Acquired Haemophilia A Associated With Suspected Chronic Neutrophilic Leukaemia Presenting As Fatal Retroperitoneal Haemorrhage in an Elderly Patient
Fahad Ul Islam Mir, Usama Ali Nizam, Azhar H Baba, Sumiya Arshad, Saalis Maqbool, Mehreen Mir

TL;DR
An elderly patient with a rare bleeding disorder and suspected blood cancer experienced fatal internal bleeding, highlighting the challenges of diagnosing and treating such conditions.
Contribution
This case report links acquired haemophilia A with suspected chronic neutrophilic leukaemia and fatal retroperitoneal haemorrhage in an elderly patient.
Findings
The patient had a severe factor VIII deficiency and high-titer inhibitors, consistent with acquired haemophilia A.
Persistent neutrophilia over years suggested undiagnosed chronic neutrophilic leukaemia.
The patient's condition led to retroperitoneal haemorrhage and a fatal outcome despite interventions.
Abstract
Acquired haemophilia A (AHA) is a rare but potentially life-threatening bleeding disorder caused by autoantibodies against coagulation factor VIII. It often presents with spontaneous bleeding and prolonged activated partial thromboplastin time (aPTT) and is commonly associated with autoimmune disorders, malignancy, or idiopathic causes. Chronic neutrophilic leukaemia (CNL) is a rare myeloproliferative neoplasm that has occasionally been linked with paraneoplastic phenomena, including AHA. An elderly patient presented following a fall with normal imaging but was noted to have a markedly prolonged aPTT (78-104 seconds), normal prothrombin time (PT), and an isolated severe factor VIII deficiency (<0.01 IU/mL). A Bethesda assay confirmed high-titer factor VIII inhibitors, with a measured level of 9 Bethesda units (BU). No underlying autoimmune disease or malignancy was identified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
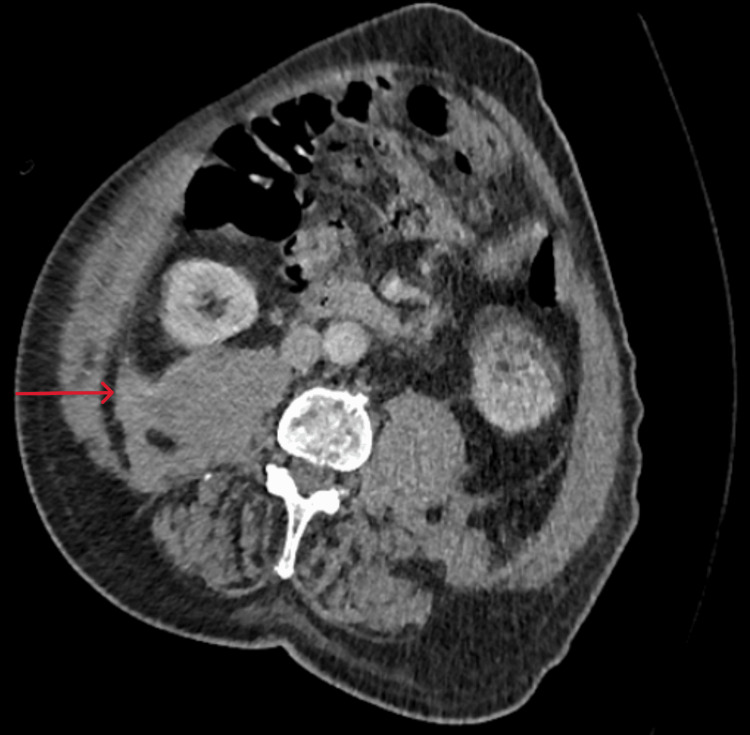 Figure 1
Figure 1| Blood test | Result | Reference range |
| White cell count | 13.4 | 4-11 x 109/L |
| Haemoglobin | 88 | 130-170 g/L |
| MCV | 94 | 83-100 fL |
| Platelet count | 239 | 150-400 x 109/L |
| Neutrophil count | 10.78 | 1.5-8.0 x 109/L |
| CRP | 2 | <5 mg/L |
| aPTT | 78 | 25.1-36.5 seconds |
| PT | 11.7 | 10-13.2 seconds |
| INR | 1.0 | 0.9-1.3 |
| Fibrinogen | 3.6 | 2-4 g/L |
| Creatinine | 144 | 59-104 umol/L |
| Urea | 16.6 | 2.5-7.8 mmol/L |
| Bilirubin | 10 | <21 umol/L |
| ALT | 16 | 10-60 U/L |
| Blood test | Results | Reference range |
| White cell count | 14.6 | 4-11 x 109/L |
| Haemoglobin | 57 | 130-170 g/L |
| Platelet count | 308 | 150-400 x 109/L |
| Neutrophil count | 12.64 | 1.5-8 x 109/L |
| Activated partial thromboplastin time (aPTT) | 104 | 25.1-36.5 seconds |
| Prothrombin time (PT) | 12.8 | 10-13.2 seconds |
| INR | 1.1 | 1.0-1.3 |
| Fibrinogen | >6 | 2-4 g/L |
| CRP | 46 | <5 mg/L |
| ANA | Weakly positive | - |
| Hep2 ANA | Negative | - |
| ENA | Negative | - |
| Anti-dsDNA | 23.7 | <27 IU/mL |
| Rheumatoid factor | 13.3 | <20 IU/mL |
| Serum kappa: lambda ratio | 1.14 | 0.26-1.25 |
| Factor VIII assay | 0.01 | 0.50-2.00 IU/mL |
| Factor XI assay | 0.74 | 0.7-2.00 IU/mL |
| Factor XII assay | 0.50 | 0.5-2.00 IU/mL |
| Factor IX assay | 0.73 | 0.5-2.00 IU/mL |
| von Willebrand activity | 3.19 | 0.4-1.63 IU/mL |
| Immunoglobulin G | 11.66 | 6-16 g/L |
| Immunoglobulin M | 0.50 | 0.4-2.3 g/L |
| Immunoglobulin A | 2.97 | 0.7-4.0 g/L |
| Mixing studies 50:50 | 73.3 seconds | - |
| Bethesda assay | 9 Bethesda units | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHemophilia Treatment and Research · Chronic Myeloid Leukemia Treatments · Coagulation, Bradykinin, Polyphosphates, and Angioedema
Introduction
Acquired haemophilia A (AHA) is a very uncommon autoimmune bleeding disorder resulting from the development of neutralizing antibodies (inhibitors) against coagulation factor VIII. The incidence is approximately 1-1.5 cases per million per year, predominantly affecting the elderly, and carries high morbidity and mortality due to severe bleeding events [1,2]. Clinical presentation may include spontaneous bleeding, soft tissue hematomas, and mucosal or retroperitoneal haemorrhages, often without prior bleeding history.
Risk factors for AHA include autoimmune conditions, malignancies, dermatological diseases, pregnancy, and medications, though up to 50% of cases are idiopathic [3]. Laboratory findings typically show an isolated prolongation of activated partial thromboplastin time (aPTT) not corrected by mixing studies, with reduced factor VIII levels and a positive Bethesda inhibitor assay.
Chronic neutrophilic leukaemia (CNL) is a rare myeloproliferative neoplasm characterized by sustained mature neutrophilia and splenomegaly. Its association with paraneoplastic syndromes, including acquired haemophilia, has rarely been reported [4]. This case underscores a possible link between undiagnosed CNL and AHA, with fatal bleeding complications.
Case presentation
An elderly patient was admitted following a fall. CT trauma series including CT head was all negative. Initial blood investigations (Table 1) revealed leukocytosis, with a white cell count (WCC) of 13.4 ×10^9^/L, absolute neutrophil count (ANC) of 11.0 ×10^9^/L, a prolonged aPTT of 78 seconds (reference: 28-40 seconds), a normal prothrombin time (PT), and a normal C-reactive protein (CRP). A review of history, medications, and prior coagulation profiles (normal PT and aPTT in August 2024) revealed no obvious aetiology. A repeat aPTT was 83 seconds.
On day 1 of admission, the patient developed a spontaneous right arm bruise. Later that day, the patient became hypotensive and reported bilateral flank pain, along with a new right flank cutaneous hematoma. Haemoglobin dropped acutely from 88 g/L to 57 g/L, prompting a major haemorrhage call. Two units of packed red blood cells were transfused. CT abdomen/pelvis revealed a retroperitoneal haemorrhage with psoas muscle hematoma, without active extravasation (Figure 1). CT abdomen additionally showed hepatosplenomegaly, which was noted on previous scans as well. His BP and hemodynamic status improved. Sometime later, the patient reported central chest discomfort and was visibly sweaty. ECG was performed, which showed transient ST-elevation in inferior leads. Cardiology advice was sought who advised against treatment for chest pain and ECG changes and suggested to treat bleeding tendency. Interestingly, his chest pain improved after some time, along with the resolution of ST-segment changes. The case was discussed with the haematology team regarding suspicion of acquired haemophilia, who suggested repeating the coagulation screen and sending for a haemophilia screen (Table 2). WCC was raised, and the ANC was 12.64, representing approximately 88% of the total cells. Blood film showed neutrophilia, and there were no blast cells were seen. The repeat aPTT was 104 seconds. Mixing studies showed partial correction (to 73.3 sec), and the Bethesda assay confirmed FVIII inhibitors (9 Bethesda Units). The autoimmune screen was negative apart from weakly positive antinuclear antibody (ANA), with negative extractable nuclear antigen (ENA) and Hep2 ANA. Myeloma screen and lupus anticoagulant were negative. Factor assays showed factor VIII <0.01 IU/mL (reference: 0.5-1.5 IU/mL), with normal levels of factors IX, XI, and XII, and von Willebrand factor (vWF) activity was elevated (3.19 IU/mL; reference: 0.40-1.63).
CT abdomen showing high-density fluid along the right psoas muscle, suggestive of hematoma (red arrow).
Historical full blood counts revealed persistent neutrophilia over a three-year period, with the most recent results in August 2024 showing a WCC of 14 ×10^9^/L and an ANC of 11.2 ×10^9^/L, raising suspicion of previously undiagnosed CNL. No lesions were seen on CT to suggest solid malignancy. Treatment was complicated by the fact that he was already bleeding, plus he had an ischemic cardiac event, and after a multidisciplinary discussion, he was switched to palliative care. The patient sadly passed away eight days post-admission.
Discussion
This case illustrates a classic presentation of AHA with spontaneous bleeding and isolated prolonged aPTT in an elderly patient, with no prior history of bleeding disorders. The diagnosis was supported by low FVIII levels, incomplete correction on mixing studies, and positive Bethesda assay.
The absence of a clear autoimmune or solid tumour aetiology led to a haematological review, with longstanding neutrophilia raising the suspicion of CNL, a rare myeloproliferative neoplasm. Although not confirmed by bone marrow biopsy due to the rapid clinical deterioration, this represents a likely paraneoplastic-acquired haemophilia. AHA can present as life-threatening bleeds including retroperitoneal haemorrhage, as seen in this case, often requiring urgent immunosuppressive therapy, bypassing agents, and specialist care [5,6]. Unfortunately, rapid progression and cardiac complications limited definitive intervention in this patient.
Early recognition and prompt initiation of factor VIII inhibitor bypassing therapy (e.g., recombinant activated factor VII (rFVIIa), activated prothrombin complex concentrate (FEIBA)) and immunosuppressive treatment (e.g., corticosteroids, cyclophosphamide, rituximab) are critical in reducing mortality in AHA [3,6].
Conclusions
This case highlights the diagnostic complexity and clinical severity of AHA, particularly when associated with a potential underlying myeloproliferative disorder such as CNL. The patient’s presentation with spontaneous bleeding, markedly prolonged aPTT, and severe factor VIII deficiency in the absence of prior coagulopathy emphasizes the importance of considering acquired haemophilia in the differential diagnosis of unexplained bleeding. Early recognition of this rare condition, with prompt initiation of appropriate treatment with immunosuppressive therapy and haemostatic agents, is essential to improving outcomes. Unfortunately, the delayed diagnosis in this case, compounded by retroperitoneal haemorrhage and subsequent cardiovascular complications, underscores the high mortality risk associated with AHA and the need for heightened clinical awareness, particularly in elderly patients with unexplained bleeding and abnormal coagulation profiles.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acquired hemophilia A in the United Kingdom: a 2-year national surveillance study by the United Kingdom Haemophilia Centre Doctors' Organisation Blood Collins PW Hirsch S Baglin TP 1870187710920071704714810.1182/blood-2006-06-029850 · doi ↗ · pubmed ↗
- 2Demographic and clinical data in acquired hemophilia A: results from the European Acquired Haemophilia Registry (EACH 2)J Thromb Haemost Knoebl P Marco P Baudo F 6226311020122232190410.1111/j.1538-7836.2012.04654.x · doi ↗ · pubmed ↗
- 3Acquired factor VIII inhibitors in oncohematology: a systematic review Crit Rev Oncol Hematol Franchini M Targher G Manzato F Lippi G 1941996620081824372710.1016/j.critrevonc.2007.12.004 · doi ↗ · pubmed ↗
- 4Chronic neutrophilic leukemia: 2020 update on diagnosis, molecular genetics, prognosis, and management Am J Hematol Szuber N Elliott M Tefferi A 2122249520203176907010.1002/ajh.25688 · doi ↗ · pubmed ↗
- 5International recommendations on the diagnosis and treatment of acquired hemophilia A Haematologica Tiede A Collins P Knoebl P 1791180110520203238157410.3324/haematol.2019.230771 PMC 7327664 · doi ↗ · pubmed ↗
- 6Efficacy and safety of OBI-1, an antihaemophilic factor VIII (recombinant), porcine sequence, in subjects with acquired haemophilia A Haemophilia Kruse-Jarres R St-Louis J Greist A 1621702120152562316610.1111/hae.12627 · doi ↗ · pubmed ↗