A Case Report and Literature Review on a Primary Dedifferentiated Liposarcoma of the Gallbladder
Victoria Xie, Richard Dominic Luyun, Justin Rivard, Mohamed Akra, Yi Yan, Miao Lu

TL;DR
A rare case of primary dedifferentiated liposarcoma in the gallbladder is reported, highlighting the importance of accurate diagnosis for proper treatment.
Contribution
This case report adds to the limited literature on gallbladder DDLPS and emphasizes its inclusion in differential diagnoses.
Findings
DDLPS was identified in a gallbladder mass via histopathology and FISH confirming MDM2 amplification.
DDLPS should be considered in the differential diagnosis of atypical gallbladder masses.
Accurate diagnosis is crucial for surgical planning and patient management in such rare cases.
Abstract
Primary dedifferentiated liposarcoma (DDLPS) of the gallbladder is an exceptionally rare neoplasm. We present a case of incidentally discovered gallbladder DDLPS identified during routine surveillance abdominal computed tomography (CT) in a patient with a history of low-grade papillary urothelial carcinoma of the bladder. The mass was initially suspected to be primary gallbladder carcinoma, prompting cholecystectomy. Histopathologic examination revealed a high-grade sarcomatous nodule within the gallbladder adventitia, sharply demarcated from an adjacent well-differentiated liposarcoma (WDLPS) component. The diagnosis of DDLPS was confirmed by fluorescence in situ hybridization (FISH) demonstrating MDM2 gene amplification. This case expands the limited literature on gallbladder DDLPS and emphasizes the importance of including liposarcoma in the differential diagnosis of atypical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
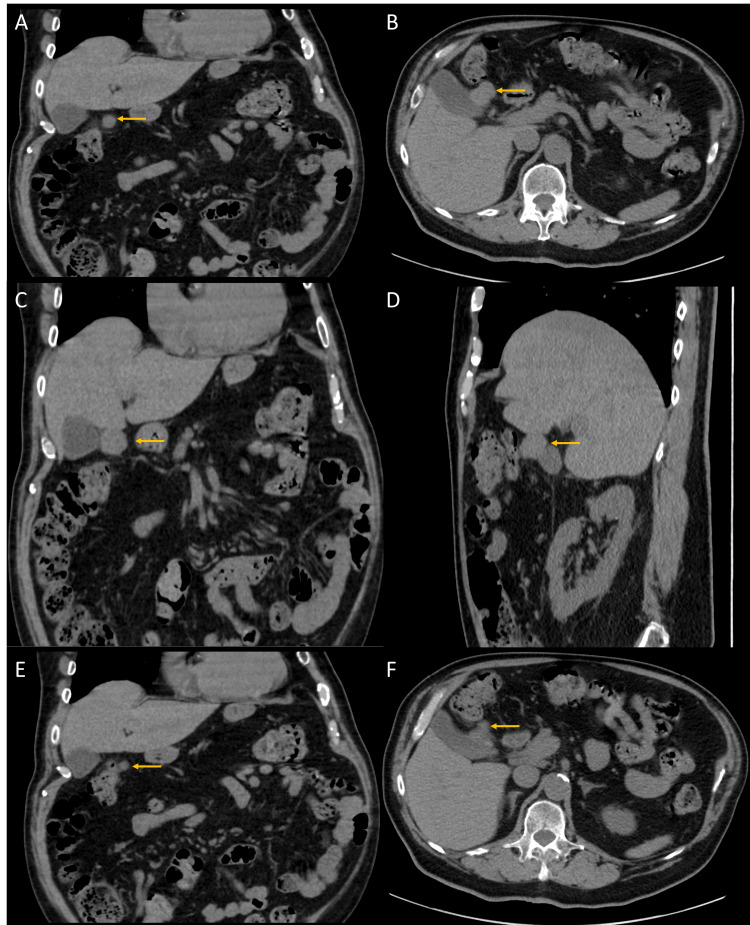 Figure 1
Figure 1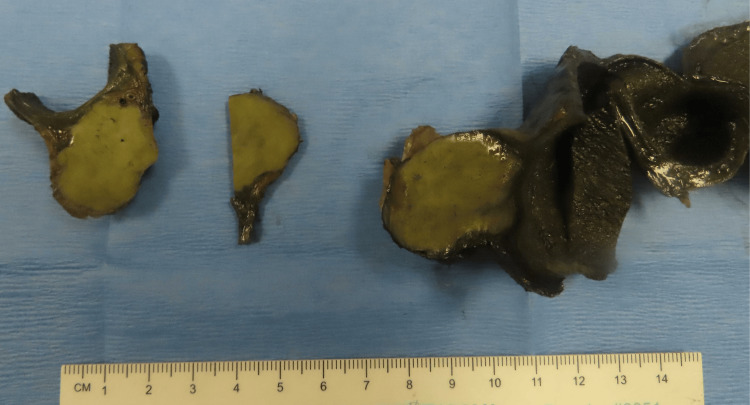 Figure 2
Figure 2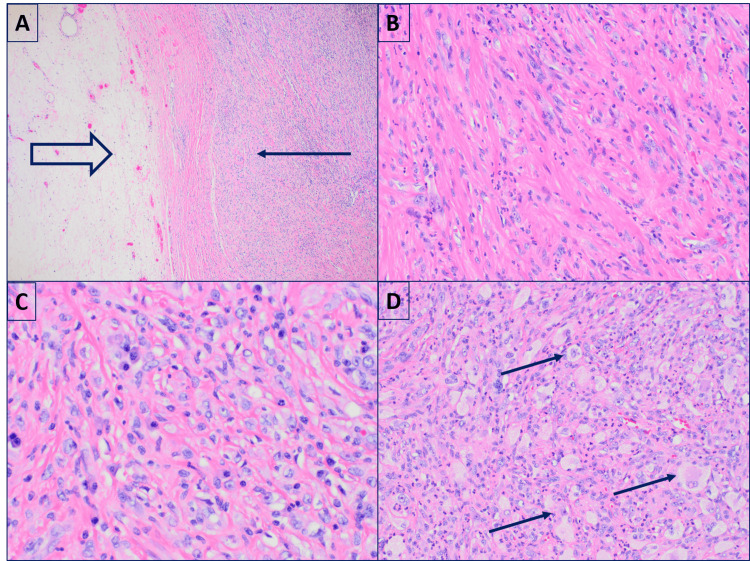 Figure 3
Figure 3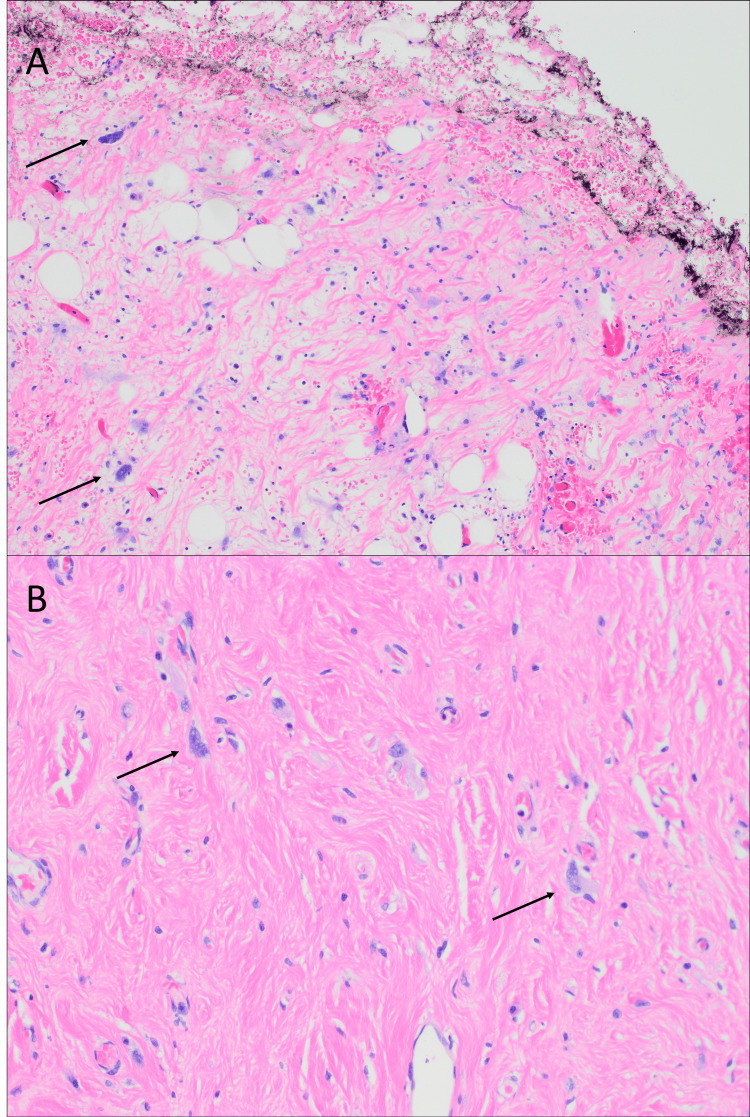 Figure 4
Figure 4| Year | Author | Age | Sex | Diagnosis | Gross findings | Intervention | Follow-up* |
| 1983 | Bader et al. [ | 79 | N/A | MLPS | Intramural mass | Cholecystectomy | DOD (2 years) |
| 2006 | Hamada et al. [ | 49 | F | PLPS | Encapsulated focally; infiltrative 25 x 23 cm | GB and tumor resection | Recurrence (10 and 29 months). Alive (3.5 years)** |
| 2009 | Husain et al. [ | 64 | F | Liposarcoma | 1.7 cm | N/A | DOD |
| 2009 | Husain et al. [ | 70 | F | Liposarcoma | 3.0 cm | N/A | DOUC |
| 2014 | Ma et al. [ | 70 | F | MLPS | Circumscribed fatty mass 13 x 8 cm | Cholecystectomy | N/A |
| 2018 | da Costa et al. [ | 71 | F | DDLPS | 14 cm | GB and tumor resection, partial hepatectomy | Alive (8 months) |
| 2020 | Cheng et al. [ | 83 | M | DDLPS | 6.0 cm | Cholecystectomy and partial hepatectomy | Alive (4 years) |
| 2021 | Ushida et al. [ | 53 | M | Metastatic MLPS | 4 cm in the submucosa | Laparoscopic cholecystectomy | N/A |
| 2023 | Zou et al. [ | 48 | F | DDLPS | GB wall mass 5 x 5 x 4.5 cm 2nd mass measuring 7 x 6 x 5 cm near liver capsule | Cholecystectomy and hepatectomy | Alive (2 years) |
| 2024 | Chen et al. [ | 32 | F | Inflammatory WDLPS | Mass on the body, 5.5 x 5 x 3 cm | Radical resection | Alive (7 months) |
| 2024 | Wang et al. [ | 64 | F | DDLPS | Mass on the body, 13 x 9 x 7 cm | GB and tumor resection | Alive (15 months) |
| 2025 | Yang et al. [ | 35 | F | WDLPS | Nodular mass 30 x 24 x 8 cm | GB and mass en bloc resection | N/A |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Bone Tumor Diagnosis and Treatments · Cholangiocarcinoma and Gallbladder Cancer Studies
Introduction
Dedifferentiated liposarcoma (DDLPS) is a malignant soft tissue neoplasm characterized by a nonlipogenic sarcomatous component adjacent to areas of well-differentiated liposarcoma (WDLPS). It accounts for approximately 20% of all liposarcomas and typically affects middle-aged to older adults, with no significant gender predilection [1-3]. DDLPS most frequently arises in the retroperitoneum, deep soft tissues of the extremities, and paratesticular region. Clinically, it follows an aggressive course, with a local recurrence rate of approximately 40% and a metastatic rate ranging from 15% to 30% [1-3].
Primary DDLPS of the gallbladder is exceedingly rare. Fewer than a dozen cases have been reported in the literature [4-14], with only four confirmed as DDLPS based on histologic features and/or demonstration of MDM2 gene amplification by fluorescence in situ hybridization (FISH) [8,9,11,13]. Owing to their rarity, gallbladder liposarcomas are rarely diagnosed preoperatively. Their nonspecific clinical presentation and imaging findings pose considerable diagnostic challenges. Nevertheless, accurate preoperative diagnosis is essential, as liposarcomas typically require complete surgical resection with negative macroscopic margins [1-3].
Most reported gallbladder liposarcomas present as large, symptomatic abdominal masses. Herein, we describe a rare case of asymptomatic gallbladder DDLPS, incidentally identified during surveillance abdominal computed tomography (CT) in a patient with a history of low-grade papillary urothelial carcinoma of the bladder. This case adds to the limited literature and highlights the importance of considering liposarcoma in the differential diagnosis of gallbladder masses.
Case presentation
A 79-year-old man with a history of low-grade noninvasive papillary urothelial carcinoma of the bladder underwent routine surveillance imaging. A contrast-enhanced CT scan of the abdomen and pelvis identified a 3.1 × 2.2 cm exophytic soft tissue mass arising from the gallbladder wall (Figures 1A-1D). A retrospective review of imaging from 2023 revealed that the lesion had previously measured 1.0 × 0.8 cm, indicating interval growth (Figures 1E-1F).
(A-D) Coronal and axial CT images demonstrate a loculated soft tissue mass arising epiphytically from the gallbladder wall and extending into the peritoneum (arrows in A and B). The fat plane between the mass and the inferior margin of the liver is obliterated in both coronal and sagittal views (C and D). (E–F) The mass has increased in size compared to the prior CT scan performed two years ago (arrows)
Diffuse mural thickening of the gallbladder was also noted. Based on the imaging findings, the lesion was initially suspected to represent a primary gallbladder carcinoma. The fat plane between the mass and the inferior margin of the liver was obliterated, raising concern for possible hepatic invasion.
The patient was asymptomatic at the time of diagnosis. His past medical history included type 2 diabetes mellitus, hypertension, and transient ischemic attacks. He had no history of prior radiation exposure. Physical examination was unremarkable. Laboratory testing revealed hypoalbuminemia and mild anemia; liver function tests and tumor markers, including carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9), were within normal limits.
The patient underwent cholecystectomy with portal lymphadenectomy. Intraoperatively, a firm, well-defined mass was palpated at the neck of the gallbladder without overt invasion into the adjacent liver. Gross examination revealed a gallbladder measuring 9.5 cm in length and 4.7 cm in maximum diameter. A yellowish-tan, indurated mass measuring 3.1 × 2.6 × 2.4 cm was located within the adventitia at the gallbladder neck (Figure 2).
Gross image showing a yellowish-tan, indurated mass located in the adventitia at the gallbladder neck
The cut surface of the mass was slightly whorled. The tumor extended to the muscularis propria and abutted the serosal surface but did not reach the hepatic bed or cystic duct margin. The gallbladder wall thickness ranged from 0.2 to 0.5 cm, and the mucosal surface appeared grossly unremarkable. No gallstones were identified.
Microscopic examination of the mass revealed a high-grade malignant neoplasm composed of spindle cells, epithelioid cells, and occasional multinucleated tumor cells in a background of prominent inflammation (Figures 3A-3C). Additional foci demonstrated solid sheets of histiocyte-like pleomorphic cells (Figure 3D).
Histologic sections of the nodule reveal a high-grade sarcoma sharply demarcated from the lipomatous component(A) Low-power view (x40) showing separation between the high-grade sarcoma (thin arrow) and the lipomatous component (thick arrow). (B) Spindle cells (x200). (C) Epithelioid/round cells (x200). (D) Histiocyte-like cells (x200), all within a prominent inflammatory stroma
Adjacent sections showed WDLPS involving the adventitia, with atypical hyperchromatic stromal cells in adipose tissue, fibrous septa, and sclerosing stroma accompanied by chronic inflammation (Figures 4A-4B).
Sections of well-differentiated liposarcoma (WDLPS)(A) Large atypical stromal cells (arrow) in fibrous septa, extending to the inked liver bed resection margin (x200). (B) Sclerosing stroma (x200)
Immunohistochemically, the tumor cells were diffusely positive for p16 and negative for pancytokeratin, S100, SOX10, CD34, smooth muscle actin (SMA), desmin, epithelial membrane antigen (EMA), anaplastic lymphoma kinase (ALK), CD68, CD117, and DOG1. FISH testing demonstrated MDM2 gene amplification, supporting a final diagnosis of DDLPS. While the liver bed resection margin was free of high-grade dedifferentiated component, it was involved by the WDLPS component.
The case was discussed at a multidisciplinary tumor board. Given the patient's advanced age, comorbidities, absence of residual high-grade tumor, lack of evidence supporting postoperative radiotherapy, and the potentially high risk of side effects and complications from such treatment, particularly given the low likelihood of meaningful benefit in reducing local recurrence or improving local control, no further surgical or adjuvant therapy was recommended.
Discussion
Primary liposarcoma of the gallbladder is exceedingly rare, with only 12 cases reported in the literature to date (Table 1) [4-14].
Among these, one patient with gallbladder myxoid liposarcoma (MLPS) had a prior history of a similar tumor in the leg, raising suspicion of metastasis rather than a primary lesion [10]. Most reported cases originated in Asia, with five from China [9,11-14] and two from Japan [5,10]. Patients ranged in age from 32 to 83 years (mean: 60 years), and a strong female predominance was observed (female-to-male ratio of 8:4). The most common presentation was an abdominal mass [5,6,8,9,12-14], while other symptoms included abdominal pain, fever, and dyspepsia. Notably, jaundice was absent in all cases. Laboratory findings were generally nonspecific, although anemia, leukocytosis, elevated C-reactive protein (CRP), and liver enzyme abnormalities were occasionally reported [5,12,14]. Tumor size ranged from 1.7 to 25 cm, with growth patterns variably described as infiltrative [5,8,11,13] or well-circumscribed [7,10,12,14].
Among the 11 confirmed primary gallbladder liposarcomas, four were diagnosed as DDLPS [8,9,11,13], two as WDLPS [12,14], two as MLPS [4,7], one as pleomorphic liposarcoma (PLPS) [5], and two as liposarcoma not otherwise specified [6]. These encompass all four major histologic subtypes recognized by the WHO Classification of Tumours of Soft Tissue and Bone [2]. DDLPS and WDLPS, characterized by MDM2 gene amplification, form a biologic continuum [1,2] and typically arise in the retroperitoneum, extremities, and paratesticular regions, though rare visceral involvement, including the gallbladder, has been documented [15]. In contrast, MLPS and PLPS generally occur in the extremities and are infrequent in the retroperitoneum or intra-abdominal sites [1-3,15].
Radiologically, DDLPS is often suggested by the presence of both soft tissue mass and abnormal fat density or distribution on CT or MRI [16,17]. WDLPS areas may present as heterogeneous fatty regions with thick septa and nodularity, while dedifferentiated regions appear as solid masses with necrosis or hemorrhage [16,17]. In two of the four previously reported gallbladder DDLPS cases, fat-containing regions were observed [8,9]. In the present case, only the dedifferentiated component was evident radiologically and on gross examination, and the WDLPS component was not initially recognized due to the unexpected location.
Grossly, DDLPS typically demonstrates a sharp transition between WDLPS and the nonlipogenic sarcoma, with the latter showing a fleshy, firm, or variegated appearance, occasionally with hemorrhage or necrosis [1-3,15]. Histologically, the WDLPS component is typified by hyperchromatic stromal cells within the fibrous septa of mature adipose tissue. Sclerosing and inflammatory variants are also recognized [1-3,15]. The dedifferentiated component displays high-grade sarcoma morphology with broad heterogeneity, including spindle cell, pleomorphic, and inflammatory MFH-like patterns. Rarely, heterologous elements such as bone, cartilage, or muscle may be present. Homologous lipogenic differentiation, including the presence of lipoblasts, may also be observed. In cases with extensive myxoid change, DDLPS can closely mimic MLPS [1-3,15]. When WDLPS is absent or overlooked, particularly in unusual anatomical sites, diagnosis may be challenging.
Immunohistochemistry can assist, with both WDLPS and DDLPS often showing positivity for MDM2, CDK4, and p16; however, demonstration of MDM2 gene amplification by FISH or polymerase chain reaction (PCR) remains the gold standard for diagnosis [18]. This distinction is critical in differentiating DDLPS from mimics such as MLPS and PLPS. Of note, DDIT3 amplification, observed in one MLPS case, is not specific and may also occur in DDLPS. Only DDIT3 gene rearrangement confirms MLPS [19,20].
Treatment for gallbladder liposarcoma has primarily involved surgical resection. Most patients underwent wide excision, with or without partial hepatectomy. One early case treated with cholecystectomy alone died from widespread recurrence [4]. Another, with incomplete follow-up data, also underwent cholecystectomy only [7]. While one patient who received chemotherapy died of the disease [6] and one experienced multiple recurrences [5], most remained disease-free over follow-up periods ranging from seven months to four years. None received adjuvant radiation therapy.
In our case, liposarcoma was not included in the preoperative differential, and resection was limited to the CT-detected mass. Histologic examination revealed high-grade sarcoma and additional sampling disclosed adjacent WDLPS infiltrating the gallbladder adventitia, resulting in a positive surgical margin at the liver bed.
Conclusions
Given the rarity of gallbladder DDLPS, accurate diagnosis can be challenging, especially when the tumor arises in an unexpected location or when only the high-grade component is initially evident. This case highlights the importance of thorough radiologic assessment, with special attention to areas of abnormal fat, as well as detailed gross and histologic examination. Extensive sampling and the use of ancillary molecular techniques, particularly FISH for MDM2 amplification, are critical for establishing the correct diagnosis. A multidisciplinary approach involving radiology, surgery, pathology, and oncology is essential for optimal management. Due to the limited number of reported cases, the long-term prognosis remains uncertain, emphasizing the need for careful postoperative surveillance and reporting of additional cases to inform clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Well-differentiated liposarcoma and dedifferentiated liposarcoma: an updated review Semin Diagn Pathol Thway K 1121213620193085204510.1053/j.semdp.2019.02.006 · doi ↗ · pubmed ↗
- 2WHO Classification of Tumours of Soft Tissue and Bone The WHO Classification of Tumors Editorial Board 3646 Lyon, France IARC Presspp.2020 https://publications.iarc.who.int/Book-And-Report-Series/Who-Classification-Of-Tumours/Soft-Tissue-And-Bone-Tumours-2020
- 3Biology and management of dedifferentiated liposarcoma: state of the art and perspectives J Clin Med Nishio J Nakayama S Nabeshima K Yamamoto T 32301020213436201310.3390/jcm 10153230 PMC 8348700 · doi ↗ · pubmed ↗
- 4Liposarcoma of the gallbladder and the peritoneum. A case report (Article in German)Zentralbl Allg Pathol Bader H Vallon H 45491271983 https://pubmed.ncbi.nlm.nih.gov/6858427/6858427 · pubmed ↗
- 5Primary liposarcoma of gallbladder diagnosed by preoperative imagings: a case report and review of literature World J Gastroenterol Hamada T Yamagiwa K Okanami Y 147214751220061655282410.3748/wjg.v 12.i 9.1472 PMC 4124333 · doi ↗ · pubmed ↗
- 6Gallbladder sarcoma: a clinicopathological study of seven cases from the UK and Austria with emphasis on morphological subtypes Dig Dis Sci Husain EA Prescott RJ Haider SA Al-Mahmoud RW Zelger BG Zelger B Al-Daraji WI 3954005420091861825810.1007/s 10620-008-0358-z · doi ↗ · pubmed ↗
- 7An extremely rare primary gallbladder myxoid liposarcoma associated with amplification of DDIT 3 gene J Gastrointestin Liver Dis Ma Y Wei S Peker D 460461232014 https://europepmc.org/article/med/2553201125532011 · pubmed ↗
- 8Dedifferentiated liposarcoma of the gallbladder: first reported case World J Surg Oncol da Costa AC Santa-Cruz F Sena BF 2211620183041991510.1186/s 12957-018-1520-5PMC 6233360 · doi ↗ · pubmed ↗