Unraveling Acute Kidney Injury: An Intricate Case of Sepsis and Immune-Mediated Renal Damage
Maha Hassan, Melissa Perez, Michael Girdler, Amarbir Dhillon, Prashant Karkal

TL;DR
This case study explores a complex instance of acute kidney injury involving sepsis and immune-mediated damage, highlighting the need for a broad diagnostic approach.
Contribution
The case presents a rare combination of sepsis, antibiotic nephrotoxicity, and ANCA-negative pauci-immune glomerulonephritis in AKI.
Findings
A 68-year-old patient with pneumonia and sepsis developed rapid-onset AKI linked to immune-mediated processes.
Renal biopsy showed acute tubular injury without immune complex deposition and elevated myeloperoxidase.
Treatment with rituximab and corticosteroids improved renal function, supporting an immune-mediated etiology.
Abstract
Acute kidney injury (AKI) is a critical condition characterized by a sudden decline in kidney function, often posing diagnostic and therapeutic challenges due to its multifactorial nature. This case is significant, as it exemplifies the complexity of AKI in the context of coexisting sepsis, potential antibiotic nephrotoxicity, and immune-mediated processes. While AKI related to sepsis and renal toxic antibiotics is well-documented, the rapid onset and the involvement of antineutrophil cytoplasmic antibody (ANCA)-negative pauci-immune glomerulonephritis add a unique dimension to this case, contributing novel insights to the medical literature. ANCA-negative pauci-immune glomerulonephritis is characterized by a rapidly progressive glomerulonephritis that lacks the detection of antineutrophil cytoplasmic antibodies. We report the case of a 68-year-old Hispanic male with a history of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
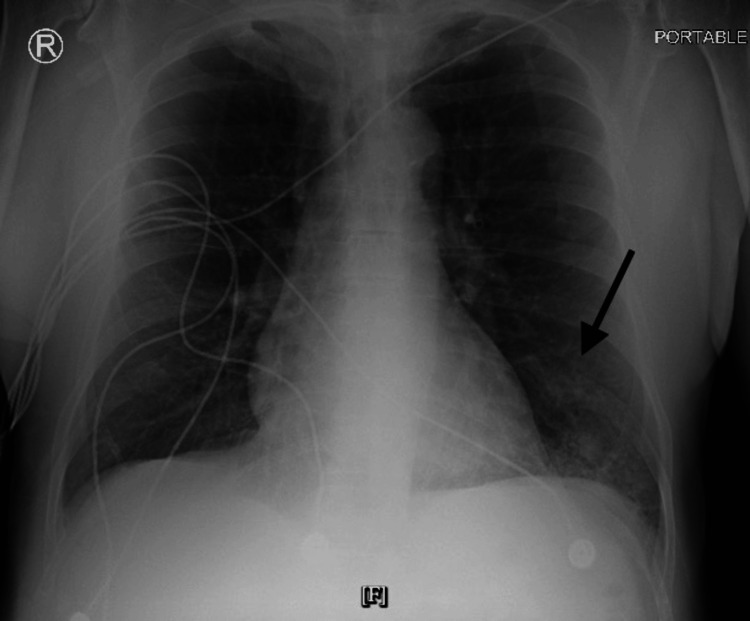 Figure 1
Figure 1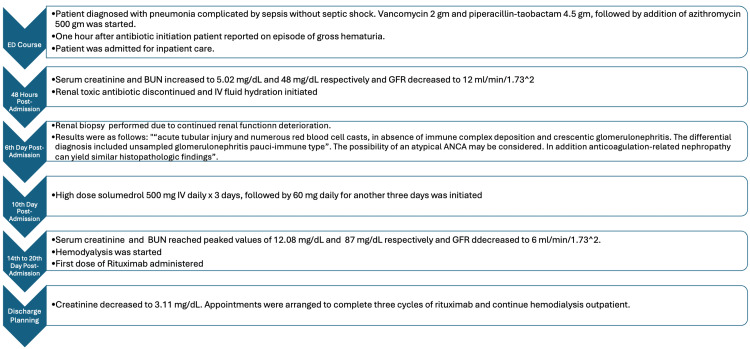 Figure 2
Figure 2| ED laboratories | ||
| Comprehensive metabolic panel | Reference | Patient’s results |
| Sodium | 137-145 mmol/L | 134 |
| Potassium | 3.5-5.1 mmol/L | 4.5 |
| Chloride | 98-107 mmol/L | 109 |
| Glucose | 74-106 mg/dL | 128 |
| Blood urea nitrogen | 9-20 mg/dL | 23 |
| Creatine | 0.66-1.25 mg/dL | 1.38 |
| Estimated glomerular filtration rate | >60 mL/min/1.73 m2 | 51 |
| Alanine aminotransferase | 0-35 U/L | 29 |
| Aspartate aminotransferase | 15-46 U/L | 84 |
| Total bilirubin | 0.2-1.3 mg/dL | 6.8 |
| Direct bilirubin | 0.0-0.3 mg/dL | 3.1 |
| Lactic acid | 0.7-2.0 mmol/L | 3.0 |
| Complete blood count | ||
| White blood count | 3.4-11 10*3/uL | 31.8 |
| Hemoglobin | 13-17.2 g/dL | 10.7 |
| Platelets | 130-360 10*3/uL | 426 |
| Neutrophil | 40%-70% | 88% |
| COVID-19 | Non-reactive | Non-reactive |
| Mycoplasma | Non-reactive | Non-reactive |
| Influenza A/B | Non-reactive | Non-reactive |
| Legionella | Non-reactive | Non-reactive |
| Reference | Day 2 | Day 7 | Day 14* | Day 26 | |
| Creatinine | 0.66-1.25 mg/dL | 5.02 | 10.96 | 12.08 | 3.11 |
| GFR | >60 mL/min/1.73 m2 | 12 | 5 | 6 | 20 |
| BUN | 9-20 mg/dL | 48 | 77 | 87 | 58 |
| Autoimmune panel | Reference | Patient's results |
| C3 | 82-167 mg/dL | 120 |
| C4 | 12-38 mg/dL | 31 |
| p-ANCA | Neg: 1:20 | <1:20 |
| c-ANCA | Neg: 1:20 | <1:20 |
| MPO | 0-469 pmol/L | 673 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Muscle and Compartmental Disorders · Chronic Kidney Disease and Diabetes
Introduction
Acute kidney injury (AKI) is characterized by a rapid decline in renal function, clinically demonstrated by a rapid increase in serum creatinine levels and/or sharp reduction in urine output. In non-hospitalized patients, the most prevalent cause of AKI is decreased renal perfusion, whereas in hospitalized patients, the leading cause of AKI is acute tubular necrosis [1]. On the other hand, AKI may result from sepsis and systemic inflammatory conditions, driven by various factors, including the kidneys’ critical role in clearing and filtering circulating cytokines and bacterial toxins [2].
In this case report, we present a 68-year-old male with a complex medical history, including asthma, pulmonary emphysema, a three-month history of non-productive cough, and a 50-year pack smoking history who presented to the ED with new onset shortness of breath (SOB), chills, nausea, vomiting, a single episode of diarrhea, and a five-day history of productive cough. During the ED evaluation, the patient experienced an episode of gross hematuria with rapid clot formation, which precluded urine analysis evaluation. Subsequently, beginning on the second day of hospitalization, the patient’s serum creatinine level began to rise from a baseline of 1.38 mg/dL to 5.02 mg/dL on the third day of admission, eventually peaking at 12.08 mg/dL on the fourteenth day after admission. This case underscores the diagnostic complexity of AKI in the context of multifactorial etiologies and highlights the importance of a comprehensive and systematic approach to its evaluation and management.
Case presentation
A 68-year-old Hispanic male with a past medical history of asthma, pulmonary emphysema, a three-month history of non-productive cough, and a 50-year pack smoking history presented to the ED due to new onset SOB, chills, nausea, vomiting, diarrhea, and a five-day history of productive cough. Two days before presenting to the ED, he was evaluated by his primary care provider, who prescribed him amoxicillin 500 mg every 8 hours, benzonatate 100 mg every 8 hours, and albuterol sulfate 90 mcg inhaler, two puffs every 6 hours. He had taken three doses of amoxicillin without improvement of the symptoms at the time of evaluation in the ER.
Upon arrival, the patient presented with a blood pressure of 169/86 mmHg, a temperature of 99.2°F, a respiratory rate of 24 bpm, a heart rate of 117 bpm, and an oxygen saturation of 92%. On physical examination, he exhibited mild crackles in the right lower lobe on respiratory examination, and there were no signs of periorbital edema or pitting edema. He appeared well-developed and well-nourished and was alert and oriented to person, place, and time. Laboratory findings revealed leukocytosis with left shift (WBC: 31.8×10⁹/L and neutrophils: 88%), lactic acid: 3 mmol/L, hemoglobin: 10.7 g/dL, creatinine: 1.38 mg/dL, and potassium: 4.5 mmol/L. Additionally, infectious workup for Mycoplasma, Legionella, influenza A and B, and COVID-19 were all negative (Table 1).
Radiologic imaging included a chest X-ray, which revealed patchy opacities in the left lung base, consistent with pneumonia (Figure 1). Based on the clinical, laboratory, and radiologic findings, the patient was diagnosed with pneumonia complicated by sepsis without septic shock; after blood and sputum cultures were obtained, antibiotic therapy was initiated with vancomycin 1 gm and piperacillin-tazobactam 4.5 gm, followed by the addition of azithromycin 500 mg. Approximately one hour after the initiation of the antibiotics, he reported an episode of gross hematuria with rapid coagulation, which precluded the performance of a urine analysis. The patient was admitted to the hospital for inpatient management and evaluation. The patient's CURB-65 score was 2, corresponding to moderate risk.
ED chest X-ray
Forty-eight hours after admission, the patient’s creatinine, blood urea nitrogen (BUN), and glomerular filtration rate (GFR) levels sharply differed from a baseline of 1.38 mg/dL, 23 mg/dL, 51 mL/min/1.73 m^2^ to 5.02 mg/dL, 48 mg/dL, and 12 mL/min/1.73 m^2^, respectively (Table 2).
Due to the patient’s deterioration of renal function, nephrology was consulted who initiated a work-up that included levels of complement component three, complement component four, perinuclear ANCA, ANCA, cytoplasmic ANCA, myeloperoxidase (MPO), the workup was remarkable for MPO at 673 pmol/L as seen in Table 3.
Additionally, a renal ultrasound demonstrated an unremarkable gross appearance of the kidneys.
Despite supportive measures such as discontinuation of renal toxic antibiotics and intravenous fluid administration, his renal function continued to deteriorate with creatinine, BUN, and estimated GFR levels reaching a peak of 12.08 mg/dL, 87 mg/dL, and 6 mL/min/1.73 m^2^ on the fourteenth day of hospitalization (Table 2). On the fourth day after admission, a tunneled dialysis catheter was placed in the right internal jugular vein, and hemodialysis was started.
A renal biopsy was performed on the sixth day after admission. The pathology results were consistent with the following: “acute tubular injury and numerous red blood cell casts, in the absence of immune complex deposition and crescentic glomerulonephritis. The differential diagnosis included unsampled glomerulonephritis pauci-immune type”. The possibility of an atypical ANCA may be considered. Additionally, anticoagulation-related nephropathy can yield similar histopathological findings.
Therefore, given that an underlying immune-mediated renal injury was considered as a possible culprit of AKI, high-dose solumedrol 500 mg IV daily for three days, followed by prednisone 60 mg daily for another three days, was initiated on the tenth day of admission. Subsequently, rituximab was added to the patient's treatment plan.
After initiation of hemodialysis, steroids, and the first dose of rituximab, the patient’s renal function began to improve, and he was discharged with a creatinine level of 3.11 mg/dL, as seen in Table 2. The patient was instructed to continue care in the outpatient setting to complete three cycles of rituximab and hemodialysis. Figure 2 provides an overview of the patient's clinical course.
Overview of the patient's clinical course
Discussion
This case exemplifies the multifactorial nature of AKI in patients with complex comorbidities, with sepsis being a primary contributor but without neglecting renal toxic antibiotics and pauci-immune-mediated glomerulonephritis as important contributors to the pathophysiology.
An important consideration for the cause of AKI is the use of renal toxic antibiotics. However, while the combination of vancomycin and piperacillin-tazobactam carries a high risk of AKI, the typical onset of AKI typically occurs eight days after the initiation of therapy [3]. Therefore, the rapid onset of hematuria within one hour after treatment initiation and the increase of creatinine and BUN just 48 hours after treatment initiation make renal toxic antibiotics a less likely culprit of the patient’s presentation.
In this case, while sepsis is considered a potential cause of the patient's presentation, the most likely underlying issue appears to be ANCA-negative pauci-immune glomerulonephritis. Sepsis-related AKI involves complex pathophysiology that is not entirely understood, though it is believed that the inflammatory response plays a crucial role. Histopathological findings in sepsis-mediated AKI often show patchy and heterogeneous tubular cell injury with apical vacuolization but without tubular necrosis, as was observed in our patient [4]. A significant factor in organ dysfunction in sepsis is the widespread activation of neutrophils, which is frequently associated with elevated MPO levels, leading to oxidative stress and tissue damage [5].
However, the rapid and severe deterioration of the patient's renal function, along with the clinical presentation, suggested the possibility of an ANCA-negative pauci-immune glomerulonephritis affecting the unsampled renal parenchyma. Due to the fulminant and rapidly progressive nature of the renal impairment, aggressive immunosuppressive treatment with rituximab was initiated. Following this treatment, the patient's renal function showed significant improvement, supporting the hypothesis that an underlying immune-mediated and systemic inflammatory response was the most likely cause of the patient's condition.
Conclusions
In conclusion, this case underscores the multifactorial nature of AKI in patients with complex comorbidities, highlighting the challenges in identifying the primary contributors to renal dysfunction. While sepsis emerged as a primary factor due to its association with systemic inflammation and rapid renal deterioration, the potential role of renal toxic antibiotics and ANCA-negative pauci-immune glomerulonephritis could not be overlooked. This case highlights the importance of considering multiple potential etiologies in the differential diagnosis of AKI, especially in the presence of complex clinical presentations. It also emphasizes the need for a comprehensive approach that integrates clinical, laboratory, and histopathological data to guide effective treatment strategies and improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute kidney injury: medical causes and pathogenesis J Clin Med Turgut F Awad AS Abdel-Rahman EM 3751220233661517510.3390/jcm 12010375 PMC 9821234 · doi ↗ · pubmed ↗
- 2Immunopathogenesis of acute kidney injury Toxicol Pathol Radi ZA 9309434620183028252410.1177/0192623318799976 · doi ↗ · pubmed ↗
- 3Acute kidney injury in patients treated with vancomycin and piperacillin-tazobactam: a retrospective cohort analysis J Hosp Med Rutter WC Burgess DR Talbert JC Burgess DS 77821220172818280110.12788/jhm.2684 PMC 5573255 · doi ↗ · pubmed ↗
- 4A unified theory of sepsis-induced acute kidney injury: inflammation, microcirculatory dysfunction, bioenergetics, and the tubular cell adaptation to injury Shock Gomez H Ince C De Backer D Pickkers P Payen D Hotchkiss J Kellum JA 31141201410.1097/SHK.0000000000000052 PMC 391894224346647 · doi ↗ · pubmed ↗
- 5Circulating myeloperoxidase is elevated in septic shock and is associated with systemic organ failure and mortality in critically ill patients Free Radic Biol Med Carr AC Spencer E Hoskin TS Rosengrave P Kettle AJ Shaw G 46246815220203169808110.1016/j.freeradbiomed.2019.11.004 · doi ↗ · pubmed ↗