Case Report: A novel KRT74 variant in an eight-year-old boy with alopecia totalis successfully treated with baricitinib
Yidong Tan, Jinxiang Yang, Xuanyi Chen, Yihang Shen, Zhe Wu, Weinan Zhou, Zhirong Yao, Jingjun Zhao, Jianying Liang

TL;DR
An 8-year-old boy with alopecia totalis and a KRT74 gene variant showed significant hair regrowth after treatment with baricitinib.
Contribution
A novel KRT74 variant is linked to alopecia areata, and JAK inhibitors may be effective in genetically predisposed cases.
Findings
The patient showed significant hair regrowth within one month of baricitinib treatment.
Immunofluorescence revealed increased JAK1-STAT1 phosphorylation and CD4+ T cell infiltration in the scalp.
The KRT74 variant was present in family members without alopecia, suggesting a genetic predisposition.
Abstract
Alopecia areata is an autoimmune condition characterized by non-scarring hair loss, with genetic factors playing a significant role in disease susceptibility. We report the case of an 8-year-old boy with alopecia totalis harboring a heterozygous KRT74 variant. While his mother and brother share this variant, they do not exhibit alopecia. Immunofluorescence analysis revealed increased phosphorylation of the JAK1-STAT1 pathway and elevated T cell infiltration, predominantly CD4+ T helper cells, in the proband’s scalp. The patient responded favorably to baricitinib treatment (2 mg/day), showing significant hair regrowth within 1 month and continued improvement over 8 months. This case suggests that KRT74 variants may contribute to immune dysregulation in alopecia areata, highlighting the potential role of JAK inhibitors in genetically predisposed alopecia cases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
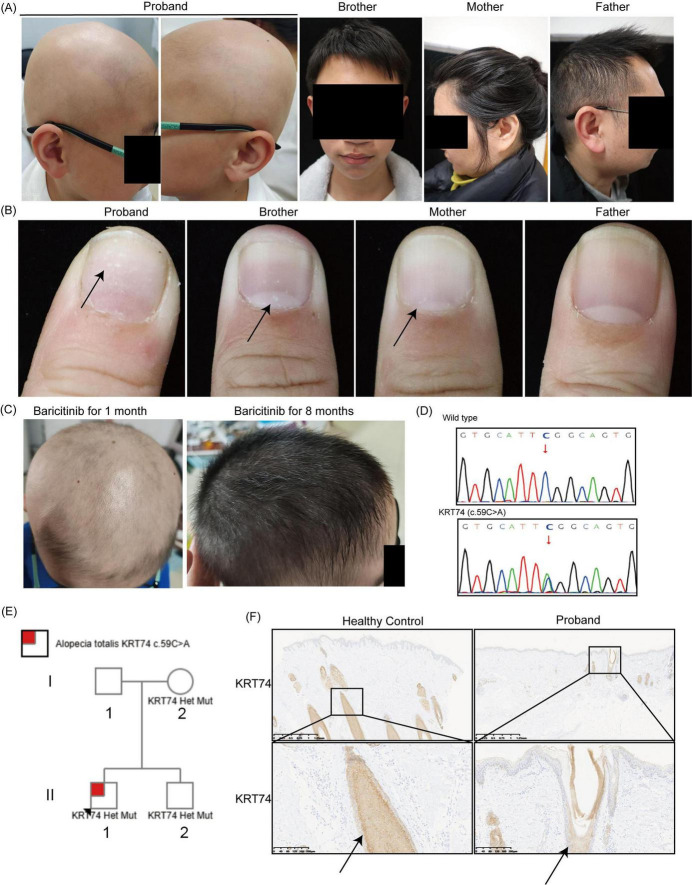 FIGURE 1
FIGURE 1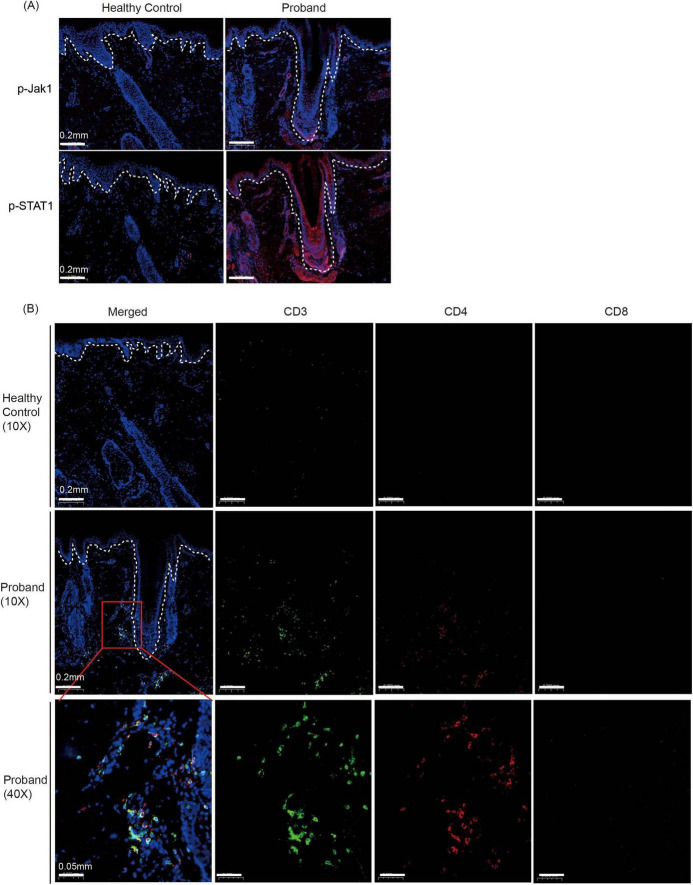 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHair Growth and Disorders · Autoimmune Bullous Skin Diseases · Dermatology and Skin Diseases
Introduction
Alopecia areata is an autoimmune condition leading to non-scaring hair loss (1), with an estimated lifetime prevalence of approximately 2% (2). Clinically, alopecia areata presents in various forms, ranging from well-defined patches (patchy alopecia areata) to complete hair loss on the scalp (alopecia totalis), or loss of all body hair (alopecia universalis). Genetic factors significantly contribute to alopecia areata susceptibility (3, 4). In children, the prevalence of child patients with a family history is estimated to be between 10% and 51.6% (3, 5). Large-scale genetic studies have identified several genes associated with alopecia area, including those encoding keratins.
Keratins are the most abundant structural protein in keratinocytes and contribute to form keratin intermediate filaments (KIFs) through heterodimerization between type I (acidic) and type II (basic to neutral) keratins (6). Beyond maintaining skin integrity, keratins are involved in regulating immune responses and hair growth (7). Pathological variant in keratin genes, such as KRT71 (6) and KRT74 (8), have been linked to hereditary hair disorders. KRT74 is expressed in the inner root sheath of human hair follicle and heterozygous variants in KRT74 cause the autosomal-dominant wooly hair (ADWH), affecting hair texture (8). We present a case of an 8-year-old boy with a heterozygous KRT74 variant who developed alopecia totalis. The patient responded favorably to baricitinib treatment, marking the first reported instance of a KRT74-mutated patient with hair loss treated with baricitinib.
Case presentation
An 8-year-old boy presented with a 7-month history of alopecia totalis. Hair loss began 1 year prior, progressing to complete scalp hair loss within 5 months (Figure 1A). Initial treatments with vitamin B6 and glutamic acid supplements were ineffective in local hospital. Given the strong association between alopecia and genetic variants, particularly in pediatric cases (3), whole exome sequencing (WES) was performed, revealing a heterozygous KRT74 variant (c.59C > A) (Figure 1D). Immunohistochemical analysis demonstrated downregulated expression of KRT74 in the patient’s hair follicle compared to a healthy control (Figure 1F). Pedigree analysis identified the same KRT74 variant in the proband’s mother and brother (Figure 1E); however, neither exhibited alopecia (Figure 1A). The proband had normal eyebrows, eyelashes, sweating, and teeth with no signs of palmoplantar hyperkeratosis or keratosis pilaris. Notably, the patient exhibited leukonychia (white spots on nails), a feature also observed in his mother and brother, which has not been previously associated with KRT74 variants (8, 9) (Figure 1B).
Clinical, genetic, and histopathological features of the proband and family members. (A) Clinical photographs of the proband, his brother, mother, and father. The proband exhibits alopecia totalis, while the other family members show normal hair growth. (B) Leukonychia (white spots on nails) in the nail of the proband, his brother, and mother, but not in the father. Arrows indicate the leukonychia. (C) Scalp images of the proband after treatment with baricitinib (2 mg/day), showing significant hair regrowth after 1 month and continued improvement after 8 months. (D) Sanger sequencing results identifying a heterozygous c.59C > A variant in the Keratin 74 (KRT74) gene. (E) Pedigree analysis of the family. (F) Immunohistochemical staining of scalp tissue showing reduced KRT74 expression in the proband’s hair follicles compared to a healthy control. Arrows indicate the expression of KRT74 in the hair follicle. Magnifications: 2× and 10×.
Recent researches have demonstrated that alopecia is a disease that happens when the immune system attacks hair follicle and cause hair loss (10). Immunosuppressive treatments, such as baricitinib (11), dupilumab (12) and ritlecitinib (13) have proven effective. Variants in keratin genes can affect the immune homeostasis of keratinocyte (7). We hypothesized that the KRT74 variant might similarly affect the patient’s immune response. Using immunofluorescence, we analyzed the phosphorylation of Janus kinase (JAK) and STAT signaling pathway. The JAK1-STAT1 signaling is known to be activated in alopecia, and targeting the pathway has proved to be effective (14). We found the increased phosphorylation of JAK1 and STAT1 in the proband (Figure 2A). T cells are regarded as the primary effector cells in the pathogenesis of alopecia, particularly CD8^+^ cytotoxic T lymphocytes (15). To assess immune infiltration in the proband, we performed immunofluorescence staining for CD3, CD4, and CD8 markers. Our analysis revealed an increased presence of T cells (CD3^+^) in the proband. Interestingly, T helper cells (CD3^+^ CD4^+^) constituted the majority of T cell population, while the frequency of CD8^+^ cytotoxic T cell was not elevated compared with healthy controls (Figure 2B).
Immunofluorescence analysis of JAK-STAT pathway activation and immune cell infiltration in the proband’s scalp tissue. (A) Immunofluorescence staining for phosphorylated JAK1 (p-JAK1) and phosphorylated STAT1 (p-STAT1) in scalp tissue from a healthy control and the proband. Dashed lines demarcate the epidermal-dermal junction. Magnifications: 10×. (B) Immunofluorescence staining for immune cell markers in scalp tissue from a healthy control and the proband. Sections were stained for CD3 (green, T cells), CD4 (red, T helper cells), and CD8 (pink, cytotoxic T cells). The merged images show increased T cell infiltration in the proband’s scalp, with a predominance of CD4 + T helper cells. Dashed lines demarcate the epidermal-dermal junction. Magnifications: 10× and 40×.
Given the increased JAK1 phosphorylation and the established efficacy of baricitinib in treating alopecia areata, the patient was initiated on baricitinib (2 mg/day). Significant hair regrowth was observed within 1 month (Figure 1C). Over an 8-months follow-up, the patient’s hair continued to thicken, indicating sustained treatment efficacy.
Discussion
Keratin 74 is a type II keratin protein predominantly expressed in the inner root sheath of hair follicles, playing a crucial role in hair structure and integrity (9). Previous research has demonstrated that variants in KRT74 are associated with autosomal dominant wooly hair and hypotrichosis (8). In our case study, we identified a heterozygous variant in KRT74 in an 8-years-old patient presenting with alopecia totalis, an immune-mediated disorder. The variant c.59C > A results in a nonsense mutation at codon 20 (p.Ser20*), introducing a premature stop codon in exon 1 of KRT74. To assess the potential pathogenicity of this variant, using MutationTaster,^1^ the variant was classified as “Disease Causing” with a prediction score of 6.0, strongly suggesting its pathogenicity. The absence of alopecia in the proband’s mother and brother, who share the same KRT74 variant, suggests potential incomplete penetrance or polygenic modulation of the phenotype. Our finding is particularly noteworthy as we observed activation of the JAK1-STAT1 pathway and T cell infiltration in the scalp of the patient with the KRT74 variant. This suggests that KRT74 may influence immune response of the scalp.
The exact mechanism by which KRT74 variants contribute to alopecia areata pathogenesis remains to be elucidated. It is plausible that alterations in keratin structure could disrupt the hair follicle’s immune privilege, rendering it more susceptible to autoimmune attacks. This concept is supported by studies on other keratin proteins; for instance, loss-of-function mutations in KRT32 lead to hyperactivation of NF-κB signaling and are implicated in the pathogenesis of pityriasis rubra pilaris, an inflammatory skin disorder (7). Given the structural and functional similarities among keratin proteins, it is conceivable that KRT74 variants may similarly influence immune regulatory pathways within hair follicles. Previous studies have suggested that self-reactive NKG2D^+^ CD8^+^ T cells and the activation of IFN-γ are key factors in the pathogenesis of alopecia areata (AA) (16, 17). However, recent studies have shown that CD4^+^ T cells may play a crucial role in the systemic Th1/Th2 inflammation and generalized phenotypes of AA patients (18–20). Our findings suggest that keratin mutations may preferentially activate CD4^+^ T cell-dependent pathways. We speculate that this could explain the clinical efficacy of JAK inhibitors (targeting signal transduction) observed in our cases. Further research is warranted to explore this potential connection and to determine whether KRT74 variants could serve as biomarkers for alopecia areata susceptibility or targets for therapeutic intervention.
In addition to alopecia totalis, our patient exhibited leukonychia, characterized by white patches on the nails. KRT74 expression has been detected in the nail matrix, nail bed, and hyponychium, suggesting a role in nail development (21). The presence of leukonychia in our patient, along with similar findings in his mother and brother who harbor the same KRT74 variant, suggests a potential association between this genetic alteration and nail pathology. This expands the phenotypic spectrum of KRT74-related disorders, which have primarily been associated with hair abnormalities. Further research is needed to elucidate the mechanisms by which KRT74 variants contribute to nail manifestations and to determine the prevalence of such features among affected individuals.
Baricitinib, an oral JAK inhibitor, has emerged as a promising treatment for inflammatory conditions, including severe alopecia areata (11). Notably, its application has extended to genetic disease such as Aicardi-Goutières syndrome (22) and refractory inflammatory skin disease (23). Although in China, there is no specific regulation or guideline regarding the dosage of baricitinib for treating pediatric alopecia areata, these instances underscore baricitinib’s potential beyond its initial indications and its success in such contexts suggests a broader applicability for JAK inhibitors in managing genetically driven inflammatory conditions.
Our findings should be interpreted cautiously. First, the KRT74 variant’s association with alopecia may reflect genetic susceptibility rather than direct causality, necessitating functional validation. Second, the lack of alopecia in family members underscores the potential role of gene-environment interactions, which were not systematically assessed here. Larger cohorts with longitudinal data are needed to clarify whether KRT74 variants represent a risk modifier in polygenic alopecia areata.
In conclusion, our findings suggest that KRT74 variants may play a role in the development of alopecia areata, highlighting the need for further studies to investigate this association. Elucidating the genetic underpinnings of alopecia areata can enhance our understanding of its pathophysiology and potentially lead to more effective, personalized therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Browne R Stewart L Williams H. Is methotrexate an effective and safe treatment for maintaining hair regrowth in people with alopecia totalis? A critically appraised topic. Br J Dermatol. (2018) 179:609–14. 10.1111/bjd.16796 29777625 · doi ↗ · pubmed ↗
- 2Gilhar A Etzioni A Paus R. Alopecia areata. N Engl J Med. (2012) 366:1515–25. 10.1056/NEJ Mra 1103442 22512484 · doi ↗ · pubmed ↗
- 3Pratt C King L Messenger A Christiano A Sundberg J. Alopecia areata. Nat Rev Dis Primers. (2017) 3:17011. 10.1038/nrdp.2017.11 28300084 PMC 5573125 · doi ↗ · pubmed ↗
- 4Martinez-Mir A Zlotogorski A Gordon D Petukhova L Mo J Gilliam T Genomewide scan for linkage reveals evidence of several susceptibility loci for alopecia areata. Am J Hum Genet. (2007) 80:316–28. 10.1086/511442 17236136 PMC 1785354 · doi ↗ · pubmed ↗
- 5Xiao F Yang S Liu J He P Yang J Cui Y The epidemiology of childhood alopecia areata in China: A study of 226 patients. Pediatr Dermatol. (2006) 23:13–8. 10.1111/j.1525-1470.2006.00161.x 16445403 · doi ↗ · pubmed ↗
- 6Fujimoto A Farooq M Fujikawa H Inoue A Ohyama M Ehama R A missense mutation within the helix initiation motif of the keratin K 71 gene underlies autosomal dominant woolly hair/hypotrichosis. J Invest Dermatol. (2012) 132:2342–9. 10.1038/jid.2012.154 22592156 · doi ↗ · pubmed ↗
- 7Shi P Chen W Lyu X Wang Z Li W Jia F Loss-of-function mutations in Keratin 32 gene disrupt skin immune homeostasis in pityriasis rubra pilaris. Nat Commun. (2024) 15:6259. 10.1038/s 41467-024-50481-z 39048559 PMC 11269665 · doi ↗ · pubmed ↗
- 8Shimomura Y Wajid M Petukhova L Kurban M Christiano A. Autosomal-dominant woolly hair resulting from disruption of keratin 74 (KRT 74), a potential determinant of human hair texture. Am J Hum Genet. (2010) 86:632–8. 10.1016/j.ajhg.2010.02.025 20346438 PMC 2850421 · doi ↗ · pubmed ↗