A Rare Case of Prostate Abscess With Pyelonephritis in an Adolescent Male
Hasan A Al-Ibraheem, George Hill

TL;DR
A 16-year-old male with no prior health issues developed a rare prostatic abscess and kidney infection, which improved after drainage and antibiotics.
Contribution
This paper presents a rare case of prostatic abscess in an adolescent male and highlights the effectiveness of transperineal drainage.
Findings
The patient had bilateral pyelonephritis and a prostatic abscess, confirmed through imaging.
Conservative antibiotic treatment alone was ineffective, but drainage improved the condition significantly.
Transperineal aspiration is a safe and minimally invasive treatment option for this rare condition in adolescents.
Abstract
Prostatic abscess is a rare urological condition in adolescents. We report the case of a 16-year-old male with no significant past medical history who presented with bilateral flank pain, dysuria, and systemic signs of infection. Imaging revealed bilateral pyelonephritis and a prostatic abscess. Initial conservative treatment with intravenous antibiotics alone showed no improvement, prompting ultrasound-guided transperineal aspiration of the abscess under general anesthesia along with antibiotics. The patient showed marked clinical improvement and was discharged. This case highlights the importance of including prostatic abscess in the differential diagnosis for adolescent males with persistent urinary symptoms and sepsis. It demonstrates the efficacy of transperineal drainage as a relatively safe and minimally invasive intervention in this population.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
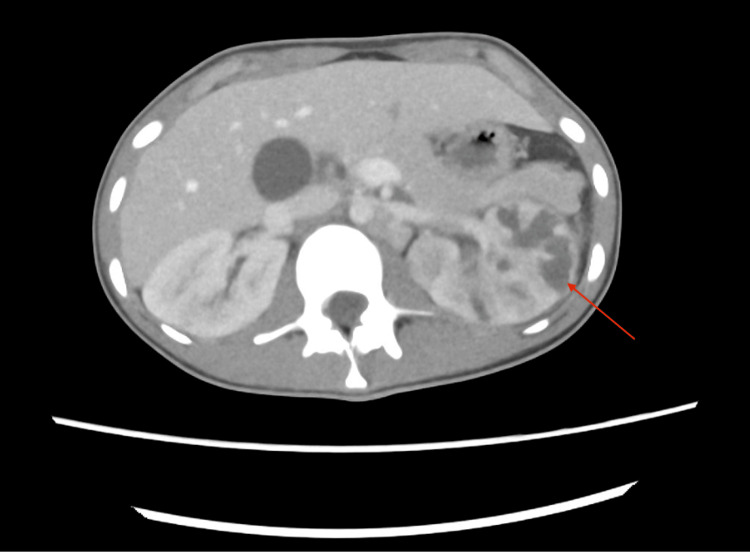 Figure 1
Figure 1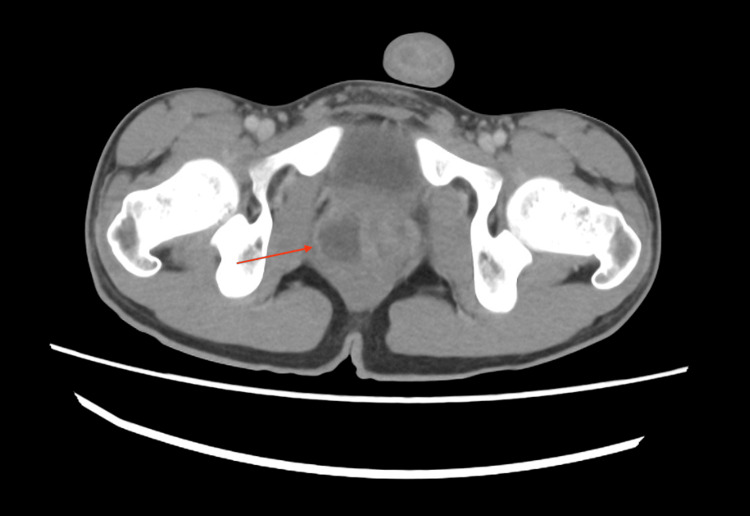 Figure 2
Figure 2| Age | Pathogen | Possible risk factors | Treatment |
| 5 [ | Pseudomonas aeruginosa | Autism spectrum disorder, poor nutrition | Antibiotics, vitamins, and trace elements |
| 14 [ | Escherichia coli | Repetitive forceful influx of contaminated water into the urethra | Antibiotics only |
| 15 [ | MRSA | Previous history of MRSA infection | Transurethral unroofing of prostatic abscess and antibiotics |
| 13 [ | MRSA | No risk factors are known | Ultrasound-guided transrectal drainage and antibiotics |
| 11 [ | Methicillin-susceptible Staphylococcus aureus | Pulmonary hypertension | Ultrasound-guided percutaneous drainage and antibiotics |
| 6 [ | Staphylococcus aureus | Poststreptococcal glomerulonephritis | Surgical drainage (the approach is not clear) and antibiotics |
| 15 [ | Not specified | X-linked chronic granulomatous disease | TRUS-guided prostatic aspiration, transurethral resection and drainage of the prostate abscess, and antibiotics |
| 12 [ | Staphylococcus aureus | No risk factors are known | Transurethral incision of prostate abscess and antibiotics |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrologic and reproductive health conditions · Urological Disorders and Treatments · Urinary Bladder and Prostate Research
Introduction
A prostatic abscess is an uncommon urological condition, typically seen in men in their fifth and sixth decades of life and very rarely encountered in the adolescent population [1]. The most frequently isolated pathogen in prostatic abscesses is Escherichia coli, followed by Klebsiella pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, and occasionally other organisms [2]. The condition presents a diagnostic challenge in younger patients due to its rarity, overlap with more common pediatric infections, lack of routine prostate examination, and nonspecific symptoms. Treatment ranges from antibiotics to more invasive and surgical interventions [2]. We report a rare case of prostatic abscess associated with bilateral pyelonephritis in an adolescent male with no risk factors identified yet, apart from low BMI on admission.
Case presentation
A 16-year-old male, previously fit and well apart from low body weight (47.4 kg, height 175 cm, BMI 15.5 kg/m²), presented with a three-day history of bilateral flank pain and dysuria. He had no significant past medical history and a normal developmental history. On examination, he was febrile and tachycardic with diffuse abdominal tenderness. He appeared sarcopenic, with a soft, non-distended abdomen. A digital rectal examination revealed a tender, enlarged, and boggy prostate. His blood tests showed a white blood cell count of 31.1 x 10^9/L (normal: 4.0-11.0 x 10^9/L), a C-reactive protein level of 221 mg/L (normal: <10), and a creatinine level of 157 μmol/L.
A contrast-enhanced CT scan of the abdomen and pelvis was performed. It demonstrated a grossly abnormal left kidney with multifocal areas of loss of corticomedullary differentiation, some of which were wedge-shaped in configuration. There was diffuse urothelial thickening of the left renal pelvis and proximal ureter. These findings were concerning for acute pyelonephritis with proximal ureteritis. The right kidney exhibited areas of early corticomedullary differentiation loss, consistent with early pyelonephritis (Figure 1). The prostate was enlarged, with a hypodense lesion in the right lobe, suggestive of a prostatic abscess (Figure 2).
Contrast-enhanced scan of the abdomen in the axial view showing features suggestive of pyelonephritisCT: computed tomography
Contrast-enhanced CT scan of the pelvis in the axial view showing hypodense lesion in the right lobe of the prostate suggestive of prostate abscessCT: computed tomography
The patient was managed empirically for sepsis; he was catheterized, blood and urine cultures were sent, and empirical intravenous antibiotics (piperacillin/tazobactam and metronidazole) were initiated following consultation with microbiology. Given the patient's young age, conservative management was initially preferred. However, due to the lack of clinical improvement, an ultrasound-guided transperineal aspiration of the abscess was performed under general anesthesia with a 14G needle to avoid transurethral or transrectal approaches in an attempt to reduce the risks of urinary incontinence or fistula. Approximately 3 mL of pus was aspirated to dryness and sent for microbiological analysis.
The culture results showed light growth of Pseudomonas aeruginosa and scant growth of Enterococcus faecium, while the urine culture revealed growth of Pseudomonas aeruginosa. Consequently, teicoplanin was administered for 14 days, and piperacillin/tazobactam was switched to oral ciprofloxacin 750 mg twice daily, based on the cultures' sensitivities and a discussion with the microbiology team. Nutritional support, including high-protein oral supplements, was initiated following the dietitian's assessment to address the patient's low BMI and poor oral intake during admission. The patient showed significant clinical and biochemical improvement. Inflammatory markers (white blood cells and C-reactive protein) trended downward, and the patient was discharged after 14 days to complete antibiotics in the community. His urethral catheter was successfully removed following discharge.
Further investigations were performed to identify potential underlying risk factors, including serological screening for hepatitis B virus, hepatitis C virus, and human immunodeficiency virus, which was negative; immunoglobulin levels were within normal range; complement levels were mildly reduced (C3 at 0.86 g/L (normal: 0.90-1.60 g/L) and C4 at 0.08 g/L (normal: 0.14-0.54 g/L)); and transthoracic echocardiogram revealed only trivial to mild pulmonary regurgitation and no vegetations.
He is awaiting an indirect MAG3 renogram, micturating cystourethrogram, and further assessment by the immunology team to address the mildly reduced complement levels. He has ongoing follow-ups with the dietitian.
Discussion
A prostatic abscess is an uncommon but recognized complication of acute bacterial prostatitis, characterized by a localized collection of pus within the prostate. It predominantly affects men in their fifth and sixth decades of life and is rare in adolescents and children outside the neonatal period. Common risk factors include bladder outlet obstruction, recent urological instrumentation, prolonged catheterization, neurogenic bladder dysfunction, diabetes mellitus, and other chronic comorbidities [1].
Pseudomonas aeruginosa is one of the causative pathogens [2]. The clinical presentation can vary but typically includes lower urinary tract symptoms (dysuria, frequency, and urgency), acute urinary retention, fever, lower abdominal or back pain, and occasionally hematuria. On digital rectal examination, the prostate may be tender, enlarged, or fluctuant, raising suspicion of an abscess [3].
Diagnosis is confirmed radiologically. Transrectal ultrasound (TRUS) is a common initial imaging modality, detecting up to 80% of cases [4]. However, CT and MRI offer superior delineation of the abscess and assessment for extra-prostatic extension. CT is particularly useful in detecting renal and ureteric involvement [5], while MRI provides high-resolution soft tissue imaging [6]. In our case, we opted for a CT scan as it was more readily available in the emergency setting overnight, unlike ultrasound or MRI.
Initial treatment involves broad-spectrum antibiotics. While some cases respond to medical therapy alone, surgical drainage significantly reduces the duration of symptoms and hospital stays [2]. Minimally invasive techniques, including TRUS or transperineal aspiration, are preferred due to the reduced risk of complications. These can be performed under local or general anesthesia, and aspirated fluid should be sent for culture [7]. In refractory or multiloculated abscesses, transurethral deroofing may be necessary [8]. Open drainage is rarely indicated and reserved for extensive abscesses involving adjacent spaces such as the perirectal or perineal regions. Other complications of untreated or severe abscesses include fistula formation, sepsis, septic emboli, and even death [9].
Transperineal drainage of prostate abscesses may be less invasive, preserve ejaculatory function, and avoid urethral injury [10]. However, due to the rarity of the condition, there is insufficient data to support this approach definitively.
A literature review was conducted using the PubMed, Scopus, Embase, and EBSCOhost electronic databases, focusing on the following terms: “prostate abscess AND adolescence” and “prostate abscess AND paediatric”, with a focus on case reports. We excluded results in the neonatal period. We identified eight case reports, which are shown in Table 1.
Our patient is a 16-year-old with a reduced BMI who developed a prostate abscess, probably due to an ascending urine infection; hence, it was associated with severe pyelonephritis. After failing to respond to conservative management with intravenous antibiotics, we elected for transperineal drainage, which improved his condition. The patient will need further follow-up and monitoring to assess for any recurrence or complications.
Conclusions
Prostatic abscesses, although rare in adolescents, should be part of the differential diagnosis in young patients presenting with persistent urinary and systemic symptoms unresponsive to antibiotics. Early imaging and intervention are crucial in preventing complications. Escalation from conservative to invasive management should be considered when there is no improvement or worsening of the clinical condition. In this case, transperineal drainage proved to be an effective method, resulting in a successful outcome. However, there is not enough evidence, and further studies are required about prostate abscess in this age group and its management. Follow-up and monitoring are crucial for young patients to detect any recurrence or late complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnosis and treatment of patients with prostatic abscess in the post-antibiotic era Int J Urol Ackerman AL Parameshwar PS Anger JT 1031102520182894450910.1111/iju.13451 · doi ↗ · pubmed ↗
- 2Acute bacterial prostatitis and abscess formation BMC Urol Lee DS Choe HS Kim HY Kim SW Bae SR Yoon BI Lee SJ 381620162738800610.1186/s 12894-016-0153-7PMC 4936164 · doi ↗ · pubmed ↗
- 3Treatment of prostatic abscess: case collection and comparison of treatment methods Korean J Urol Jang K Lee DH Lee SH Chung BH 8608645320122330113110.4111/kju.2012.53.12.860PMC 3531640 · doi ↗ · pubmed ↗
- 4Diagnostic and therapeutic utility of transrectal ultrasound in urological office prostatic abscess management: a short report from a single urologic center Arch Ital Urol Androl Fabiani A Filosa A Maurelli V 3443488620142564146810.4081/aiua.2014.4.344 · doi ↗ · pubmed ↗
- 5Prostatic abscess: CT and sonographic findings AJR Am J Roentgenol Thornhill BA Morehouse HT Coleman P Hoffman-Tretin JC 8999001481987355492210.2214/ajr.148.5.899 · doi ↗ · pubmed ↗
- 6Case series: diffusion weighted MRI appearance in prostatic abscess Indian J Radiol Imaging Singh P Yadav MK Singh SK Lal A Khandelwal N 46482120112143103310.4103/0971-3026.76054 PMC 3056370 · doi ↗ · pubmed ↗
- 7Management of prostate abscess in the absence of guidelines Int Braz J Urol Abdelmoteleb H Rashed F Hawary A 8358404320172837966110.1590/S 1677-5538.IBJU.2016.0472 PMC 5678513 · doi ↗ · pubmed ↗
- 8Transurethral resection of prostate abscess: is it different from conventional transurethral resection for benign prostatic hyperplasia?ISRN Urol Goyal NK Goel A Sankhwar S Dalela D 109505201320132384096910.1155/2013/109505 PMC 3693178 · doi ↗ · pubmed ↗