Pneumorrhachis in Acute Asthma Exacerbation in an 18-Year-Old Female Patient: A Report of a Rare Case
Omar Abdelaziz, Hashim Abid, Ado Yusuf, Nickh Uppal

TL;DR
A rare case of pneumorrhachis caused by severe asthma in an 18-year-old woman is reported, showing it can occur without trauma and resolve with conservative treatment.
Contribution
This paper adds a rare non-traumatic case of pneumorrhachis caused by asthma exacerbation to the limited clinical literature.
Findings
Pneumorrhachis occurred alongside pneumomediastinum in a patient with severe asthma exacerbation.
Conservative treatment resolved symptoms and radiographic abnormalities without neurological complications.
The case highlights the importance of recognizing pneumorrhachis in asthma exacerbations without trauma.
Abstract
Pneumorrhachis (intraspinal air) is a rare radiological finding, often associated with trauma, iatrogenic causes, or increased intrathoracic pressures. We present a case of pneumorrhachis secondary to severe asthma exacerbation, highlighting its pathophysiology and clinical implications. An 18-year-old female patient presented with a history of dry cough, chest tightness, and pain in her neck. Subsequent scans, including chest X-rays and computed tomography (CT) scans, showed a large volume pneumomediastinum and pneumorrhachis. The patient was managed conservatively with bronchodilators, corticosteroids, and supplemental oxygen, leading to the resolution of symptoms and radiographic abnormalities. This case illustrates that pneumorrhachis can occur in asthma due to increased intrathoracic pressure, leading to air dissection into the spinal canal. Conservative management suffices in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
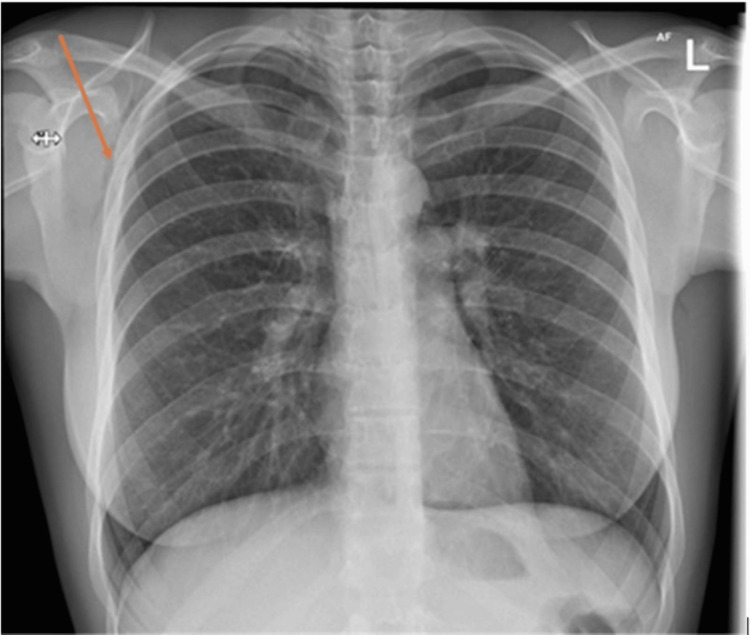 Figure 1
Figure 1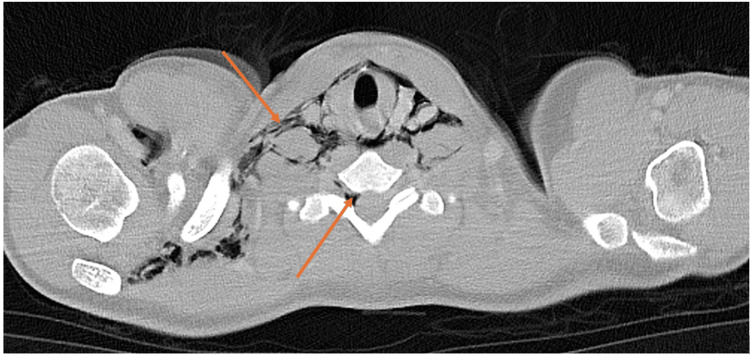 Figure 2
Figure 2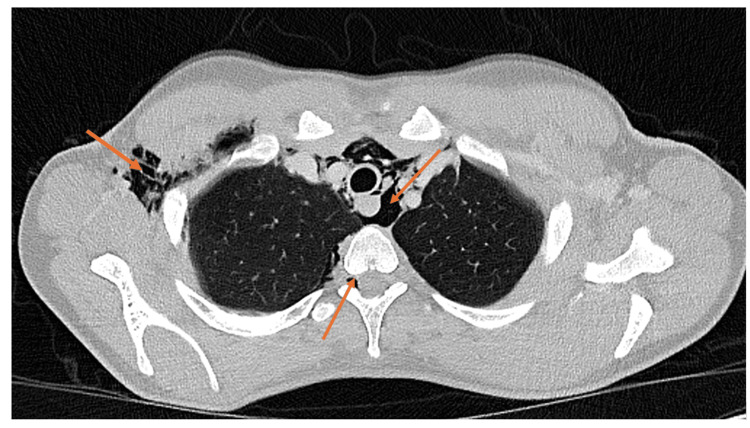 Figure 3
Figure 3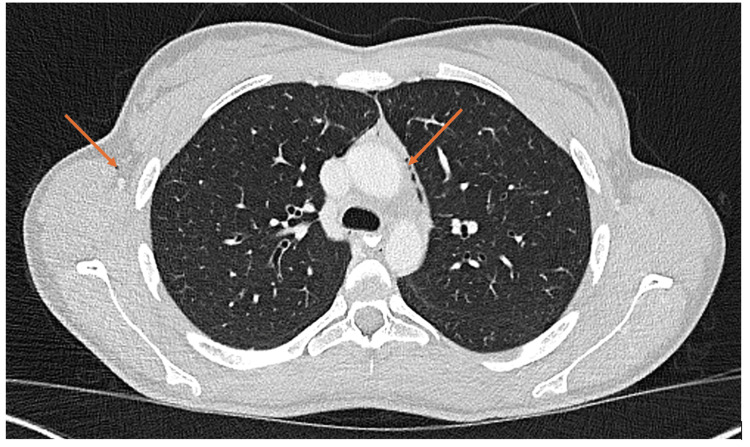 Figure 4
Figure 4| Test | Result | Normal value |
| White blood cell (WBC) count | 13.3 x 109/L | 4.0-11.0 x 109/L |
| Neutrophils | 9.82 x 109/L | 1.80-7.50 x 109/L |
| Eosinophils | 0.33 x 109/L | 0.00-0.40 x 109/L |
| Potassium | 3.3 mmol/L | 3.5-5.0 mmol/L |
| Sodium | 141 mmol/L | 135-145 mmol/L |
| C-reactive protein (CRP) | 58 | <1 |
| Magnesium | 0.92 mmol/L | 0.7-1.0 mmol/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPneumothorax, Barotrauma, Emphysema · Foreign Body Medical Cases · Pleural and Pulmonary Diseases
Introduction
Pneumorrhachis (PR), the presence of intraspinal air, is an exceptional but eminent radiographic finding, accompanied by different etiologies and possible pathways of air entry into the spinal canal [1]. In the absence of trauma or iatrogenic causes, spontaneous PR has been reported secondary to respiratory tract infection, abdominal infections, asthma, vomiting, and acute cough and is usually preceded by pneumomediastinum [2]. An acute increase in the intra-alveolar pressure leads to rupture of alveoli resulting in air escape into the perivascular space. This air further moves through the facial planes into the posterior mediastinum and thus into the epidural space [3]. Spontaneous PR is extremely rare, and only a few cases have been reported in the literature [1]. There are no guidelines for the management of PR. Treatment of the inciting etiology, such as bronchodilators and oxygen supplementation for asthma exacerbation, abscess drainage, chest tube for pneumothorax, etc., is required [4].
Case presentation
An 18-year-old female patient presented to the emergency department (ED) of a district general hospital with a dry cough and chest tightness. She also complained of pain overlying her right shoulder, jaw, and neck, which was exacerbated by deep breaths and swallowing.
This was initially managed as an acute severe exacerbation of asthma. The patient had a past medical history of childhood asthma that was diagnosed at the age of three but without acute exacerbations for several years. She had not utilized inhalers for four years preceding the presentation due to being asymptomatic. Social history comprised a smoking history of three years, alongside cannabis use.
On examination, chest auscultation revealed diffuse bilateral wheeze and palpable subcutaneous emphysema at the right base of the neck. Investigations showed a mild increase in inflammation markers (Table 1).
A chest X-ray was performed (Figure 1), which showed streaking linear lucencies overlying the superior mediastinum and surgical emphysema in the right axilla.
X-ray showing streaking linear lucencies overlying the superior mediastinum and surgical emphysema in the right axilla
Computed tomography (CT) thorax-abdomen with oral and intravenous contrast was performed to rule out an esophageal rupture (Figures 2, 3). This confirmed large volume pneumomediastinum with extensive surgical emphysema of the neck and right axilla/chest wall. Air was seen tracking into the spinal canal via the right intervertebral foramen from the deep neck fascia in the lower cervical spine, causing PR. There was a small left pneumothorax within the left oblique fissure and anteriorly. No evidence of esophageal perforation was observed. In addition to initial management for asthma exacerbation, the case was discussed with cardiothoracic surgery, who advised that as the lung was fully expanded, there was no current indication for chest drain, opting instead for conservative management with monitoring and oxygen.
CT showing large volume pneumomediastinum with extensive surgical emphysema of the neck and right axilla/chest wallCT: computed tomography
CT scan showing large volume pneumomediastinum with extensive surgical emphysema of the neck and right axilla/chest wallCT: computed tomography
At this point, the diagnosis was revised to non-traumatic spontaneous pneumomediastinum secondary to bronchial asthma. Following a review by respiratory physicians, the management consisted of regular nebulizers and steroids, oxygen supplementation with 2 L via nasal cannula, and adequate analgesia. A neurological examination was also done, which was normal.
A repeat chest X-ray was performed the day after admission due to ongoing pain, which showed a larger volume and worsening of the pneumomediastinum. Further discussion with cardiothoracic surgery was performed, who advised that there was no indication for acute surgical intervention. The case was also discussed with neurosurgery, who confirmed that no neurosurgical intervention was indicated and advised to avoid strenuous activities. Gastroenterology also advised that there was no indication for esophagogastroduodenoscopy (EGD).
CT thorax-abdomen was done on the fifth day of admission (Figure 4), which showed interval resolution of the pneumothoraces and volume reduction of the surgical emphysema and pneumomediastinum.
CT showing resolution of pneumorrhachis and pneumomediastinumCT: computed tomography
Following a period of supportive management and monitoring, the symptoms as described above improved. The patient was discharged after six days as an inpatient, with follow-up organized with the respiratory pleural team as an outpatient.
She was seen in the pleural clinic a week after her discharge, with a repeat chest X-ray demonstrating normal appearances without evidence of subcutaneous emphysema, pneumothorax, or pneumomediastinum. In order to optimize her asthma control, inhaled therapy was initiated alongside a referral to the asthma team. She was discharged from the pleural clinic.
Discussion
Pathophysiology of PR in asthma
PR is typically caused by the introduction of air into the spinal canal through various mechanisms, including trauma, iatrogenic causes, or increased intrathoracic pressure [1]. In asthma exacerbations, the forceful coughing and bronchospasm associated with severe airflow obstruction can lead to alveolar rupture, resulting in pneumomediastinum [5]. Air can also dissect in the retropharyngeal and retroperitoneal space causing discomfort and respiratory compromise. In rare situations, air can dissect between the mediastinum and the upper spine causing PR [6]. This mechanism aligns with the findings in our patient, who presented with severe coughing episodes preceding the identification of PR.
Diagnostic considerations
CT is considered to be the diagnostic modality of choice, with a sensitivity of 100% [7]. In our case, the patient’s CT scan revealed air within the spinal canal, confirming the diagnosis. Importantly, PR is often asymptomatic, as seen in this patient, but it can occasionally present with neurological symptoms such as radiculopathy or myelopathy if the air compresses neural structures. The absence of neurological deficits in this case underscores the importance of considering PR even in asymptomatic patients with predisposing conditions.
Clinical significance and management
The identification of PR in asthma exacerbations highlights the potential complications of increased intrathoracic pressure in severe asthma. While PR itself is often benign and self-limiting, its presence should prompt clinicians to evaluate for other complications of barotrauma, such as pneumothorax or pneumomediastinum [8]. In this case, the patient’s pneumomediastinum resolved with conservative management, including bronchodilators, corticosteroids, and oxygen therapy. High‐concentration oxygen therapy may be considered, as it may promote re‐absorption of gas into soft tissue in subcutaneous emphysema, pneumomediastinum, and presumably PR [6].
Uniqueness of the case
This case is noteworthy due to the rarity of PR in asthma exacerbation and the absence of neurological symptoms despite the presence of intraspinal air. Spontaneous pneumomediastinum is an uncommon entity primarily affecting young adults and children. There have been only a few case reports of PR associated with spontaneous pneumomediastinum [9].
Gupta et al. [10] described a rare case of spontaneous giant PR with symptoms that included back pain and deteriorating mobility, managed surgically with laminectomy without fusion. Gibikote et al. [9] described an even rarer case of PR in the pediatric population: a four-year-old boy with a traumatic case of PR that resolved spontaneously. Extensive extradural PR was also described by Garcia-Cebrián et al. [11], with the cause being related to obstetric analgesia. Poovazhagi et al. [12] present the case of a seven-year-old girl with accidental injury, presenting with emphysema, pneumomediastinum, pneumothorax, pneumoperitoneum, and PR. Fantacci et al. [13] reported a case of respiratory syncytial virus associated with PR, requiring rapid recognition and management.
These cases highlight the fact that the causes of PR are many, and while it may be complicated by various conditions and associated with neurological symptoms such as meningeal irritation, extremity weakness, and cauda equina syndrome, it may also present in the asymptomatic patient. These learning points are further impressed in the report as described by ourselves, where careful consideration of differentials as well as extensive follow-up was essential.
Implications for clinical practice
As with other rare conditions, there are no published guidelines for the ED management of PR, necessitating the use of case presentations to educate providers as to the complications and plan of care of this diagnosis [14]. Early recognition and appropriate management of the underlying asthma are crucial to prevent further complications. Additionally, this case underscores the value of CT imaging in diagnosing PR and ruling out other potential causes of air leakage.
Conclusions
In summary, PR is a rare but important complication of asthma exacerbation that can occur due to increased intrathoracic pressure and air dissection into the spinal canal. This case underscores the importance of considering atypical complications in asthma exacerbations and the need for vigilant monitoring and appropriate imaging to guide management. It also adds to the limited literature on PR in asthma and emphasizes the importance of considering and prompt management of this diagnosis in patients with severe respiratory distress.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pathogenesis, diagnosis and management of pneumorrhachis Eur Spine J Oertel MF Korinth MC Reinges MH Krings T Terbeck S Gilsbach JM 6366431520061683573510.1007/s 00586-006-0160-6PMC 1602196 · doi ↗ · pubmed ↗
- 2Pneumorrhachis secondary to exacerbation of asthma: a case report and literature review Respirol Case Rep Zhao CZ Poci N Niewodowski D Baker A Mc Donald C 122811202310.1002/rcr 2.1228 PMC 1056260937822866 · doi ↗ · pubmed ↗
- 3Pneumorrhachis, pneumomediastinum, pneumopericardium and subcutaneous emphysema as complications of bronchial asthma Ann Thorac Med Manden PK Siddiqui AH 143145420091964164710.4103/1817-1737.53352 PMC 2714570 · doi ↗ · pubmed ↗
- 4Spontaneous pneumorachis - a case-based review J Asthma Allergy Alampoondi Venkataramanan SV George L Sahu KK 153915541420213495564210.2147/JAA.S 325293 PMC 8694274 · doi ↗ · pubmed ↗
- 5Subcutaneous and mediastinal emphysema. Pathophysiology, diagnosis, and management Arch Intern Med Maunder RJ Pierson DJ Hudson LD 144714531441984 https://pubmed.ncbi.nlm.nih.gov/6375617/6375617 · pubmed ↗
- 6Pneumomediastinum J Thorac Dis Kouritas VK Papagiannopoulos K Lazaridis G 44497201510.3978/j.issn.2072-1439.2015.01.11PMC 433208325774307 · doi ↗ · pubmed ↗
- 7Narrative review of traumatic pneumorrhachis World J Crit Care Med Pothiawala S Civil I 2482531220233818845210.5492/wjccm.v 12.i 5.248PMC 10768418 · doi ↗ · pubmed ↗
- 8The Macklin effect: a frequent etiology for pneumomediastinum in severe blunt chest trauma Chest Wintermark M Schnyder P 54354712020011150265610.1378/chest.120.2.543 · doi ↗ · pubmed ↗