Effectiveness of Ecological Momentary Interventions on Pain, Mental Health, and Quality of Life in Individuals With Rheumatic Diseases: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Xiaoxiao Mei, Yan Li, Wing Fai Yeung, Yule Hu, Jiaying Li, Mengqi Li, Janelle Yorke

TL;DR
This study finds that real-time interventions can reduce pain and improve quality of life for people with rheumatic diseases, but do not significantly improve mental health.
Contribution
The first systematic review and meta-analysis examining the effectiveness of ecological momentary interventions in rheumatic disease populations.
Findings
Ecological momentary interventions significantly reduced pain in individuals with rheumatic diseases.
Subgroup analyses showed greater effects with daily reminders and human contact on pain and quality of life.
The interventions did not significantly improve anxiety or depression in participants.
Abstract
Background: Rheumatic diseases are a group of inflammatory conditions that significantly impact physical and mental health. Ecological momentary interventions have shown promising effects among individuals with rheumatic diseases as they can deliver the most appropriate type and intensity of intervention tailored to their needs in real time, but their effectiveness has not been systematically reviewed and examined. Objective: To examine the effectiveness of ecological momentary interventions in reducing pain, improving mental health, and enhancing quality of life in individuals with rheumatic diseases. Design: Systematic review and meta-analysis. Methods: A literature search was conducted in nine electronic databases from inception to April 2024. Randomized controlled trials (RCTs) examining the impact of ecological momentary interventions on pain, mental health, and/or quality of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
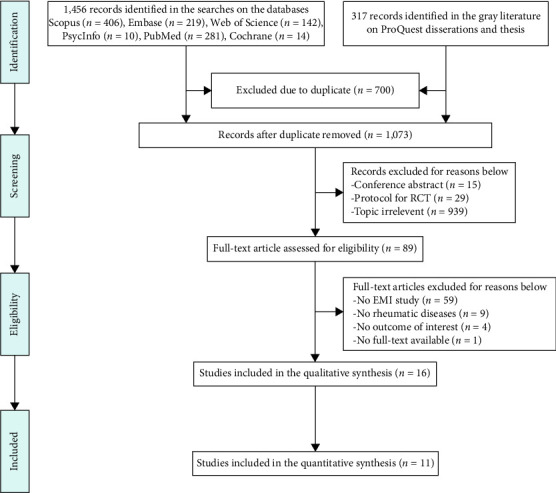 Figure 1
Figure 1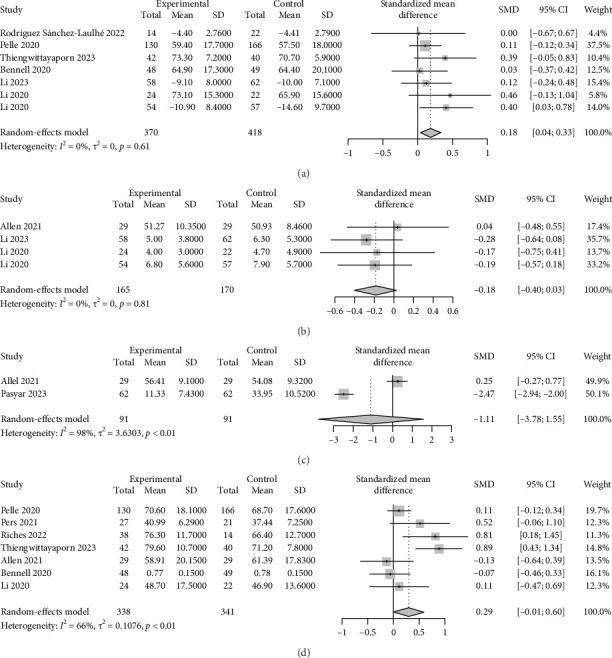 Figure 2
Figure 2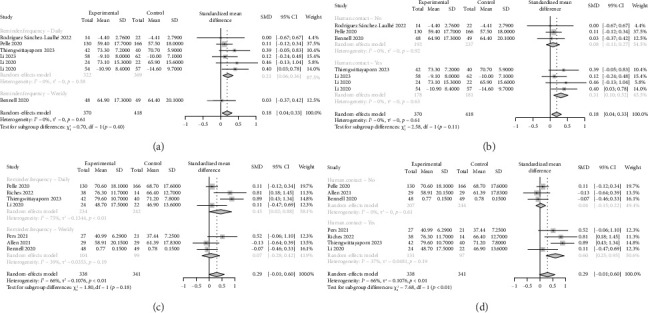 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibromyalgia and Chronic Fatigue Syndrome Research · Health, psychology, and well-being · Optimism, Hope, and Well-being
1. Introduction
Rheumatic diseases are a diverse group of inflammatory, frequently autoimmune conditions that affect the joints, muscles, bones, and organs and are associated with substantial morbidity and mortality [1, 2]. The most prevalent rheumatic diseases encompass rheumatoid arthritis, osteoarthritis, systemic lupus erythematosus, juvenile idiopathic arthritis, and gout [3, 4]. These conditions are often characterized by systemic inflammation and share common clinical features, including chronic pain, joint swelling, fatigue, and stiffness [5, 6]. These debilitating symptoms can lead to an increased risk of depression and anxiety [7–9] and significant reductions in quality of life [10, 11].
The treatment of rheumatic diseases has been revolutionized by a deeper understanding of the physiopathological connections over the last decades; however, many individuals with these conditions continue to face suboptimal management of their symptoms and ongoing challenges in their daily lives [12, 13]. The traditional models of care, which often rely on infrequent clinic visits and retrospective self-reporting of symptoms, may fail to capture the dynamic and context-dependent nature of rheumatic disease experiences [14, 15]. Moreover, these traditional models may not fully engage patients in their care or empower them to actively manage their condition between visits [16]. Consequently, there is a growing recognition of the need for more personalized, real-time approaches to symptom monitoring and intervention delivery in the management of rheumatic diseases [17, 18].
Ecological momentary interventions have emerged as a promising strategy for addressing the unique and fluctuating needs of individuals with rheumatic diseases. Ecological momentary interventions are defined as real-time interventions delivered within individuals' daily lives and natural environments, utilizing mobile technologies such as smartphones or wearable devices [19]. A key feature of ecological momentary interventions is their capacity for real-time delivery, which provides support during critical moments, such as during emotional distress or unhealthy behaviors, thus overcoming the limitations of scheduled therapy sessions [20]. Additionally, this approach utilizes data from ecological momentary assessments to tailor interventions to the user's specific needs, rather than applying a one-size-fits-all program [21]. By seamlessly integrating into the user's daily routine, ecological momentary interventions account for the individual's current environment and emotional state, thereby enhancing the relevance and effectiveness of the interventions [20, 21]. Contemporary research has begun to explore the application of ecological momentary interventions across a range of rheumatic disease populations. Several studies have investigated the use of ecological momentary interventions for pain management, with some evidence suggesting that these interventions can lead to reductions in pain intensity and improvements in pain-coping strategies among patients with systemic lupus erythematosus and osteoarthritis [22–24]. Additionally, there is an emerging literature on the use of ecological momentary interventions to support mental health [25, 26] and quality of life [27–30] in individuals with rheumatic diseases.
However, the overall effectiveness of ecological momentary interventions in this population has not been systematically reviewed and examined. Additionally, there is no summarized information about the ecological momentary intervention protocols for rheumatic diseases. As these may differ concerning their reminder strategy (e.g., daily or weekly) and supporting mechanisms (e.g., human contact or fully automated), there is a need to better describe the current ecological momentary interventions available to patients with rheumatic diseases and investigate their feasibility. Thus, the purpose of this study was to perform a systematic review and meta-analysis on the effectiveness of ecological momentary interventions in improving pain, mental health, and quality of life among individuals with rheumatic diseases.
2. Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used when conducting and reporting this systematic review [31]. The protocol was registered in PROSPERO (International Prospective Register of Systematic Reviews; CRD42024554432). Ethical approval was not required because there was no clinical intervention performed on patients, and all data were retrieved from published articles.
2.1. Search Strategy for Identification of Studies
A comprehensive literature search was conducted from inception to April 2024 using the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Embase, PsycINFO, Web of Science, Scopus, ProQuest, Wanfang Database, and China National Knowledge Infrastructure. The search strategy sample—Embase is provided in Supporting Table 1.
2.2. Study Selection Criteria
The articles were included based on the following PICOS criteria: (1) Population: Individuals diagnosed with rheumatic diseases; (2) Intervention: Ecological momentary intervention delivered in real-time or near real-time, utilizing data collected from specific moments in daily life, including ecological momentary assessments or a fixed timepoint obtained from individual experience [32]; (3) Comparison: No restrictions on the type of control groups, which may include attention control, standard care, routine care, or waitlist control; (4) Outcomes: Studies must quantitatively report at least one of the following outcomes: pain, quality of life, or mental health indicators (e.g., anxiety and depression); (5) Study design: RCTs or pilot RCTs.
Peer-reviewed studies published in English or Chinese were eligible, with no limitations on publication dates. Protocols, reviews, conference abstracts, and design/development papers without efficacy outcomes were excluded. Studies that used ecological momentary assessments solely for data collection or outcome measurement were also excluded.
2.3. Study Selection and Data Extraction
All records were imported into EndNote X9 [33]. After duplicates were removed, two reviewers (Xiaoxiao Mei and Jiaying Li) independently screened the titles and abstracts according to the established inclusion and exclusion criteria. Subsequently, a full-text assessment of potentially relevant studies was conducted by the same reviewers to identify eligible studies for inclusion in this review.
Data from the included studies were extracted independently by the same two reviewers using predesigned data collection forms guided by the Cochrane Handbook [34]. The following information was collected: (1) general information (first author, publication year, country, study design, and data analysis methods); (2) participants' characteristics (diagnosis, sample size, age, and gender distribution); (3) details of the interventions (frequency, duration, content of the ecological momentary intervention, response generation, human contact, feasibility and acceptability); (4) outcomes and measurement tools; and (5) main findings. Discrepancies were resolved through discussion and consensus, involving a third review author (L.Y.). The authors were contacted if clarification was needed.
2.4. Quality Assessment and Certainty of Evidence
The same two independent reviewers critically appraised the included studies using the Cochrane tool to evaluate the risk of bias (RoB 2.0) [35]. The RoB was assessed according to the following domains: (1) randomization process, (2) deviations from the intended interventions, (3) missing outcome data, (4) outcome measurement, and (5) selection of the reported result. Each domain was classified as “high RoB,” “low RoB,” or “some concerns.” The overall RoB for each outcome was judged as “low RoB” (all domains low), “some concerns” (at least one domain raised some concerns but no high risk), and “high RoB” (at least one domain high or multiple with some concerns) [35].
The overall quality of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework [36] by the same two reviewers. By default, the evidence of RCTs received a “high” initial grade, which was then downgraded based on prespecified criteria: RoB (assessed using RoB 2.0), inconsistency (substantial unexplained heterogeneity), indirectness (factors limiting generalizability), imprecision (considering total events/participants and 95% CI), and publication bias (evidence of small-study effects) [36].
2.5. Statistical Analysis
The outcomes in this study were measured using different scales; hence, standardized mean difference (SMD) and 95% confidence interval (CI) were applied. The SMD represents the difference in mean outcomes between baseline and study completion, standardized by the pooled standard deviation [37]. Given the expected variability between studies and outcome measurements, we employed a random-effects model to pool the SMDs across studies [38]. To assess the robustness of our findings, we conducted sensitivity analyses using a “leave-one-out” approach and re-estimated the overall effect [39]. This allowed us to evaluate the impact of any single study on the overall result. Subgroup analyses were performed based on reminder frequency (daily vs. weekly) and human contact involvement (yes vs. no). These subgroup analyses aimed to explore potential sources of heterogeneity and identify any differential effects across study design features. The convention proposed by Cohen [40] was used for the interpretation of the effect magnitude: trivial < 0.2, small ≥ 0.20, medium ≥ 0.50, and large ≥ 0.80. All statistical analyses were performed using the R 4.3.3 statistical software program (metaphor and meta package) [41].
3. Results
3.1. Literature Search
The database search identified 1773 studies. Following the removal of duplicates (n = 700), 1073 publications were screened for inclusion. Of these, 984 were excluded after reviewing the title and abstract. The remaining 89 papers were selected for full reading, and 74 were excluded because they did not include ecological momentary intervention (n = 59), no rheumatic diseases (n = 9), no outcome of interest (n = 4), or no full-text available (n = 1). Therefore, 16 studies were included in the review. However, we were unable to obtain relevant data from 5 studies [23, 27, 42–44] (i.e., data were presented graphically only or without mean difference and standard deviation, and authors did not respond to the emails soliciting the required data after multiple attempts). Therefore, 11 studies were included in the meta-analysis (Figure 1).
3.2. Study Characteristics
The characteristics of the included studies are shown in Table 1. Among the 16 included studies, 14 were RCTs, one was a pilot RCT, and one was reported as a pilot and feasibility RCT. In total, these studies enrolled 1869 participants, comprising 466 men and 1403 women. The study population was predominantly composed of adult participants (age > 18 years), with only one study including adolescent participants (mean age 15 years). Six studies focused on participants with knee or hip osteoarthritis, four studies included participants with rheumatoid arthritis, and three studies enrolled participants with systemic lupus erythematosus. Additionally, there was one study each that investigated participants with juvenile idiopathic arthritis and gout, and one study that included participants with either systemic lupus erythematosus or rheumatoid arthritis.
3.3. Intervention Characteristics
Table 2 summarizes the characteristics of the ecological momentary interventions. Overall, nine studies [22, 23, 25, 26, 29, 30, 42, 43, 45] addressed ecological momentary interventions based on self-management techniques, and four studies [44, 46–48] investigated ecological momentary interventions utilizing behavior change techniques. Two studies [27, 28] examined ecological momentary interventions grounded in an intensive treat-to-target strategy, and one study [24] explored ecological momentary interventions founded on pain-coping skills training.
The majority of studies utilized apps for participant data input [22, 24, 25, 27–30, 44, 45, 47, 48], whereas two studies employed short message service [26, 46]. Most studies adopted a daily ecological momentary assessment prompt schedule [22, 23, 25, 26, 29, 30, 42, 43, 45, 47, 48], while four studies used a weekly ecological momentary assessment prompt schedule [24, 28, 44, 46]. Only one study administered 13 text message prompts at 1- to 2-week intervals over 24 weeks [27].
Six studies utilized an artificial intelligence-based system to generate intervention responses, while 10 studies relied on pre-established rules. Besides, the ecological momentary intervention system automatically provided participants with tailored recommendations and motivational feedback without human involvement in six studies, whereas in 10 studies, researchers delivered personalized feedback and recommendations to participants using ecological momentary assessment results.
3.4. RoB and Certainty of Evidence
The RoB is shown in Supporting Figure 1. Overall, 13 studies were rated as having a high RoB [22–29, 43–45, 47, 48]. Ten studies presented some concerns in the randomization process [27, 44, 45] or the selection of the reported results [24, 26–30, 42, 43]. Additionally, one study presented the RoB due to missing outcome data [45]. Moreover, 13 studies were found to have a RoB in the measurement of the outcome due to a lack of blinding [22–29, 43–45, 47, 48].
From the GRADE approach, the evidence of the certainty of pain, depression, anxiety, and quality of life was graded as moderate, low, very low, and very low, respectively. The degrading factors mainly originated from the RoB of included studies, imprecision of results, and the heterogeneity across studies. The details of the GRADE evaluation are shown in Supporting Table 2.
3.5. Effects of Interventions
3.5.1. Pain
Pain was evaluated using generic (e.g., visual analog scale, numeric rating scale, McGill pain questionnaire) [23, 25, 42, 45, 48] or disease-specific questionnaires [22, 30, 43, 44, 46, 47] across 11 studies. Two studies reported between-group reductions in pain [22, 23], while one study found within-group reductions after the ecological momentary intervention [44]. The overall meta-analysis revealed a trivial but statistically significant reduction in pain in the ecological momentary intervention groups compared to controls (SMD = 0.18, 95% CI: 0.04–0.33; I^2^ = 0%, p=0.61, Figure 2(a)). The result of the sensitivity analysis for pain presented in Supporting Figure 2 indicated that the results were stable. Subgroup analyses further elucidated these findings. Specifically, pain reduction was significantly greater in participants who received daily reminders (SMD = 0.21, 95% CI: 0.06–0.36; I^2^ = 0%, p=0.58), whereas there was no significant difference in pain between weekly reminder ecological momentary intervention groups and controls (SMD = 0.03, 95% CI: −0.37–0.42, Figure 3(a)). Additionally, the reduction in pain was significantly greater in participants who received ecological momentary interventions that involved human contact (SMD = 0.31, 95% CI: 0.10–0.52; I^2^ = 0%, p=0.63), but not in those who received ecological momentary interventions without human contact (SMD = 0.08, 95% CI: −0.11–0.27; I^2^ = 0%, p=0.92; Figure 3(b)).
3.5.2. Depression and Anxiety
Depression was evaluated in 4 studies using the Patient Health Questionnaire-9 items [25, 47, 48] or depression domains of PROMIS-29 [24], among which 1 study observed a reduction in this outcome after the ecological momentary intervention [25]. The overall meta-analysis revealed a small but marginally significant reduction in depression scores in the ecological momentary intervention groups compared to the controls (SMD = −0.18, 95% CI: −0.40–0.03; I^2^ = 0%, p=0.81, Figure 2(b)). The result of the sensitivity analysis for depression presented in Supporting Figure 3 indicated that the results were stable. Only two studies reported changes in anxiety using anxiety domains of PROMIS-29 [24] or health anxiety inventory [26], with one study showing significantly lower anxiety scores in the ecological momentary intervention group compared to the control group [26]. However, the overall meta-analysis did not find statistically significant reductions in anxiety between the ecological momentary intervention and control groups (SMD = −1.11, 95% CI: −3.78–1.55; I^2^ = 98%, p < 0.01; Figure 2(c)). The result of the sensitivity analysis for anxiety presented in Supporting Figure 4 showed that the pooled result was the opposite after removing the study by Allen et al. [24], which may have been influenced by low participant engagement with the ecological momentary interventions.
3.5.3. Quality of Life
Quality of life was assessed in 11 studies, using generic (e.g., EuroQoL 5-Dimension 3-Level questionnaire, 12-item short-form health survey) [22, 27–29, 46] or disease-specific questionnaires [24, 30, 42–44, 47]. Four studies reported between-group improvements in quality of life or specific quality-of-life domains [27–30], while two studies found within-group enhancement after the ecological momentary intervention [44]. The overall meta-analysis demonstrated a small but marginally significant improvement in quality of life favoring the ecological momentary intervention groups over controls (SMD = 0.29, 95% CI: −0.01–0.60; I^2^ = 66%, p < 0.01, Figure 2(d)). The result of the sensitivity analysis for quality of life presented in Supporting Figure 5 revealed that the overall findings were sensitive to the exclusion of the studies by Allen et al. [24] and Bennell et al. [46], which may have been influenced by low participant engagement with the ecological momentary interventions. Subgroup analysis further revealed that the improvement of quality of life was more pronounced in participants who received daily reminders (SMD = 0.45, 95% CI: 0.02–0.88; I^2^ = 75%, p < 0.01), whereas there was not any significant difference between participants in weekly reminder ecological momentary intervention groups and controls (SMD = 0.07, 95% CI: −0.28–0.42; I^2^ = 39%, p=0.19; Figure 3(c)). Additionally, the improvement in quality of life was significantly greater in participants who received ecological momentary interventions that involved human contact (SMD = 0.60, 95% CI: 0.25–0.95; I^2^ = 37%, p=0.19), but not in those who received ecological momentary interventions without human contact (SMD = 0.04, 95% CI: −0.15–0.22; I^2^ = 0%, p=0.61; Figure 3(d)).
3.6. Feasibility and Acceptability
The majority of studies (11 out of 16) reported data on participants' engagement with the ecological momentary interventions. Eight studies provided metrics on the percentage of app usage [22–24, 42, 44, 46–48], while three studies reported the mean duration between two app usage records [25, 28, 29]. Notably, one study found that only 50% of participants in the ecological momentary intervention group used the app [24]. In contrast, a substantially higher rate of app usage was reported by Gohir et al. (87.9%) [23] and Li et al. (83.1%) [48].
In terms of participant satisfaction, seven studies reported relevant data [22, 24, 25, 27–29, 42]. The studies by Kuusalo [27] and Riches [29] showed that 97.6% and 93.0% of participants in the ecological momentary intervention groups provided positive evaluations of the interventions, respectively. However, Pelle et al. [22] found that only 26% of participants were willing to continue using the app after the intervention ended.
Regarding the safety of the ecological momentary interventions, eight studies reported adverse [25, 28, 29, 45, 47, 48] or serious adverse events [23, 27] were observed during the interventions. However, the authors explicitly stated that these adverse events were not attributed to the ecological momentary interventions themselves (Table 1).
4. Discussion
4.1. Main Findings
To our knowledge, this was the first meta-analysis to evaluate the efficacy of ecological momentary interventions in reducing pain, improving mental health, and enhancing quality of life among individuals with rheumatic diseases. We found moderate-quality evidence that ecological momentary interventions significantly reduce pain. However, the evidence was of low or very low quality for the effects of ecological momentary interventions on mental health outcomes, and there was no statistically significant impact on depression and anxiety. For quality of life, the analysis revealed low-quality evidence that ecological momentary interventions had a marginally significant effect in improving quality of life. These findings suggest the need for more high-quality RCTs to draw robust conclusions about the benefits of ecological momentary interventions for individuals with rheumatic diseases.
4.2. Interpretation of Findings
4.2.1. Effect of Ecological Momentary Interventions on Pain
The moderate-certainty evidence that ecological momentary interventions can significantly reduce pain among individuals with rheumatic diseases supports the use of these interventions for pain management in this population. This beneficial effect is likely attributable to the incorporation of self-management techniques or behavior change strategies in the included studies. These approaches have been considered favorable solutions for alleviating pain in chronic conditions, as they can empower participants to take personal responsibility for monitoring and managing their health status throughout diseases [49, 50]. Ecological momentary interventions that provided daily reminders had a larger effect on pain relief compared to those with weekly reminders, possibly by helping participants maintain a sustained focus on disease management and enhancing adherence [51]. Additionally, ecological momentary interventions with daily reminders can closely monitor participants' pain status and make timely adjustments to the intervention measures based on the feedback, leading to better pain relief outcomes. This is consistent with previous research, suggesting that high-frequency assessments are more effective in symptom improvement [52]. Besides, ecological momentary interventions involving human involvement, such as clinician or researcher interactions, demonstrated more significant pain-reducing effects than automated ecological momentary intervention delivery. This may be due to the development of a stronger sense of responsibility and willingness to actively participate in the intervention when participants have regular contact with healthcare providers, who can also deliver more personalized feedback and support [53–55].
4.2.2. Effect of Ecological Momentary Interventions on Mental Health
Contrary to our expectations, the meta-analysis found no statistically significant effect of ecological momentary interventions on depression and anxiety among individuals with rheumatic diseases. This is noteworthy that depression and anxiety are strongly associated with psychosocial factors, such as negative emotions, low social support, and maladaptive coping mechanisms [7, 56, 57]. However, the majority of the ecological momentary interventions were primarily designed to target physical activity (N = 3, 60%), or pain management (N = 1, 20%), rather than incorporating specific modules to address the psychosocial aspects of mental health. This mismatch between the intervention contents and the intended mental health outcomes may have reduced the intervention's ability to effectively alleviate symptoms of depression and anxiety [58, 59]. The lack of effect may also be partially attributed to the opposite results reported in a single study [24]. Additionally, the very low and low certainty of the evidence, due to methodological limitations and heterogeneity across studies, may have contributed to the statistically insignificant findings on mental health outcomes.
4.2.3. Effect of Ecological Momentary Interventions on Quality of Life
The results suggest that ecological momentary interventions marginally improve quality of life for individuals with rheumatic diseases, which may be primarily driven by the beneficial effect of ecological momentary interventions in reducing pain since pain is a key factor influencing quality of life [60]. Furthermore, promptly addressing any problems or challenges encountered by participants through the ecological momentary intervention platform can help resolve issues that may otherwise negatively impact their quality of life [61]. The finding that daily reminders led to greater quality-of-life benefits than weekly reminders highlights the importance of intervention intensity, as more frequent prompts can enhance patient adherence and engagement [19]. Then, regular exposure to the intervention could help foster habit formation and improve self-monitoring skills, thereby improving quality of life [19, 62]. Furthermore, ecological momentary interventions involving human involvement demonstrated stronger quality-of-life outcomes than automated ecological momentary intervention delivery. Direct engagement with healthcare providers likely enhances the clinical relevance, personalization, and accountability of the self-management strategies or behavior change techniques delivered through the ecological momentary interventions [63]. Participants may feel more supported, empowered, and confident in managing their condition when they can access expert guidance and tailored recommendations, leading to a better quality of life [58, 64].
4.3. Feasibility and Acceptability
The variability observed in user engagement metrics, ranging from low to high adoption rates, suggests that maintaining consistent and meaningful usage of ecological momentary interventions remains a significant challenge. Some principles, such as user-centered design and gamification, are strongly recommended for designing platforms to increase the engagement of users [65, 66]. The mixed results on participant satisfaction also highlight the importance of carefully evaluating the acceptability of ecological momentary interventions from the end-user perspective, as developing interventions that not only provide immediate utility but also foster long-term adoption and continued use will be crucial [67]. Encouragingly, the lack of safety concerns directly attributed to the ecological momentary interventions themselves is a positive indication that these digital tools can be implemented with acceptable risk profiles, supporting the continued exploration and refinement of ecological momentary interventions as adjuncts or alternatives to traditional modes of healthcare delivery.
4.4. Limitation
This review has several limitations. First, this study only involved 4 rheumatic diseases (rheumatoid arthritis, osteoarthritis, systemic lupus erythematosus, and juvenile idiopathic arthritis), and most of the included studies had relatively small sample sizes. Therefore, caution should be taken when generalizing the findings to other rheumatic diseases. Second, some authors did not respond to the data request emails, and some current data were not included in the analyses, which may have impacted the comprehensiveness of the analyses. Additionally, the heterogeneity in the delivery models, components, durations, and outcome measures may have introduced clinical heterogeneity, despite our efforts to apply strict inclusion criteria to reduce such heterogeneity. Finally, a majority of the included trials exhibited measurement biases and unclear selection processes. The quality of the evidence, as assessed using the GRADE criteria, ranged from very low to moderate (Supporting Table 2). Consequently, the results should be interpreted with appropriate caution.
4.5. Implications
This study provides supporting evidence for the potential benefits of ecological momentary interventions in improving health outcomes for individuals with rheumatic diseases. As such, healthcare providers should consider integrating ecological momentary interventions into routine care as a complementary approach to optimize existing healthcare management strategies. Also, when designing future ecological momentary interventions, research should focus on optimizing the parameter settings, such as reminder frequency, and human-interactive elements, to enhance their efficacy. Additionally, further evaluation of the effectiveness of ecological momentary interventions in different rheumatic disease subtypes is needed to strengthen the evidence base for clinical application. Despite the positive impact of ecological momentary interventions on pain and quality of life, the study findings indicate that they have not yet achieved significant improvements in mental health indicators, such as anxiety and depression. Therefore, future research should prioritize the optimization of ecological momentary intervention design and implementation to better address the mental health needs of individuals with rheumatic diseases. Furthermore, high-quality RCTs are still needed to rigorously validate the effects of ecological momentary interventions and provide more robust evidence to guide clinical practice.
5. Conclusion
Our review demonstrated that ecological momentary interventions can, to some extent, alleviate pain and improve quality of life among individuals with rheumatic diseases, but have not achieved significant improvements in anxiety and depression. Future research should focus on further optimizing the design and implementation of ecological momentary interventions and delving deeper into their impact on mental health. Ecological momentary interventions represent an innovative approach that deserves further promotion and application in the clinical management of rheumatic diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Goldblatt F. O’Neill S. G. Clinical Aspects of Autoimmune Rheumatic Diseases The Lancet 2013382989479780810.1016/S 0140-6736(13)61499-32-s 2.0-8488312823223993190 · doi ↗ · pubmed ↗
- 2Dong L. Umehara H. Zhong J. Editorial:Rheumatic Diseases and Infection Frontiers of Medicine 20229 p. 94167810.3389/fmed.2022.941678 PMC 919856735721091 · doi ↗ · pubmed ↗
- 3Jokar M. Jokar M. Prevalence of Inflammatory Rheumatic Diseases in a Rheumatologic Outpatient Clinic: Analysis of 12626 Cases Rheumatology Research 201831212710.22631/rr.2017.69997.1037 · doi ↗
- 4Kwiatkowska B. Raciborski F. Kłak A. Maślińska M. Gryglewicz J. Early Diagnosis of Rheumatic Diseases: An Evaluation of the Present Situation and Proposed Changes Reumatologia 20155313810.5114/reum.2015.505502-s 2.0-8492752369827407218 PMC 4847309 · doi ↗ · pubmed ↗
- 5Khallaf M. K. Al Sergany M. A. El-Saadany H. M. Abo El-Hawa M. A. Ahmed R. A. M. Assessment of Fatigue and Functional Impairment in Patients with Rheumatic Diseases The Egyptian Rheumatologist 2020421515610.1016/j.ejr.2019.04.0092-s 2.0-85065326738 · doi ↗
- 6Atzeni F. Masala I. F. Salaffi F. Di Franco M. Casale R. Sarzi-Puttini P. Pain in Systemic Inflammatory Rheumatic Diseases Best Practice & Research Clinical Rheumatology 2015291425210.1016/j.berh.2015.04.0162-s 2.0-8493898840226266998 · doi ↗ · pubmed ↗
- 7Ziarko M. Siemiątkowska K. Sieński M. Samborski W. Samborska J. Mojs E. Mental Health and Rheumatoid Arthritis: Toward Understanding the Emotional Status of People With Chronic Disease Bio Med Research International 2019201911810.1155/2019/14739252-s 2.0-85062363727 PMC 638831530886858 · doi ↗ · pubmed ↗
- 8Torta R. Pennazio F. Ieraci V. Anxiety and Depression in Rheumatologic Diseases: The Relevance of Diagnosis and Management Reumatismo 2014661929710.4081/reumatismo.2014.7692-s 2.0-8490219740124938201 · doi ↗ · pubmed ↗