Guillain–Barre Syndrome in Patients With Cystic Fibrosis: A Case Series
James Nolan, Maxter Thai, Vanessa Moore, Daniel Henderson, David Reid

TL;DR
This paper reports four cases of Guillain–Barre Syndrome in adults with cystic fibrosis, highlighting the rare but severe neurological complications in this patient group.
Contribution
The novelty lies in documenting multiple cases of GBS in CF patients and exploring potential links to chronic inflammation and CFTR dysfunction.
Findings
Four adult CF patients developed Guillain–Barre Syndrome.
GBS in CF patients may be linked to chronic inflammation or dysfunctional CFTR protein.
GBS has a particularly detrimental impact in CF patients due to pre-existing lung and metabolic issues.
Abstract
People with cystic fibrosis (CF) typically experience chronic respiratory infections, but neurological sequelae are rare. Guillain–Barre Syndrome (GBS) is classically precipitated by a respiratory or gastrointestinal infection, although other rarer aetiologies exist. This case series outlines four adults with CF who developed GBS. The association with acute and chronic respiratory infections in people with CF is explored, as well as other potential precipitants. An autoimmune phenomenon in the context of chronic systemic inflammation or a possible contributory role of dysfunctional CFTR protein is also considered. We present four cases of Guillain–Barre Syndrome in adult patients with cystic fibrosis. We highlight the particularly detrimental impact that can occur in a population of patients with chronic underlying suppurative airway disease, impaired lung function and metabolic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
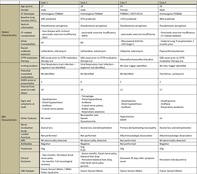 Figure 1
Figure 1| Case 1 | Case 2 | Case 3 | Case 4 | ||
|---|---|---|---|---|---|
| Patient Characteristics | Age (years) | 27 | 18 | 54 | 29 |
| Gender | Male | Male | Female | Male | |
| CF genotype | Homozygous F508del | Homozygous F508del | F508del/2657+5G>A | Homozygous F508del | |
| Baseline lung function (FEV1) | 40% predicted | 97% predicted | < 15% predicted | 98% predicted | |
| Sputum colonisation |
|
|
|
| |
| CF‐related complications |
Liver disease with cirrhosis Pancreatic exocrine insufficiency DIOS |
Pancreatic exocrine insufficiency ABPA | Pancreatic exocrine insufficiency |
Pancreatic exocrine insufficiency CF‐related diabetes | |
| Other Comorbidities | Nil | Nil |
Rheumatoid arthritis CKD Stage II | Bilateral lung transplantation 2 months prior | |
| Recent antibiotic exposure | Ceftazidime, tobramycin | Ceftazidime, tobramycin | Cefepime, tobramycin | Piperacillin/tazobactam | |
| CFTR modulator therapy | GBS onset prior to CFTR modulator therapy era | GBS onset prior to CFTR modulator therapy era | Elexacaftor/tezacaftor/ivacaftor | GBS onset prior to CFTR modulator therapy era | |
| GBS characteristics | Inciting incident | Viral Respiratory tract infection—organism not identified | Viral Respiratory tract infection—organism not identified | Nil clear trigger identified | Nil clear trigger identified |
| Potential associated medications | Nil identified | Nil identified | Nil identified | Tacrolimus, cyclosporin | |
| EGRIS score at presentation | 2 | 4 | 2 | 2 | |
| Interval from onset to nadir (days) | 10 | 10 | 12 | 17 | |
| Signs and symptoms at nadir |
Quadriparesis Distal hypoesthesia Areflexia Cranial nerve palsies |
Tetraplegia Distal hypoesthesia Areflexia Cranial nerve palsies Bulbar palsy Respiratory weakness |
Quadriparesis Distal hypoesthesia Areflexia |
Quadriparesis Areflexia Respiratory weakness | |
| Other features | Nil noted |
Neuropathic pain Sweats Dysautonomia |
Hypertension SIADH | Nil | |
| Nerve conduction study | Axonal loss | Axonal loss and demyelination | Primary demyelinating neuropathy | Axonal loss and demyelination | |
| Lumber puncture | Not performed | Not performed | Albuminocytologic dissociation | Albuminocytologic dissociation | |
| MRI | Nil abnormality detected | Nil abnormality detected | Not performed | Nil abnormality detected | |
| Antibodies | Negative | Negative | Not performed | Negative | |
| Treatment | IVIg |
IVIg PLEX | IVIg | IVIg | |
| Clinical Outcome |
Two months: persistent facial nerve palsy Six months: full neurological recovery |
Seven months: Facial nerve palsy, bilateral foot drop Persistent bilateral foot drop, mild facial nerve palsy persists | Deceased 39 days after symptom onset | Persistent mild dysarthria | |
| GBS Subtype | Classic sensori‐motor/Miller Fisher syndrome | Classic sensori‐motor | Classic sensori‐motor | Classic sensori‐motor |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Myasthenia Gravis and Thymoma
Introduction
1
Cystic fibrosis (CF) is an autosomal recessive disease caused by mutations in the CF transmembrane conductance regulator (CFTR) gene with multi‐system effects including pulmonary, gastrointestinal, endocrinological, musculoskeletal and genitourinary. The lungs are the most severely affected organ, with chronic airway bacterial infection causing progressive deterioration in lung function [1]. Rare descriptions of neurological abnormalities in CF patients, particularly peripheral neuropathy, are hypothesised to be secondary to CF‐related diabetes, micronutrient deficiencies, or due to a yet unknown immunological aetiology [2].
Guillain–Barre syndrome (GBS) is an eponym encompassing acute inflammatory demyelinating polyneuropathies (AIDP). Classically precipitated by a respiratory or gastrointestinal infection, GBS is characterised by progressive, symmetrical, flaccid muscle weakness, areflexia and ascending sensory changes. GBS occurs secondary to molecular mimicry, and the resultant cross‐reactivity of an immune response to a preceding infection with components of peripheral nerves. It is a heterogeneous syndrome with multiple variants, and the dysregulated immune response can cause both axonal loss and demyelination [3].
Here, we present four cases of GBS in adult patients with CF. We highlight the particularly detrimental impact that can occur in a population of patients with chronic underlying suppurative airway disease, impaired lung function and metabolic dysregulation.
Case Series
2
Table 1 provides a summary of baseline patient characteristics and clinical presentation, clinical course and treatment of GBS in the case series cohort.
Case 1
2.1
A 27‐year‐old male diagnosed with CF (homozygous for F508del CFTR mutation) was admitted to hospital with 5 days of progressive peripheral weakness, 3 days of peripheral paraesthesia and a 1‐day history of intermittent diplopia, with increasing difficulty performing airway clearance, occurring two weeks following an unidentified upper respiratory tract infection (URTI). His medical history was relevant for moderately severe CF‐related bronchiectasis, CF‐related liver disease with Child–Pugh A Cirrhosis and pancreatic exocrine insufficiency. Areflexia with progressive peripheral weakness and the development of facial nerve and bulbar weakness and bilateral diplopia were noted on presentation; however, spirometry remained stable throughout admission. Treatment with intravenous immunoglobulin (IVIg) was provided. Hospitalisation was complicated by a pulmonary exacerbation of CF, for which targeted antimicrobial therapy was provided. Standard airway clearance techniques proved difficult due to facial and bulbar weakness. Symptoms stabilised at Day 5 of admission before gradually improving until hospital discharge on Day 17. At 2 months follow‐up, mild facial nerve palsy persisted, but with complete neurological recovery evident at 6 months.
Case 2
2.2
An 18‐year‐old male with CF (homozygous for F508del CFTR mutation) was admitted to hospital for management of a pulmonary exacerbation of CF‐related bronchiectasis on the background of an unidentified URTI 2 weeks prior. A concomitant 3‐day history of progressive peripheral upper and lower limb weakness and paraesthesia was volunteered. Medical history was relevant for mild CF‐related bronchiectasis, pancreatic exocrine insufficiency and allergic bronchopulmonary aspergillosis (ABPA). Areflexia and rapidly progressive tetraplegia were evident on presentation, with associated bulbar weakness and declining respiratory function. IVIg was commenced, but rapidly progressive bulbar and respiratory involvement resulted in an intensive care unit (ICU) admission (on Day 3 of admission) for intubation and ventilation. During a 73‐day ICU admission, plasma exchange (PLEX) and IVIg therapy were provided and a tracheostomy was performed. Hospitalisation was complicated by severe neuropathic pain, autonomic dysfunction and pneumonia. A further 15‐day acute and 84‐day inpatient rehabilitation hospitalisation followed. On discharge, there was residual peripheral lower limb paraplegia and cranial nerve palsy, with modest improvement over 5‐year follow‐up.
Case 3
2.3
A 54‐year‐old female with CF (F508del/2657+5G>A) was admitted to hospital with a pulmonary exacerbation of CF‐related bronchiectasis and a 3‐day history of increasing distal paraesthesia. Her medical history was relevant for severe CF‐related bronchiectasis complicated by chronic hypoxia and hypercarbia managed with long‐term oxygen therapy (LTOT) and nocturnal non‐invasive ventilation (NIV), pancreatic exocrine insufficiency, quiescent rheumatoid arthritis (RA) and Chronic Kidney Disease Stage II. Admission neurological examination was consistent with previously documented mild lower limb peripheral neuropathy secondary to RA. Treatment for a pulmonary exacerbation with intravenous antibiotics was initiated. On Day 4 of admission, progressive lower limb, then upper limb weakness with hyporeflexia developed. Treatment with IVIg was provided. Admission was complicated by acute on chronic hypercapnic respiratory failure and Clostridium difficile infection. Despite improvement in peripheral neurology, the patient's respiratory status deteriorated, secondary to the pulmonary exacerbation of CF‐related bronchiectasis and she died on Day 36 of hospitalisation.
Case 4
2.4
A 29‐year‐old male with CF (homozygous for F508del CFTR mutation) was admitted to hospital with a one‐week history of progressive lower limb weakness and increasing falls without preceding illness. His medical history was relevant for a bilateral lung transplantation 2 months prior for severe CF‐related bronchiectasis. Neurological examination demonstrated progressive lower and upper limb weakness, with bulbar involvement. Respiratory involvement was evident on declining spirometry. IVIg therapy was provided, tacrolimus and cyclosporin immunosuppression were switched to everolimus and mycophenolate due to the potential association with GBS. A 73‐day hospitalisation was complicated by pneumonia. Neurological function improved, but at long‐term follow‐up, residual dysarthria remains.
Discussion
3
To our knowledge, these four cases represent the first descriptions of GBS occurring in adults with CF. Three patients developed serious short‐term sequelae, whilst one patient died as a consequence of underlying very severe CF‐related bronchiectasis compounded by exacerbation of ventilatory failure by GBS. Of the three surviving patients, all demonstrated slow neurological recovery, with two experiencing permanent neurological effects. The care for all patients was complex and required significant multidisciplinary input. Particularly challenging were the impact of a progressive neuropathy on mobility, airway clearance, nutrition and hydration; the cornerstones of CF care.
The reported incidence of GBS in Australia is 1.7 per 100,000 population/year, and our CF centre cares for approximately 350 patients across a wide geographic area. Given the dispersion in time, patient geographic residence and season at time of hospitalisation of each of the described cases, no unifying aetiology for our cohort has been identified. At our institution, most adults with CF have been diagnosed in childhood, via standard diagnostic means and initially managed through specialist paediatric CF services prior to transition to adult care [1].
Whilst there are multiple established or proposed causal associations, the majority of GBS cases occur post respiratory or gastrointestinal infections, with URTIs the probable precipitant in two of our reported cases [4]. It is notable that in two cases a clear preceding infection was not identified. Several non‐infectious aetiologies for GBS have been suggested, and a wide range of potential aetiologies were considered in each of our reported cases. Only in case Four were potential medications previously associated with GBS, tacrolimus and cyclosporin, present and thus identified as a potential cause and promptly ceased [5, 6]. The antimicrobial agent colistin has also been identified as a potential GBS mimic, but none of our patients demonstrated a temporal exposure to this or similar antimicrobial agents [7]. Finally, all patients in this case series had exocrine pancreatic insufficiency, a risk factor for vitamin and mineral deficiency, which are recognised causes of peripheral neuropathy in patients with CF [2]. It is standard practice in our centre that all patients receive regular guideline‐directed nutritional supplementation and regular monitoring to ensure against micronutrient deficiency [8]. It is also notable that there was no reported family history of GBS or other neurological disorder.
People with CF classically experience acute and chronic respiratory infection caused by a wide range of pathogens [9]. It is worth considering that CF‐associated chronic systemic inflammation, alterations in immune function and microbiological dysbiosis represent risk factors for the development of molecular mimicry and autoimmune phenomena [10]. Interestingly, the CFTR protein has a role in airway epithelial cell wound healing following injury. Due to absent or dysfunctional CFTR, there is reduced production of GM1 gangliosides, which are involved in cell–cell communication and exert anti‐inflammatory effects [11]. Anti‐GM1 ganglioside antibodies are detected in approximately 60% of patients with GBS [4]. Whether there is a link between a pre‐existing cellular deficiency of GM1 gangliosides in CF and susceptibility to neuronal injury could be theorised. However, it is notable that anti‐GM1 antibodies were not detected in any patients in our case series.
Although an association between GBS and CF has not been previously reported, this case series should focus the attention of CF physicians towards early consideration, investigation and neurological referral. A high index of suspicion could lead to earlier diagnosis and management, and subsequently improve patient outcomes. Given the observed morbidity and mortality highlighted by this case series, prompt treatment should be considered in any person with CF exhibiting a clinical syndrome concerning GBS. This case series also adds to the growing literature on the extra‐pulmonary role of the CFTR protein and CF‐related autoimmune phenomenon.
Author Contributions
All authors contributed equally to the development of this manuscript.
Ethics Statement
All patients provided consent, and ethics approval to report this case series was obtained from the local ethics committee (HREC/2023/MNHA/100792).
Consent
The authors declare that written informed consent was obtained from all the patients for the publication of this manuscript and accompanying images and attest that the form used to obtain consent from the patients complies with the Journal requirements as outlined in the author guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1S. C. Bell , M. A. Mall , H. Gutierrez , et al., “The Future of Cystic Fibrosis Care: A Global Perspective,” Lancet Respiratory Medicine 8, no. 1 (2020): 65–124, 10.1016/S 2213-2600(19)30337-6.31570318 PMC 8862661 · doi ↗ · pubmed ↗
- 2B. Chakrabarty , S. K. Kabra , S. Gulati , et al., “Peripheral Neuropathy in Cystic Fibrosis: A Prevalence Study,” Journal of Cystic Fibrosis 12, no. 6 (2013): 754–760, 10.1016/j.jcf.2013.01.005.23391476 · doi ↗ · pubmed ↗
- 3N. Shahrizaila , H. C. Lehmann , and S. Kuwabara , “Guillain‐Barré Syndrome,” Lancet 397, no. 10280 (2021): 1214–1228, 10.1016/S 0140-6736(21)00517-1.33647239 · doi ↗ · pubmed ↗
- 4R. Bellanti and S. Rinaldi , “Guillain‐Barré Syndrome: A Comprehensive Review,” European Journal of Neurology 31, no. 8 (2024): e 16365, 10.1111/ene.16365.38813755 PMC 11235944 · doi ↗ · pubmed ↗
- 5J. A. Falk , F. C. Cordova , A. Popescu , G. Tatarian , and G. J. Criner , “Treatment of Guillain‐Barré Syndrome Induced by Cyclosporine in a Lung Transplant Patient,” Journal of Heart and Lung Transplantation 25, no. 1 (2006): 140–143, 10.1016/j.healun.2005.06.012.16399546 · doi ↗ · pubmed ↗
- 6N. S. Sharma , K. M. Wille , C. W. Hoopes , and E. Diaz‐Guzman , “Acute Demyelinating Polyneuropathy After Lung Transplantation: Guillain–Barré Syndrome or Tacrolimus Toxicity?,” Case Reports in Transplantation 2014 (2014): 685010, 10.1155/2014/685010.25184071 PMC 4144080 · doi ↗ · pubmed ↗
- 7C. Camargo , T. Narula , D. A. Jackson , T. Padro , and W. D. Freeman , “Colistin Neurotoxicity Mimicking Guillain‐Barré Syndrome in a Patient With Cystic Fibrosis: Case Report and Review,” Oxford Medical Case Reports 2021, no. 9 (2021): omab 080, 10.1093/omcr/omab 080.34527253 PMC 8436279 · doi ↗ · pubmed ↗
- 8N. Saxby , C. Painter , A. Kench , et al., Nutrition Guidelines for Cystic Fibrosis in Australia and New Zealand, ed. S. C. Bell (Thoracic Society of Australia and New Zealand, 2017).10.1016/j.jcf.2019.05.00731175004 · doi ↗ · pubmed ↗