Role of Intravenous Azithromycin as Adjunctive Therapy in Children With Acute Encephalitis Syndrome (AES): An Open-Label Randomized Controlled Trial
Priti Yadav, Kundan Mittal, Paramjeet S Gill, Anindya Mittal, Kausalya Raghuraman, Jaya S Kaushik

TL;DR
This study examines whether adding intravenous azithromycin to standard treatment improves outcomes in children with acute encephalitis syndrome.
Contribution
The study provides empirical evidence on the efficacy and safety of azithromycin as adjunctive therapy for acute encephalitis syndrome in children.
Findings
Adding azithromycin did not reduce all-cause mortality in children with AES.
Hospital stay duration and disability rates were similar between groups.
No serious adverse events were observed in either group.
Abstract
Background: Acute encephalitis syndrome (AES) has high morbidity and mortality in children. Empirical treatment of AES often consists of third-generation cephalosporins, with vancomycin and acyclovir, and frequently excludes the use of azithromycin, targeted at scrub typhus. In a resource-constrained setting, testing for scrub typhus becomes challenging. Considering the lacunae in the existing literature, there is a need for robust evidence to determine the role of additional azithromycin use in children with AES. Objective: To evaluate the efficacy and safety of adjunctive intravenous azithromycin treatment in children with AES compared to standard therapy alone. Material and methods: An open-label, two-arm randomized controlled trial was conducted at a tertiary care teaching hospital with a level III pediatric intensive care unit. Children aged one to 14 years with AES were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
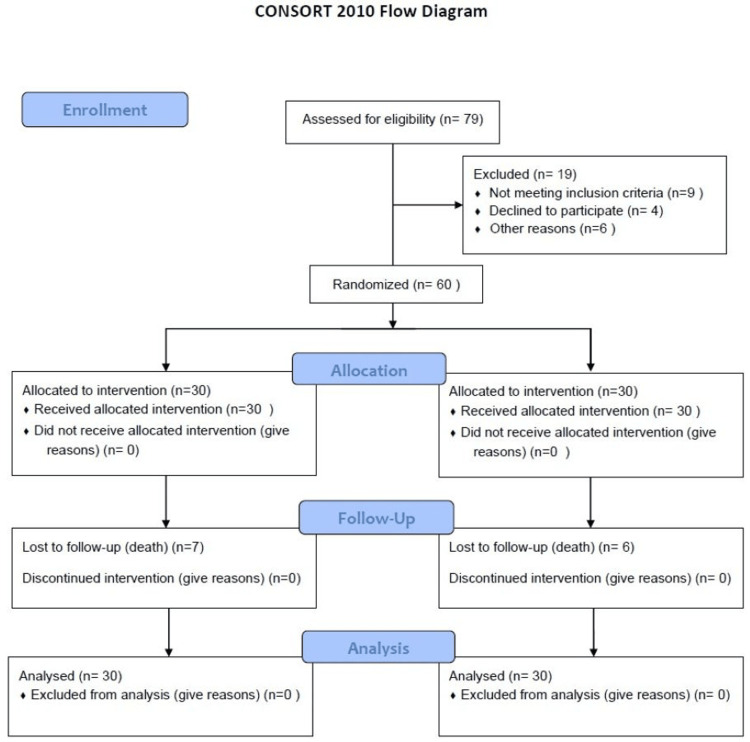 Figure 1
Figure 1| Characteristics | Azithromycin group | Conventional treatment group | P-value |
| Demographics | |||
| Age (mean (SD)) | 7.37 (3.82) | 6.10 (3.84) | 0.18* |
| Male gender (n (%)) | 13 (43.3%) | 17 (56.7%) | 0.31 |
| Rural residence | 16 (53.3%) | 23 (76.7%) | 0.06 |
| Urban residence | 14 (46.7%) | 7 (23.3%) | 0.06 |
| Clinical features | |||
| Fever | 30 (100.0%) | 30 (100.0%) | 1 |
| Abnormal body movements | 30 (100.0%) | 28 (93.3%) | 0.49 |
| Altered sensorium | 30 (100.0%) | 30 (100.0%) | 1 |
| Rash | 0 (0.0%) | 3 (10.0%) | 0.24 |
| Headache | 5 (16.7%) | 6 (20.0%) | 0.74 |
| Nausea/vomiting | 9 (30.0%) | 9 (30.0%) | 1 |
| Arthralgia | 2 (6.7%) | 2 (6.7%) | 1 |
| Myalgia | 1 (3.3%) | 1 (3.3%) | 1 |
| Loose stools | 10 (33.3%) | 7 (23.3%) | 0.39 |
| Examination | |||
| Pallor (yes) | 19 (63.3%) | 18 (60.0%) | 0.79 |
| Hepatomegaly | 5 (16.7%) | 5 (16.7%) | 1 |
| Hepatosplenomegaly | 0 (0.0%) | 1 (3.3%) | 1 |
| Investigations | |||
| ELISA for scrub typhus | 1 (3.3%) | 1 (3.3%) | 1 |
| CSF: protein (mg/dL) | 80.80±36.94 | 106.50±64.85 | 0.08* |
| CSF: sugar (mg/dL) | 70.00±21.20 | 72.20±39.34 | 0.69* |
| CSF: cells (/HPF) | 23.17±46.27 | 27.70±65.39 | 0.36* |
| Outcome measure | Azithromycin group (n=30) | Conventional treatment group (n=30) | P-value |
| All-cause mortality (N (%)) | 7 (23.3%) | 6 (20.0%) | 0.75* |
| Duration of hospital stay in days (mean (SD)) | 12.57 (10.5) | 13.67 (6.8) | 0.28^ |
| Liverpool outcome score at discharge (Mean (SD)) | 52.4 (28.14) | 53.47 (27.78) | 0.79^ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Encephalopathies and Encephalitis · Mosquito-borne diseases and control · SARS-CoV-2 and COVID-19 Research
Introduction
Acute encephalitis syndrome (AES) is an important cause of mortality and morbidity in children in India. The causative agent of AES varies with season and geographical location and predominantly affects the population below 15 years of age. There have been several outbreaks of AES in Uttar Pradesh with an incidence of 15 per million population and a case fatality rate of 12.6% in the years 2015-2019. One Rickettsial infection contributes to 0.5-2% of AES in Uttar Pradesh [1]. Presumptive treatment of febrile illnesses with doxycycline and azithromycin has been associated with a reduction in the progression of febrile illness to AES in the Gorakhpur district of Uttar Pradesh [2]. Although some studies have examined the use of azithromycin in preventing the progression from acute febrile illness to AES, there are no studies evaluating the empirical use of azithromycin for the treatment of AES. Beyond Uttar Pradesh, there are emerging reports of frequent scrub typhus outbreaks in other parts of India, including Rajasthan, Haryana, Meghalaya, and even islands in the Pacific Ocean. In an adult study from Haryana, scrub typhus was detected in 16% of patients admitted with fever lasting more than seven days [3]. AES caused by scrub typhus is treatable with doxycycline and/or azithromycin, which can significantly reduce mortality. The standard management protocol for AES often includes a combination of third-generation cephalosporins, vancomycin, acyclovir, and/or artesunate [4]. However, there is limited literature on the effectiveness of adding azithromycin to the existing treatment regimen for AES. Therefore, this study was planned to evaluate the efficacy and safety of azithromycin in the management of AES in children.
Materials and methods
The study was an open-label, two-arm, randomized controlled trial conducted in the Department of Pediatrics and Microbiology at Pandit Bhagwat Dayal Institute of Medical Sciences, Rohtak, Haryana, a tertiary care referral center in India. The study extended from April 2020 to March 2021. The study was reported in accordance with CONSORT guidelines. Children aged one to 14 years with suspected AES were enrolled in the study. AES was considered in the acute onset of fever with change in the mental status like confusion, disorientation, or coma, and/or new onset of seizure (excluding simple febrile seizure). Recruitment of patients commenced after obtaining ethical approval from the Biomedical Research Ethics Committee (IEC/Th/19/Ped04 dated 30th December 2019). Informed written consent was obtained from the parents of all enrolled subjects, and a patient information sheet was provided to them before enrollment in the study. The study was registered with CTRI (CTRI/2020/05/025270) before the enrollment of the first patient.
All eligible participants were admitted to the pediatric intensive care unit. A detailed clinical history and physical examination were performed in each child. All children were enrolled sequentially and allotted a study number. They were randomized by block randomization using variable block sizes of two, four, and six, generated by computer using random number tables, into two groups: an interventional group (azithromycin (intravenous 10 mg/kg for five days) plus conventional treatment) and a control group (conventional treatment). Azithromycin (500 mg/vial) was used and prepared by diluting 4.8 mL sterile water in a vial to generate a concentration of 100 mg/mL. A sealed opaque envelope containing group codes was prepared. Envelops were sequentially numbered and kept in order according to their serial numbers. The envelope was opened at the time of randomization, and the patient was allocated to their respective group.
Patients were closely monitored for the need for mechanical ventilation, inotropic support, and signs of multi-organ dysfunction. Five milliliters of blood were collected for ELISA testing for scrub typhus, HIV serology, and thick and thin peripheral smears for malaria parasites. Patients were investigated and managed as per the standard treatment protocol. Any adverse event following drug administration was recorded. The primary outcome measure was all-cause mortality. The secondary outcomes include the total duration of hospital stay and the Liverpool outcome score (LOS). The LOS (open access) was performed at the time of discharge, and the mean score was computed to assess the degree of disability [5].
A convenience sample size of 30 participants was chosen for each group, considering logistical limitations. All the measurements and data were analyzed using conventional statistical tools. All data was entered in Microsoft Excel (Microsoft Corporation, Redmond, WA) spreadsheets. Normally distributed variables were described by their mean and standard deviation. For normally distributed data, the Student t-test was employed, and the Mann-Whitney and Chi-square tests were used for categorical data. All data were analyzed using IBM SPSS Statistics (Version 20.0; IBM Corp., Armonk, NY, USA).
Results
Out of 79 eligible participants, 60 children were randomized, 30 to receive azithromycin and 30 to receive conventional treatment (Figure 1).
Study flowFigure showing the enrollment of study subjects.
The baseline demographic characteristics were comparable between the two groups (Table 1). The majority of children presented with fever, abnormal body movement, and altered sensorium in both groups (Table 1).
Only one child in each group tested positive for scrub typhus. On comparison of the primary outcome measure, all-cause mortality was comparable between the azithromycin group (7 (23.3%)) and the conventional treatment group (6 (20%)) (P=0.75). Secondary outcome measures, including duration of hospital stay (12.57 vs. 13.67 days; P=0.28) and LOS (52 vs. 53.4; P=0.79), were also comparable between the two groups (Table 2).
Only one child in the azithromycin group developed a rash and another developed hypotension.
Discussion
Preliminary findings of this study suggest that the addition of azithromycin provided no extra benefit in children with AES in terms of all-cause mortality, duration of hospital stay, or significant disability at discharge. The side effect profile was comparable between the two groups.
Over the past decade, there has been a paradigm shift in the etiology of AES, from Japanese encephalitis (JE) to other infectious and non-infectious causes. Scrub typhus has emerged as a significant cause of AES in North India [6-9]. In a study on 464 children with acute encephalitis, 2.9% of children died, with 6.7% having neurological disability [6]. The case fatality rate varies considerably, and districts of Assam have reported 27.6% mortality among children with AES [10]. In a study from South India, 23% of children with AES had scrub typhus [11]. Authors reported a sensitivity of 93% and a specificity of 82% for IgM when compared to PCR, as used in our study.
In several districts of Uttar Pradesh, the case fatality rate declined to 5-5.8% in 2019-2020, compared to 33% in the early 1980s. Only 0.5-2.0% of cases were attributed to Rickettsial infection. There are several reports of scrub typhus as an emerging cause of AES [12-14].
Authors attribute this sharp decline to aggressive immunization campaigns for JE and presumptive treatment of febrile cases with doxycycline and azithromycin [15-17]. The present study observed a mortality rate of 20-23.3%. The comparable mortality in the present study could be attributed to only two cases that tested positive for scrub typhus on serum testing. In the present study, the additional use of azithromycin did not affect mortality, despite its more extensive coverage, which not only targets Rickettsial infections but also covers Mycoplasma infections. The present study provides evidence on the additional use of azithromycin among children with AES, demonstrating its neutral effect on mortality, duration of hospital stay, and neuro-morbidity.
The present study had certain limitations, including a small sample size, and the interventions were not masked. A facility for testing all neuroviruses in cerebrospinal fluid (CSF) was one of the logistical limitations, and only CSF JE antibodies were tested. There could be many more confounding factors, such as differences in CSF protein, delay in seeking treatment, enrollment during a particular season, or inclusion of a migrating population, which will need to be considered when interpreting the results of the present study. Estimating the entire neuroviral panel would have helped establish the etiology of AES. Moreover, neuroimaging and EEG could not be performed on all enrolled children due to limitations. A lack of long-term follow-up of patients is one of the limitations of the present study. However, authors believe that in the majority of peripheral centers, facilities for neuroimaging, EEG, and long-term follow-up are lacking.
In light of the above limitations, the present study provides some preliminary evidence to discourage routine use of azithromycin among children with AES. However, further studies with a larger sample size and long-term follow-up will be required before limiting the use of azithromycin in the management of AES among children.
Conclusions
In this study with a limited sample size, the addition of azithromycin provided no benefit among children with AES in terms of all-cause mortality, duration of hospital stay, or significant disability at discharge. Only two cases of scrub typhus were identified, for which azithromycin is considered the drug of choice in children. Therefore, we conclude that adjunctive treatment with intravenous azithromycin did not impact all-cause mortality in children with AES in our study. However, a larger sample size and a multicentric study are needed to better understand the effect of azithromycin on all-cause mortality in children with AES.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Case definitions, diagnostic algorithms, and priorities in encephalitis: consensus statement of the International Encephalitis Consortium Clin Infect Dis Venkatesan A Tunkel AR Bloch KC 111411285720132386136110.1093/cid/cit 458PMC 3783060 · doi ↗ · pubmed ↗
- 2Consensus guidelines on evaluation and management of suspected acute viral encephalitis in children in India Indian Pediatr Sharma S Mishra D Aneja S Kumar R Jain A Vashishtha VM 8979104920122325570010.1007/s 13312-012-0216-0 · doi ↗ · pubmed ↗
- 3Changing landscape of acute encephalitis syndrome in India: a systematic review Natl Med J India Joshi R Kalantri SP Reingold A Colford JM Jr 212220252012 https://pubmed.ncbi.nlm.nih.gov/23278779/23278779 · pubmed ↗
- 4Acute encephalitis syndrome in India: the changing scenario Ann Neurosci Ghosh S Basu A 1311332320162772158010.1159/000449177 PMC 5043220 · doi ↗ · pubmed ↗
- 5Disability after encephalitis: development and validation of a new outcome score Bull World Health Organ Lewthwaite P Begum A Ooi MH 5845928820102068012310.2471/BLT.09.071357 PMC 2908971 · doi ↗ · pubmed ↗
- 6Acute encephalitis syndrome in Gorakhpur, Uttar Pradesh, India - role of scrub typhus J Infect Murhekar MV Mittal M Prakash JA 6236267320162759226310.1016/j.jinf.2016.08.014 · doi ↗ · pubmed ↗
- 7Acute encephalitis syndrome in Gorakhpur, Uttar Pradesh, 2016: clinical and laboratory findings Pediatr Infect Dis J Mittal M Bondre V Murhekar M 110111063720182974637810.1097/INF.0000000000002099 · doi ↗ · pubmed ↗
- 8Scrub typhus as a cause of acute encephalitis syndrome, Gorakhpur, Uttar Pradesh, India Emerg Infect Dis Mittal M Thangaraj JW Rose W 141414162320172872661710.3201/eid 2308.170025 PMC 5547812 · doi ↗ · pubmed ↗