Evaluating the Effect of Total Hip Arthroplasty on Bone Mineral Density in Postmenopausal Women Using an Artificial Intelligence-Assisted Osteoporosis Diagnostic System
Hisatoshi Ishikura, Toru Moro, Takeyuki Tanaka, Naoto Kaminaga, Kenichi Kato, Mayu Iiboshi, Sakae Tanaka

TL;DR
This study finds that total hip arthroplasty may slow bone density loss in postmenopausal women with hip osteoarthritis.
Contribution
A novel AI-assisted diagnostic system estimates BMD changes in postmenopausal women after hip surgery.
Findings
THA slowed annual BMD decline in lumbar spine and proximal femur compared to age-matched population trends.
BMD decline rates were lower in patients who had THA at younger ages.
AI-assisted system using chest radiographs effectively estimated BMD changes.
Abstract
Background and aim: Total hip arthroplasty (THA) alleviates pain and improves walking ability and quality of life in patients with hip osteoarthritis (OA). However, its effect on systemic bone mineral density (BMD) remains unclear. In this study, we investigated the effect of THA on systemic BMD in postmenopausal women with hip OA using an artificial intelligence (AI)-assisted osteoporosis diagnostic support system that estimates BMD solely using posteroanterior chest radiographs. Methods: This retrospective observational study included postmenopausal Japanese women aged 50-59 years who underwent bilateral THA on separate occasions at our institution between 2007 and 2023. BMD was estimated using our AI-assisted osteoporosis diagnostic system that uses posteroanterior chest radiographs obtained approximately one month before each THA. The rate of change was compared with age-specific…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
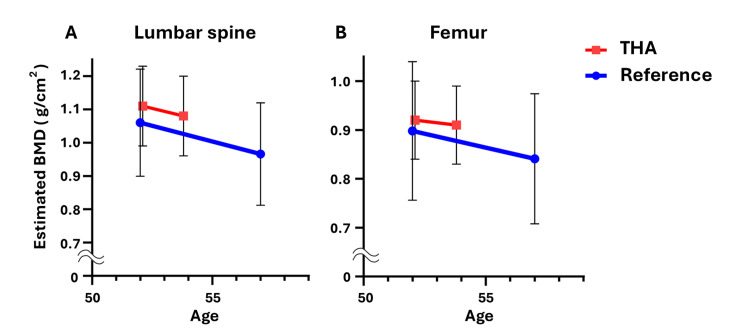 Figure 1
Figure 1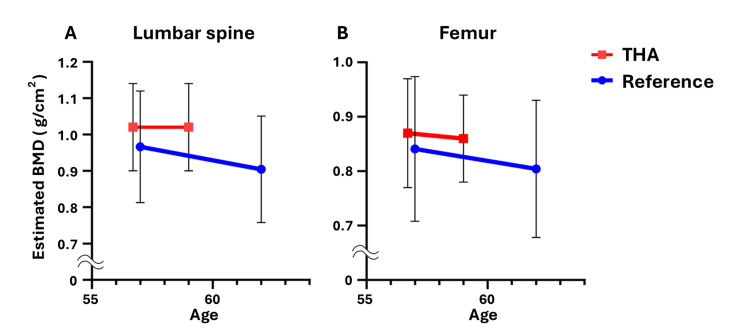 Figure 2
Figure 2| Variable | 50-54 years age group | 55-59 years age group | P-value |
| Number of patients | 23 | 36 | |
| Age at the first THA (years) | 52.1±1.3 | 56.7±1.5 | <0.001 |
| Height (m) | 1.56±0.08 | 1.57±0.09 | 0.602 |
| Weight (kg) | 57.7±12.2 | 57.0±11.8 | 0.145 |
| Body mass index (kg/m2) | 23.3±3.9 | 23.5±3.8 | 0.387 |
| Interval between THAs (years) | 1.7±1.1 | 2.3±2.3 | 0.2 |
| Pre-THA | |||
| Estimated BMD in lumbar (g/cm2) | 1.11±0.12 | 1.02±0.12 | 0.01 |
| Estimated BMD in femur (g/cm2) | 0.92±0.08 | 0.87±0.10 | 0.04 |
| Post-THA | |||
| Estimated BMD in lumbar (g/cm2) | 1.08±0.12 | 1.02±0.12 | 0.08 |
| Estimated BMD in femur (g/cm2) | 0.91±0.08 | 0.86±0.10 | 0.01 |
| Age (years) | THA interval (days) | Estimated BMD in lumbar spine | Estimated BMD in femur | ||||||
| Before THA | After THA | Before THA | After THA | ||||||
| BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | ||
| 50 | 216 | 1.13 | 99 | 1.05 | 91 | 0.91 | 95 | 0.91 | 95 |
| 50 | 762 | 0.99 | 86 | 0.95 | 82 | 0.84 | 88 | 0.87 | 90 |
| 51 | 291 | 1.10 | 95 | 1.08 | 94 | 0.94 | 97 | 0.97 | 101 |
| 51 | 327 | 1.18 | 102 | 1.05 | 91 | 0.84 | 87 | 0.83 | 86 |
| 51 | 974 | 1.11 | 96 | 1.07 | 93 | 0.96 | 100 | 0.91 | 95 |
| 51 | 301 | 1.11 | 96 | 1.11 | 96 | 0.92 | 96 | 0.88 | 92 |
| 51 | 654 | 1.18 | 102 | 1.26 | 109 | 0.99 | 103 | 0.99 | 103 |
| 51 | 435 | 1.15 | 100 | 1.07 | 93 | 0.93 | 96 | 0.87 | 91 |
| 52 | 923 | 1.08 | 94 | 1.01 | 87 | 0.85 | 89 | 0.87 | 91 |
| 52 | 847 | 0.96 | 83 | 0.93 | 81 | 0.90 | 94 | 0.82 | 85 |
| 52 | 287 | 1.29 | 112 | 1.26 | 109 | 0.98 | 102 | 0.96 | 100 |
| 52 | 1638 | 1.10 | 96 | 1.07 | 93 | 0.99 | 104 | 0.95 | 99 |
| 52 | 840 | 1.24 | 108 | 1.09 | 95 | 0.91 | 95 | 0.87 | 90 |
| 52 | 217 | 0.93 | 81 | 0.99 | 86 | 0.81 | 84 | 0.84 | 87 |
| 52 | 241 | 1.06 | 92 | 0.98 | 85 | 0.90 | 94 | 0.90 | 94 |
| 53 | 420 | 1.05 | 91 | 1.03 | 89 | 0.92 | 96 | 0.91 | 95 |
| 53 | 1,561 | 1.01 | 88 | 1.03 | 90 | 0.88 | 91 | 0.90 | 94 |
| 53 | 441 | 1.19 | 103 | 1.20 | 105 | 0.99 | 103 | 1.01 | 105 |
| 54 | 357 | 1.19 | 104 | 1.20 | 104 | 0.99 | 103 | 0.97 | 101 |
| 54 | 1022 | 0.89 | 78 | 0.86 | 75 | 0.80 | 84 | 0.79 | 82 |
| 54 | 256 | 1.28 | 111 | 1.23 | 107 | 1.02 | 106 | 1.00 | 104 |
| 54 | 623 | 0.93 | 80 | 0.96 | 83 | 0.83 | 86 | 0.83 | 87 |
| 54 | 252 | 1.32 | 114 | 1.37 | 119 | 1.15 | 120 | 1.12 | 117 |
| Age (years) | THA interval (days) | Estimated BMD in lumbar spine | Estimated BMD in femur | ||||||
| Before THA | After THA | Before THA | After THA | ||||||
| BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | BMD (g/cm2) | YAM (%) | ||
| 55 | 280 | 1.15 | 100 | 1.25 | 109 | 1.00 | 104 | 1.00 | 104 |
| 55 | 469 | 0.91 | 79 | 0.92 | 80 | 0.73 | 76 | 0.73 | 76 |
| 55 | 945 | 1.20 | 104 | 1.04 | 90 | 1.10 | 114 | 1.04 | 108 |
| 55 | 397 | 0.91 | 79 | 0.92 | 80 | 0.87 | 90 | 0.84 | 88 |
| 55 | 376 | 0.92 | 80 | 0.96 | 83 | 0.83 | 86 | 0.84 | 88 |
| 55 | 1163 | 1.13 | 98 | 1.15 | 100 | 0.98 | 102 | 0.93 | 97 |
| 55 | 427 | 0.93 | 81 | 1.00 | 87 | 0.72 | 75 | 0.80 | 83 |
| 55 | 217 | 0.96 | 83 | 0.96 | 84 | 0.87 | 90 | 0.86 | 90 |
| 55 | 189 | 1.19 | 104 | 1.22 | 106 | 1.01 | 105 | 0.97 | 101 |
| 55 | 358 | 1.06 | 92 | 1.01 | 88 | 0.93 | 96 | 0.88 | 92 |
| 55 | 410 | 1.24 | 108 | 1.12 | 97 | 0.93 | 96 | 0.88 | 92 |
| 56 | 302 | 0.96 | 83 | 0.93 | 80 | 0.82 | 85 | 0.80 | 83 |
| 56 | 2366 | 1.20 | 104 | 1.23 | 107 | 1.04 | 108 | 0.96 | 100 |
| 56 | 1491 | 0.82 | 71 | 0.74 | 64 | 0.75 | 78 | 0.70 | 72 |
| 56 | 204 | 0.93 | 81 | 1.03 | 89 | 0.85 | 89 | 0.86 | 89 |
| 56 | 2976 | 0.88 | 76 | 0.86 | 75 | 0.82 | 85 | 0.77 | 80 |
| 56 | 329 | 0.94 | 82 | 0.98 | 85 | 0.82 | 85 | 0.82 | 85 |
| 56 | 1701 | 1.03 | 90 | 0.99 | 86 | 0.78 | 81 | 0.77 | 80 |
| 56 | 567 | 0.92 | 80 | 1.08 | 94 | 0.81 | 84 | 0.86 | 90 |
| 56 | 238 | 0.95 | 83 | 1.00 | 87 | 0.87 | 90 | 0.90 | 94 |
| 57 | 2711 | 1.09 | 95 | 1.10 | 95 | 1.00 | 104 | 0.91 | 95 |
| 57 | 280 | 1.00 | 87 | 0.92 | 80 | 0.88 | 92 | 0.83 | 86 |
| 57 | 212 | 0.93 | 81 | 1.03 | 89 | 0.85 | 89 | 0.90 | 94 |
| 58 | 2934 | 0.85 | 74 | 0.80 | 70 | 0.75 | 79 | 0.68 | 71 |
| 58 | 721 | 1.03 | 89 | 1.01 | 88 | 0.85 | 88 | 0.83 | 87 |
| 58 | 299 | 0.98 | 85 | 0.97 | 84 | 0.78 | 81 | 0.78 | 81 |
| 58 | 869 | 1.13 | 98 | 1.17 | 102 | 1.00 | 104 | 0.99 | 103 |
| 58 | 2176 | 0.95 | 82 | 1.01 | 88 | 0.93 | 97 | 0.88 | 92 |
| 58 | 667 | 1.05 | 91 | 1.06 | 92 | 0.85 | 88 | 0.84 | 88 |
| 58 | 259 | 1.22 | 106 | 1.11 | 96 | 0.92 | 95 | 0.85 | 88 |
| 59 | 252 | 1.13 | 98 | 1.20 | 104 | 0.84 | 87 | 0.90 | 94 |
| 59 | 260 | 1.04 | 90 | 1.01 | 88 | 0.87 | 91 | 0.90 | 94 |
| 59 | 728 | 1.19 | 103 | 1.18 | 103 | 0.99 | 103 | 0.92 | 96 |
| 59 | 2095 | 0.84 | 73 | 0.82 | 71 | 0.71 | 74 | 0.71 | 74 |
| 59 | 381 | 1.17 | 101 | 1.02 | 88 | 0.96 | 99 | 0.89 | 93 |
| 59 | 354 | 0.96 | 83 | 0.99 | 86 | 0.77 | 80 | 0.81 | 84 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone health and osteoporosis research · Orthopaedic implants and arthroplasty · Hip disorders and treatments
Introduction
Hip osteoarthritis (OA) is a leading cause of hip pain, gait disturbance, and impairment in activities of daily living [1]. Total hip arthroplasty (THA) is known to alleviate hip pain, improve walking ability, and improve quality of life and cardiopulmonary function [2,3].
An aging society has led to an annual increase in the number of patients with osteoporosis. Fragility fractures, such as vertebral and proximal femur fractures, not only decrease activities of daily living but also affect life expectancy in these patients [4]. Fractures around implants after THA often require large plates or implant replacements, resulting in extensive treatment. In particular, postmenopausal women experience a substantial decrease in bone mineral density (BMD), highlighting the importance of appropriate nutrition, exercise, and osteoporosis treatments during this period [5]. Regarding the postoperative effects of THA, there have been reports of local bone remodeling around the stem [6]; however, there is still no consensus on its effect on systemic BMD. To address these osteoporosis-related issues, an artificial intelligence (AI)-assisted osteoporosis diagnostic system has been developed to estimate BMD in the lumbar spine and proximal femur using posteroanterior chest radiographs [7,8]. This study aimed to verify the effect of THA on BMD in postmenopausal women using this system and preoperative chest radiographs. Our hypothesis is that THA attenuates age-related BMD decline in postmenopausal women.
Materials and methods
Patients data
We conducted a retrospective observational study in postmenopausal Japanese women aged 50-59 years who underwent independent bilateral THA at our institution between 2007 and 2023. Menopause was defined as the absence of menstruation for more than one year, and menopausal status was determined based on self-reported information. The exclusion criteria were as follows: patients with less than six months or more than 10 years between bilateral THA, patients with obvious abnormalities on chest radiographs (e.g., pneumonia) or foreign bodies (e.g., pacemakers), and patients using osteoporosis treatment drugs during the observation period. As a result, a total of 59 patients were included in the study, comprising 23 patients aged 50-54 years and 36 patients aged 55-59 years. The mean age was 54.9 years, and the mean interval between the two unilateral THAs was 2.1 years. The patient demographics are summarized in Table 1. Written informed consent was obtained from all study participants. The study protocol was approved by the institutional review boards of our institution (Ethical Committee approval no.: 11953-7).
AI-assisted osteoporosis diagnostic system
The authors have conducted the research and development of this AI-assisted osteoporosis diagnostic system using cohort data from approximately 50,000 individuals who underwent health check-ups at hospitals and about 20,000 individuals from the general population [8]. This system performs regression analysis within seconds of uploading a single chest or lumbar spine radiograph and provides estimates of BMD, young adult mean percentage, and T-scores for the lumbar spine and proximal femur. Previous studies have reported highly accurate estimation results using this system [7-9]. Specifically, the correlation coefficients (CCs) between the estimated BMD values calculated from anterior chest radiographs and the actual measured values for the lumbar spine and proximal femur were 0.85 and 0.84, respectively, which were higher than those achieved by other methods, such as dual-energy X-ray absorptiometry (DXA) of the forearm (CC: 0.46-0.62), microdensitometry of the metacarpal bone (CC: 0.66), and quantitative ultrasonography of the calcaneus (CC: 0.29-0.55) [10-14].
Image inspection
Using posteroanterior chest radiographs obtained approximately one month before each unilateral THA, we calculated the estimated BMD from the first and second THA preoperative chest radiographs using the AI osteoporosis diagnostic support system. The BMD calculated from the preoperative chest radiographs for the first THA was considered the pre-THA BMD, whereas the BMD calculated from the preoperative chest radiographs for the second THA was considered the BMD after unilateral THA (post-THA). We compared the rate of change with age-specific BMD reference values for the general Japanese population to assess the effect of THA on BMD [5].
Data analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24 (Released 2017; IBM Corp., Armonk, New York, United States). Statistical significance was set at p < 0.05. The student’s t-test was used to compare the differences in the mean values between the two groups.
Results
Before surgery, the mean estimated BMD values for the lumbar spine and proximal femur were 1.06 g/cm^2^ and 0.89 g/cm^2^, respectively. After THA, with an average follow-up of 2.1 years, the mean estimated BMD values were 1.05 g/cm^2^ and 0.88 g/cm^2^ for the lumbar spine and proximal femur, respectively, showing a slight decrease compared with preoperative values.
In this study, patients were divided into two groups: those aged 50-54 years and those aged 55-59 years. Each group was compared with the BMD reference values of the same age group in the general population. Among the 23 patients in the 50- to 54-year age group who underwent primary THA, the estimated BMD decreased by 1.52% (lumbar spine) and 0.81% (femur) annually (Figure 1). Among the 36 patients in the 55-59 age group who underwent primary THA, the estimated BMD decreased by 0.00% (lumbar spine) and 0.80% (femur) annually (Figure 2). These rates were lower than the age-specific annual BMD loss rates reported in the literature, which indicated an annual bone density decrease rate of 1.77% (lumbar spine) and 1.27% (femur) per year for Japanese women aged 50-54 years and 1.28% (lumbar spine) and 0.88% (femur) per year for those aged 55-59 years (Figures 1, 2) [5]. The detailed data for each case are presented in Tables 2-3.
Trend of the estimated BMD in THA patients aged 50-54 years.The trend of mean and standard deviation of the estimated BMD of the lumbar spine (A) and proximal femur (B) in primary THA patients aged 50-54 years (red line), along with the reference values in Japanese women of the same age (blue line).BMD: bone mineral density; THA: total hip arthroplasty
Trend of the estimated BMD in THA patients aged 55-59 years.The trend of mean and standard deviation of the estimated BMD of the lumbar spine (A) and proximal femur (B) in primary THA patients aged 55-59 years (red line), along with the reference values in Japanese women of the same age (blue line).BMD: bone mineral density; THA: total hip arthroplasty
Discussion
Our study highlights the potential for THA to mitigate age-related BMD decline in postmenopausal women. Few studies have investigated the relationship between THA and systemic bone density, potentially because of the inaccuracy of DXA measurements at the same site in patients with hip OA and the impossibility of DXA measurements at the same site in patients with post-THA [15,16]. However, assessing BMD both before and after THA is crucial because poor bone quality negatively affects postoperative outcomes [17]. Monitoring the bone status of patients undergoing THA and prompt intervention for osteoporosis may improve THA outcomes. Meta-analyses have demonstrated the effectiveness of osteoporosis medications in preventing bone loss around implants [18].
The AI-assisted osteoporosis diagnostic system, capable of estimating BMD using chest radiographs commonly obtained during routine health checkups, offers advantages in terms of medical costs and serves as a useful screening tool for osteoporosis. Its key advantage lies in its ability to accurately estimate BMD using past chest radiographs, regardless of the lumbar spine or hip joint condition. Using this system, we were able to track BMD changes in patients over time, from pre- to post-THA.
Factors that may have contributed to the slow decrease in BMD in postmenopausal patients undergoing THA observed in our study include increased physical activity owing to pain relief and rehabilitation during the perioperative period, which may have improved awareness of physical health. Numerous studies have indicated the beneficial effects of exercise on BMD [19].
Our study has several limitations. First, we could not eliminate errors inherent in the AI-assisted osteoporosis diagnostic system. Second, this retrospective study, conducted at a single institution, had variations in the intervals between bilateral THA surgeries and included a limited number of cases. The errors of these AI systems and the small sample size are significant limitations that may affect the robustness of this study. Further research is needed to improve the accuracy of the AI systems themselves and to increase the sample size through multi-center studies. Moreover, although this study stratified patients by age and excluded those who had undergone osteoporosis treatment, it is also a limitation that factors such as activity level, including the patients' exercise habits, and dietary intake were not considered. Future studies that take these patient backgrounds into consideration may have the potential to address this limitation. Additionally, we compared the BMD of THA patients with age-matched reference values from previous reports of the general population, and a power analysis was not conducted. In the future, analyzing and comparing the natural course of BMD in hip OA cases that did not undergo surgery will allow for a study more focused on the effects of THA.
Despite these various limitations, the strength of this study lies in its innovative approach as the first to use an AI-assisted osteoporosis diagnostic system to comprehensively track changes in BMD before and after THA, providing a foundation for future research.
Conclusions
THA has the potential to attenuate age-related BMD decline in postmenopausal women with hip OA. However, this finding should be interpreted with caution, as the effect may be influenced by previously mentioned limitations, and further research is needed to determine its applicability to the broader postmenopausal population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical practice. Osteoarthritis of the hip N Engl J Med Lane NE 1413142135720071791404210.1056/NEJ Mcp 071112 · doi ↗ · pubmed ↗
- 2Health-related quality of life and appropriateness of knee or hip joint replacement Arch Intern Med Quintana JM Escobar A Arostegui I Bilbao A Azkarate J Goenaga JI Arenaza JC 22022616620061643209210.1001/archinte.166.2.220 · doi ↗ · pubmed ↗
- 3Effect of total hip arthroplasty on cardiovascular fitness J Arthroplasty Ries MD Philbin EF Groff GD Sheesley KA Richman JA Lynch F Jr 8490121997902150710.1016/s 0883-5403(97)90052-8 · doi ↗ · pubmed ↗
- 4Report on the Japanese Orthopaedic Association's 3-year project observing hip fractures at fixed-point hospitals J Orthop Sci Sakamoto K Nakamura T Hagino H 1271341120061656838310.1007/s 00776-005-0998-1 · doi ↗ · pubmed ↗
- 5Diagnostic criteria for primary osteoporosis: year 2012 revision J Bone Miner Metab Soen S Fukunaga M Sugimoto T 2472573120132355350010.1007/s 00774-013-0447-8 · doi ↗ · pubmed ↗
- 6Periprosthetic bone remodeling of short cementless femoral stems in primary total hip arthroplasty: a systematic review and meta-analysis of randomized-controlled trials Medicine (Baltimore) Yan SG Li D Yin S Hua X Tang J Schmidutz F 096201710.1097/MD.0000000000008806 PMC 570898329381984 · doi ↗ · pubmed ↗
- 7Basic study on AI osteoporosis diagnostic support system - bone density estimation using X-ray images [Article in Japanese]J Orthop Sci Moro T Saito T Hidaka R 1738932019 https://jglobal.jst.go.jp/detail?JGLOBAL_ID=201902279120159828
- 8AI-assisted diagnostic system for osteoporosis using the X-ray image [Article in Japanese]Jpn J Joint Dis Moro T Saito T Tanaka T 11351144662023 https://jglobal.jst.go.jp/en/detail?JGLOBAL_ID=202402210390610490