 extrapulmonary samples, 99 % was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
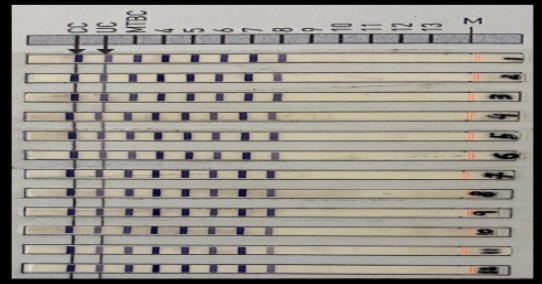 Figure 1
Figure 1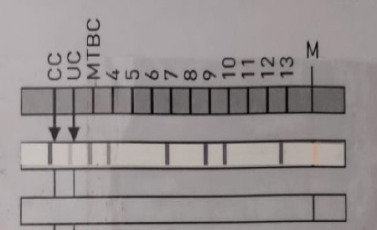 Figure 2
Figure 2| Pulmonary | Extrapulmonary | |||
|---|---|---|---|---|
| Frequency | Percent (%) | Frequency | Percent (%) | |
| 0-20 | 9 | 8.7 | 10 | 9.8 |
| 21-40 | 34 | 32.7 | 46 | 45.1 |
| 41-60 | 45 | 43.3 | 35 | 34.3 |
| 61-80 | 16 | 15.4 | 9 | 8.8 |
| 81-100 | - | - | 2 | 2.0 |
|
|
|
|
|
|
| Pulmonary specimens | ||
|---|---|---|
| Frequency | Percent ( %) | |
| BAL | 5 | 4.8 |
| Bronchial wash | 1 | 1.0 |
| Endotracheal aspirate | 2 | 1.9 |
| Gastric aspirate | 2 | 1.9 |
| Sputum | 94 | 90.4 |
|
|
|
|
|
| ||
|
|
| |
| Pus | 21 | 20.6 |
| Tissue biopsy | 3 | 2.9 |
| Bone marrow | 1 | 1.0 |
| Bone | 1 | 1.0 |
| CSF | 27 | 26.5 |
| Cyst fluid | 1 | 1.0 |
| Drain fluid | 1 | 1.0 |
| LN FNAC | 3 | 2.9 |
| LN Biopsy | 1 | 1.0 |
| Lung biopsy | 2 | 2.0 |
| Pericardial fluid | 1 | 1.0 |
| Pleural fluid | 36 | 35.3 |
| Urine | 4 | 3.9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Mycobacterium research and diagnosis · Hepatitis B Virus Studies
Introduction
Mycobacterium bovis is one of the member of the Mycobacterium tuberculosis complex (MTBC) which comprises of Mycobacterium tuberculosis (MTB), M. africanum, M. canettii, M. bovis, M. bovis BCG, M. microti, M. caprae, M. pinnipedii, M. orygis. The clinical infection caused by M. bovis is indistinguishable from those caused by other members of MTBC. 1 Tuberculosis (TB) caused by the different members of the MTBC is a global problem. The End TB strategy by WHO aims to end the global tuberculosis (TB) epidemic by 2035.2 However, M. bovis could pose a potential challenge for the control of TB epidemic, because of its zoonotic nature. In the rural areas of India, people often live in close proximity to cows (the natural host of M. bovis) which increases the risk of transmission of M. bovis from animals to humans. Moreover, M. bovis is intrinsically resistant to pyrazinamide (one of the first line antitubercular drug), which may pose additional challenge. 1 Awareness of the magnitude of problem due to M. bovis infection in humans is very important to plan appropriate strategies at the national level for control of TB in India. The incidence of tuberculosis caused by M. bovis in India is unknown or underestimated as the routinely used diagnostic methods are not capable of differentiating M. bovis from the other members of MTBC including M. tuberculosis. 1 Availability of reliable molecular diagnostic methods such as Genotype MTBC kit based on line probe assay (LPA) paves way for reliable differentiation of M. bovis from other members of MTBC. In our study, we analysed MGIT positive cultures and performed line probe assay for identification of MTBC isolates.
Methods
Study design and duration
A hospital-based cross-sectional study was performed in Department of Microbiology after approval from the Institutional Ethics Committee. The laboratory confirmed MTBC isolates from pulmonary and extrapulmonary TB patients were included after satisfying the inclusion and exclusion criteria. A total of 206 patient samples were taken, of which 104 was pulmonary and 102 from extrapulmonary sites. All pulmonary and extrapulmonary MTBC isolates were taken consecutively. Demographic patient details such as age, gender and specimen type were noted by a Senior Resident posted in the laboratory and provided in a de-identified manner. Inclusion criteria was MTBC isolates from pulmonary and extrapulmonary TB patients during the study period (January 2020 to December 2021). Exclusion criteria was repeat isolates from the same patient. The sample size based on the expected prevalence of 12.6 % (Bapat PR et al, 2017) 3 and the absolute precision as 4 % and confidence level at 95% was 265. However, due to limited funding, we studied a sample size of 206 MTBC isolates. Pulmonary samples such as sputum, BAL and extrapulmonary samples like CSF, pleural fluid, urine, lymph node aspirate, pus, tissue bits, ascitic fluid are included in this study.
Sample processing
Collected specimens were either processed immediately or stored at 2-8°C until processed. First, samples underwent decontamination by NALC-NaOH method and the sediments were then inoculated into BACTEC MGIT (Mycobacteria growth indicator tube) 960 and incubated at 37°C. The MGIT tubes flagged as positive were identified as MTBC using rapid detection of MPT64 antigen. All the isolates were then tested using Genotype MTBC line probe assay (LPA) for identification of M. bovis and other members of MTBC.
Results
Age and gender distribution
A total of 206 patient samples were included in the study, of which 104 was pulmonary and 102 extrapulmonary samples. Of 104 patients with PTB, 73 (70.2 %) were male and 31 (29.8 %) were female. Mean age of the patients with pulmonary tuberculosis (PTB) was 43.10 ± 16.01 (range, 7 to 75). Of 102 patients with EPTB, 59 (57.8%) were male and 43 (42.2 %) were female. Mean age of the patients with extrapulmonary tuberculosis (EPTB) was 40.19 ± 16.95 (range, 1 to 85). Age distribution of patients with MTBC isolation from Pulmonary and Extra-pulmonary specimens is given in Table 1.
MTBC speciation
The distribution of MTBC species in pulmonary and extrapulmonary specimens is summarised in Table 2. M. tuberculosis/M. canettii was isolated in all the pulmonary specimens (100%). Among the 102 extrapulmonary samples, 99 % (101/102) was identified as M. tuberculosis/M. canettii, and 1 % (1/102) as M. bovis BCG from lymph node fine needle aspiration cytology (LN FNAC), Figure 1,2. This LN FNAC sample was from a 5 month-old female child with disseminated BCGiosis.
Results of LPAConjugate control (CC): documents efficiency of conjugate binding and substrate reactionUniversal control (UC): positive for all mycobacteria and gram-positive bacteria with high G+C contentMTBC: positive for all members of MTBCBands in 1-8: M. tuberculosis/M. canettii
LPA identification of M bovis BCG from LN FNAC sample
Discussion
This cross-sectional study was performed to assess the proportion of M. bovis among members of MTBC in laboratory confirmed MTBC isolates from pulmonary and extrapulmonary TB patients. M. bovis is zoonotic in nature and there is risk of transmission, especially in rural areas where people live in close proximity to cows. There is no national level surveillance for M. bovis and only a few studies have been conducted. Simultaneous control for bovine TB is required to eliminate tuberculosis in humans. The study was done using Genotype MTBC kit based on line probe assay for identification of M. bovis.
A total of 206 patient samples were included, of which 104 was pulmonary and 102 from extrapulmonary sites. In our study, the mean age group was 43.10 ± 16.01 and 40.19 ± 16.95 in pulmonary and extrapulmonary TB respectively. The most common age group was 41-60 years (43.3 %) in pulmonary and 21-40 years (45.1%) in extra-pulmonary TB patients. In other Indian studies, the most prevalent age group in pulmonary and extrapulmonary tuberculosis was 20 to 29 years;4 in another, 20 to 39 years;5 and in a third, 25 to 34 years.6 In a study by Sarpal SS et al, mean age of patients was 35.92 ± 15.42 and majority of patients belonged to age group of 25-34 years. 7
In the epidemiology of tuberculosis, age is a critical determinant. TB patients' symptoms, risk of disease progression and treatment results vary with age, most likely due to changes in the immunological response.8 The risk of disease following primary TB infection is highest in newborns (under 4 years old) and gradually decreases until it reaches a trough at the age of 5 to 10 years. There is a significant rise in risk during early adulthood and adolescent period (ages 15 to 19 years), with second peak occurring around the age of 20 to 30 years. 9 Disseminated TB, such as miliary TB and TB meningitis are frequent in early infancy. Elderly persons, on the other hand, acquire immunological senescence and those with latent TB infection (LTBI) have a higher chance of developing active TB.8,9
In our study, out of total 206 patients, 74 (36.0 %) were female and 132 (64.0 %) were male. Of the 104 pulmonary samples, 31 (29.8 %) were female and 73 (70.2 %) were male samples. In the 102 extra-pulmonary samples, 43 (42.2 %) were female and 59 (57.8%) were male samples. This is in concordance with a study from South India where pulmonary samples were from 34 % females and 66 % males; and extra-pulmonary samples from 45 % females and 55 % males. 4 Another study from North India shows similar findings, with 36.1 % female and 63.9 % male prevalence in pulmonary and extra-pulmonary samples. 5 Also, in a study conducted in West Bengal, 30.7 % of TB patients were female and 69.3 % were male.10 Various age groups and regions of the world have gender disparities, the cause of which is unknown. The male preponderance for tuberculosis in this study is accordant with data from other nations, and it may indicate work-related, behavioural, or immunological risk factors.
In our research, M. tuberculosis/M. canettii was the most prevalent species in pulmonary (100 %) and extrapulmonary (99 %) samples. M. bovis BCG was identified from one LN FNAC sample and no other mycobacteria species were identified. A molecular epidemiological surveillance study conducted in a tertiary care centre in Southern India showed similar findings. In that, of 940 (548 pulmonary and 392 extrapulmonary samples) isolates from positive mycobacteria MGIT tubes, wild-type M. bovis was not identified. The most common MTBC detected was M. tuberculosis (97.1 %), followed by M. orygis (0.7%) and M. bovis BCG (0.5%); NTM accounted for 1.6 %. 4 A recent study in China was done on pulmonary samples to identify M. bovis. Similar to our study, no M. bovis isolation was found.11
Based on earlier studies from various developing countries, it was estimated 2.1% of pulmonary tuberculosis and 9.4% of extrapulmonary tuberculosis was due to M. bovis. 12 Recent estimates suggest about 3.1% of human TB globally are caused by M. bovis. In the developing countries, 5–10% of the human TB cases in adults and 30% of pediatric TB cases are due to M. bovis. 13 In the rural areas of UK, where cattle rearing is common, M. bovis was responsible for 5–8.5% of the pulmonary TB in humans, prior to the bovine tuberculosis eradication programme in the UK. 14 Among the MTBC isolates from human TB cases in Mexico, 69% of the extrapulmonary and 31% of the pulmonary isolates were M. bovis. 15 In a study conducted in Central India, M. bovis was detected in 12.6% of the blood samples from residents of high TB endemic areas. 16 It also was observed that most of these patients had symptoms suggestive of tuberculosis such as fever, cough with expectoration, night sweats and chest pain. M. bovis can cause a clinical presentation similar to that of M. tuberculosis induced TB. 16 In another study conducted among the tribal population of the Melghat region, 2.5% of them were positive for M. bovis and many of them had symptoms consistent with pulmonary tuberculosis.17 However, all of these studies relied on blood serology or PCR rather than the culture isolation of M. bovis, which is the definitive proof of M. bovis infection.
The threat of zoonotic TB to tuberculosis control is becoming more widely recognised. Evidence is emerging that other members of the MTBC, such as M. orygis, may also cause human infections. However, M. bovis is still classified as the primary agent of zoonotic tuberculosis by organisations like the WHO.4 In a recent South Indian study, 7 cases of TB were found to be caused by M. orygis, in concordance with other reports from South Asia.4 M. orygis has also been found in cattle and rhesus monkeys in Bangladesh. These findings suggest that MTBC complex members, other than M. bovis, may be more widespread in cattle in these countries and surveillance studies limited to M. bovis may underestimate the incidence of zoonotic TB. Other MTBC subspecies capable of producing human illness should be included in the operational definition of zoonotic TB. In our study, LPA kit did not cover M. orygis and hence its prevalence cannot be estimated. However, M. bovis was not detected in any of the samples.
The strength of our study is that instead of biochemical assays, a line probe assay (LPA) was utilised for speciation, and it is a quick and accurate diagnostic tool for MTBC speciation. Our research has the following limitations: Due to a lack of financial resources, the sample size is less. Also, the isolates collected may be skewed towards places close to the study site. Hence, to achieve a representative data, more research will have to be conducted in other Indian states.
Conclusion
In our cross-sectional study, M. tuberculosis/M. canettii accounted for 99.5 % of species identified in all samples. M. bovis BCG was identified from one lymph node FNAC sample. In our study, there was no pulmonary or extrapulmonary tuberculosis infection by M. bovis. This, along with another study in Southern India by Duffy et al., 4 suggests that zoonotic TB by M. bovis may not be as prevalent in India and hence may not constitute a significant risk to public health in India.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lombardi G Botti I Pacciarini ML Boniotti MB Roncarati G Monte PD Five-year surveillance of human tuberculosis caused by Mycobacterium bovis in Bologna, Italy: an underestimated problem Epidemiology & Infection 20171453035303910.1017/S 095026881700199628879829 PMC 9152750 · doi ↗ · pubmed ↗
- 2WHO Global tuberculosis report 20152015 WHO Available from: http://apps.who.int/iris/bitstream/10665/191102/1/9789241565059_eng.pdf?ua=1
- 3Bapat P R Dodkey R S Shekhawat S D Husain A A Nayak A R Kawle A P Kashyap R S Prevalence of zoonotic tuberculosis and associated risk factors in Central Indian populations Journal of Epidemiology and Global Health 20177277283(2017). 10.1016/j.jegh.2017.08.00729110869 PMC 7384573 · doi ↗ · pubmed ↗
- 4Duffy SC Srinivasan S Schilling MA Stuber T Danchuk SN Michael JS Venkatesan M Bansal N Maan S Jindal N Chaudhary D Reconsidering Mycobacterium bovis as a proxy for zoonotic tuberculosis: a molecular epidemiological surveillance study The Lancet Microbe 2020 Jun 112e 66S 73(2020). 10.1016/S 2666-5247(20)30038-032642742 PMC 7325494 · doi ↗ · pubmed ↗
- 5Sarpal S S Goel N K Kumar D Janmeja A K Gender disparities in retreatment patients of tuberculosis: A north Indian study Journal of Natural Science, Biology, and Medicine 2015 Jan 6163(2015). 10.4103/0976-9668.14908725810636 PMC 4367069 · doi ↗ · pubmed ↗
- 6Siddaiah A Ahmed M N Kumar A M VD'Souza G Wilkinson E Maung T M Rodrigues R Tuberculosis notification in a private tertiary care teaching hospital in South India: a mixed-methods study BMJ Open 2019 Feb 192e 023910(2019). 10.1136/bmjopen-2018-023910 PMC 637751830782889 · doi ↗ · pubmed ↗
- 7Sarpal S S Goel N K Kumar D Janmeja A K Treatment outcome among the retreatment tuberculosis (TB) patients under RNTCP in Chandigarh, India Journal of Clinical and Diagnostic Research: JCDR 2014 Feb 8253(2014). 10.7860/JCDR/2014/6510.400624701481 PMC 3972597 · doi ↗ · pubmed ↗
- 8Fu H Lin H H Hallett T B Arinaminpathy N Explaining age disparities in tuberculosis burden in Taiwan: a modelling study BMC Infectious Diseases 2020 Dec 20112(2020). 10.1186/s 12879-020-4914-2PMC 705767332131756 · doi ↗ · pubmed ↗