Spontaneous Refractory Intercostal Artery Hemorrhage in a Patient With Decompensated Liver Cirrhosis
Jiro Kimura, Prakash Chauhan, Calvin Eriksen, Matthew Cooper, Raj Prasad

TL;DR
A patient with liver cirrhosis experienced spontaneous intercostal artery bleeding, successfully managed through liver transplantation.
Contribution
This case highlights the rare occurrence of spontaneous ICAH in decompensated cirrhosis and its successful treatment via liver transplantation.
Findings
Spontaneous ICAH occurred in a cirrhotic patient without trauma.
Liver transplantation resolved coagulopathy and prevented further bleeding.
Prompt management was critical in a high-risk patient with acute liver failure.
Abstract
Intercostal artery hemorrhage (ICAH) is an uncommon occurrence that may lead to significant clinical complications if not promptly addressed. We present the case of a 39-year-old man with a history of liver cirrhosis who was waitlisted for liver transplantation (LT). He presented with acute, severe left shoulder pain without any recent trauma. Contrast-enhanced computed tomography revealed a left posterolateral chest wall intramuscular hematoma with active contrast extravasation originating from the left sixth intercostal artery. Interventional radiology angiography confirmed the extravasation, and embolization was successfully performed to achieve hemostasis. Despite the embolization, the patient required blood transfusions due to a gradually decreasing hemoglobin level. Five days after the initial procedure, CT angiography identified additional multifocal small arterial hemorrhages.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
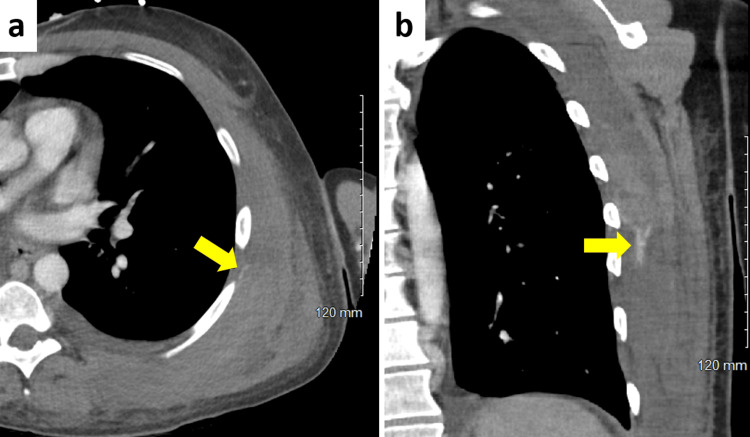 Figure 1
Figure 1 Figure 2
Figure 2| Test | Reference range | At hospital admission | At the time of LT |
| White blood cells (10³/μL) | 3.9-11.2 | 8.9 | 5.4 |
| Hemoglobin (g/dL) | 13.7-17.5 | 6.4 | 7.8 |
| Hematocrit (%) | 40-51 | 19 | 23 |
| Platelets (10³/μL) | 165-366 | 67 | 47 |
| Sodium (mmol/L) | 136-145 | 138 | 141 |
| Potassium (mmol/L) | 3.4-5.1 | 3.6 | 2.9 |
| Bilirubin (mg/dL) | 0.2-1.2 | 6.3 | 15.8 |
| Creatinine (mg/dL) | 0.70-1.30 | 0.73 | 1.49 |
| PT-INR | 0.8-1.1 | 2.1 | 2.1 |
| No. | Author | Year | Age | Sex | Symptoms | Hemodynamic status | Bleeding site | Diagnostic imaging | Ruptured intercostal artery | Laterality | Treatment | Complications | Prognosis | Contributing factor | Antithrombotic medications |
| 1 |
Dua et al. [ | 2014 | 47 | Male | Right chest pain and dyspnea | Shock | Right thorax | CT | 11th | Right | Thoracotomy | None | Alive | None | None |
| 2 |
Sangani and Naliath [ | 2020 | 60 | Male | Left chest and abdominal pain | Stable | Left chest wall and thorax | CT | 8th | Left | Surgery | None | Alive | Cough | None |
| 3 |
Jang et al. [ | 2015 | 39 | Male | Left flank pain | Stable | Left retroperitoneum | CT | 11th | Left | Conservative | None | Alive | Cough | None |
| 4 |
Yu et al. [ | 2006 | 76 | Male | Suddenly enlarging mass | Stable | Right abdominal wall | CT | 10th | Right | TAE | None | Alive | Cough | None |
| 5 |
Moon et al. [ | 2008 | 45 | Male | Right flank pain | Stable | Retroperitoneum | CT | 10th and 11th | Right | TAE | None | Alive | Hypertension | None |
| 6 |
Mathew et al. [ | 2008 | 69 | Male | Left chest pain | Shock | Left thorax and abdominal wall | CT | 10th | Left | TAE | None | Alive | Unknown | None |
| 7 |
Lu et al. [ | 2012 | 50 | Female | Left shoulder pain | Stable | Left shoulder | CT | 4th | Left | TAE | Alveolar hemorrhage | Died of alveolar hemorrhage | SLE | Enoxaparin |
| 8 |
Dobrilovic et al. [ | 2013 | 62 | Female | Chest and back pain | Shock | Left thorax | MRI | NA | Left | TAE | NA | Alive | Unknown | None |
| 9 |
Ishida et al. [ | 2014 | 58 | Male | Back pain | Stable | Posterior mediastinum | CT | 10th | Right | Conservative | None | Alive | None | None |
| 10 |
Junck and Utarnachitt [ | 2015 | 63 | Male | Back pain | Stable | Posterior mediastinum | CT | 8th | Right | TAE | None | Alive | None | None |
| 11 |
Afonso et al. [ | 2020 | 76 | NA | Right shoulder pain | Stable | Right subscapular region | CT | 5th | Right | TAE | None | Alive | Hemodialysis | Acetylsalicylic acid |
| 12 |
Izumoto [ | 2022 | 48 | Male | Back pain | Stable | Posterior mediastinum | CT | 9th | Right | TAE | None | Alive | None | None |
| 13 | Our case | 2025 | 39 | Male | Left shoulder pain | Stable | Left chest wall | CT | 6th | Left | TAE | Liver failure | Alive | Cirrhosis | None |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Abdominal vascular conditions and treatments · Abdominal Trauma and Injuries
Introduction
Intercostal artery hemorrhage (ICAH) is a rare but potentially life-threatening condition [1]. Severe coughing is recognized as a major contributing factor in some cases [2]. The most common underlying cause of ICAH is trauma, which may include blunt or penetrating injuries, as well as iatrogenic causes such as thoracentesis or surgical procedures [3]. While spontaneous rupture of the intercostal artery can occur, it is much less frequent and typically associated with underlying conditions such as neurofibromatosis type 1, coarctation of the aorta, connective tissue disorders (e.g., Marfan syndrome), or severe hypertension [4]. The overall incidence of ICAH is extremely low and cannot be reliably quantified from current literature, with most data derived from isolated case reports and small series.
According to the literature, undiagnosed or untreated intercostal artery injury can result in massive hemothoraces. While initial tamponade may occur, rebleeding is possible, potentially leading to recurrent or retained hemothorax and hemodynamic instability [5]. Fatal outcomes have been reported, particularly when bleeding is not promptly recognized and managed, as ICAH can be both life-threatening and technically challenging to control, even with surgical intervention.
To the best of our knowledge, ICAH leading to hepatic decompensation, defined by the new onset of ascites, hepatic encephalopathy, variceal bleeding, or jaundice, in a cirrhotic patient has not been previously reported [6]. Herein, we present a case of a cirrhotic patient who fully recovered from refractory ICAH following liver transplantation (LT).
Case presentation
A 39-year-old man with a history of liver cirrhosis secondary to cryptogenic cirrhosis presented to the emergency department with complaints of acute, severe left shoulder pain without any recent injury. He was triaged as level 4 according to the Emergency Severity Index [7]. His past medical history included hypertension, hepatic encephalopathy, ascites, esophageal varices, and portal vein thrombosis. His Model for End-Stage Liver Disease 3.0 score was 24 points, and he had been on the waiting list for LT for six months [8]. He was not taking any antithrombotic medications.
He denied having a fever, cough, or chest pain. On examination, his vital signs were within normal limits. He appeared jaundiced and had a bruise with tenderness on his left back. Laboratory results showed a drop in hemoglobin from 8.6 g/dL three days earlier to 6.4 g/dL and a prothrombin time international normalized ratio of 2.1. A shoulder X-ray revealed no acute fracture or dislocation, and the regional soft tissues appeared intact. Contrast-enhanced CT revealed an intramuscular hematoma in the left posterolateral chest wall with active contrast extravasation originating from the left sixth intercostal artery (Figure 1).
Contrast-enhanced abdominal CT scan showing contrast extravasation at the level of the sixth intercostal space (arrow): (a) axial view and (b) coronal view
He was admitted to our hospital, and interventional radiology was consulted for arterial embolization. Angiography revealed contrast extravasation from the left sixth intercostal artery (Figure 2). Embolization was performed, and hemostasis was achieved. However, he continued to require blood transfusions due to a gradual decline in hemoglobin levels. Five days after the initial embolization, CT angiography was performed and revealed additional multifocal small arterial hemorrhages. A compression binder was applied to his chest wall, which provided partial effectiveness.
Interventional radiology and TAEThe ICAH was identified, and TAE was subsequently performed.ICAH, intercostal artery hemorrhage; TAE, transcatheter arterial embolization
Despite these interventions, he developed acute-on-chronic liver failure. His bilirubin and creatinine levels progressively increased from 6.3 mg/dL and 0.73 mg/dL to 15.8 mg/dL and 1.49 mg/dL, respectively (Table 1). Fortunately, a deceased donor LT was performed eight days after admission. Following the surgery, his coagulation status normalized, and no postoperative hemorrhage occurred. His postoperative course was uneventful, with no recurrence of ICAH, and he was discharged on postoperative day 9.
Discussion
Table 2 summarizes the reported cases of spontaneous ICAH [1,2,5,9-17]. Since the first case was described in 2005, only 13 cases, including the present one, have been reported to date. The median patient age was 58 years (IQR: 45-69), with a male predominance (10 males and two females). The most common presenting symptom was pain (12 out of 13 patients). Identified contributing factors included cough (n = 3), cirrhosis (n = 1), hypertension (n = 1), systemic lupus erythematosus (n = 1), and hemodialysis (n = 1). Interestingly, four patients had no identifiable contributing factors. Three patients presented in shock following the hemorrhage.
The most common cause of ICAH is trauma [18]. Other reported etiologies include rupture of intercostal artery aneurysms associated with conditions such as neurofibromatosis type 1 and coarctation of the aorta, as well as anticoagulant use, bleeding disorders, pulmonary infections, and uncontrolled hypertension [4]. Some authors have also documented cases of spontaneous ICAH occurring without a clear inciting event, such as trauma, or in the absence of identifiable arterial wall pathology or associated systemic disease [1]. Notably, to the best of our knowledge, this is the first reported case of ICAH leading to acute-on-chronic liver failure in a patient with cirrhosis.
Except for one patient who underwent magnetic resonance imaging due to a contrast allergy, all other cases were diagnosed using CT. Hemorrhage occurred on the left side in six patients and on the right side in seven. The majority of patients were treated with transcatheter arterial embolization (TAE) (n = 9). Eight patients recovered without complications. However, our patient developed liver failure due to recurrent ICAH following TAE. One patient, who had systemic lupus erythematosus and was receiving enoxaparin, died due to alveolar hemorrhage.
Fortunately, the patient underwent LT eight days after the onset of ICAH. Following LT, his coagulation status normalized, and no further bleeding was observed. However, in patients with a high risk of bleeding, ICAH may be fatal due to hemorrhage that is refractory to standard treatment, although the overall mortality rate of this condition remains unknown [5]. In such cases, rapid and intensive management, including correction of coagulopathy, is essential.
Conclusions
We presented the case of a cirrhotic patient who developed ICAH as a result of abnormal coagulation, ultimately progressing to liver decompensation. Despite initial management with TAE, the patient experienced recurrent hemorrhage and acute-on-chronic liver failure, illustrating the challenging and refractory nature of ICAH in patients with cirrhosis. Fortunately, urgent LT successfully corrected the underlying coagulopathy and resolved the bleeding, leading to full recovery. This case highlights the importance of prompt and aggressive intervention, including correction of coagulopathy, in cirrhotic patients with ICAH, as the condition may be life-threatening in this vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Idiopathic spontaneous rupture of an intercostal artery WMJ Dua A Dua A Jechow S Desai SS Kuy S 1161181132014 https://wmjonline.org/wp-content/uploads/2014/113/3/116.pdf 25118440 · pubmed ↗
- 2First case of cough-induced combined intercostal artery rupture with partial diaphragm tear Indian J Thorac Cardiovasc Surg Sangani NK Naliath SM 6396423620203310062610.1007/s 12055-020-01004-0PMC 7573052 · doi ↗ · pubmed ↗
- 3A novel, minimally invasive approach to assure hemostasis for intercostal bleeding after trauma J Trauma Acute Care Surg Park H Glaser J Florecki K Schmoekel N Du Bose J Stein D Scalea T 102710298420182946208210.1097/TA.0000000000001853 · doi ↗ · pubmed ↗
- 4Spontaneous bleeding from multiple intercostal arteries in a patient with coarctation of the aorta Ann Thorac Surg Wightman SC Wang Y Rohr AM Greene CL Hwang GL Watkins AC Lui NS 07110202010.1016/j.athoracsur.2019.12.04232035043 · doi ↗ · pubmed ↗
- 5Spontaneous rupture of intercostal artery after severe cough Am J Emerg Med Jang JY Lim YS Woo JH Jang JH 13113333201510.1016/j.ajem.2014.06.03325085284 · doi ↗ · pubmed ↗
- 6Towards a new definition of decompensated cirrhosis J Hepatol D'Amico G Bernardi M Angeli P 2022077620223415732210.1016/j.jhep.2021.06.018 · doi ↗ · pubmed ↗
- 7Implementation and refinement of the emergency severity index Acad Emerg Med Wuerz RC Travers D Gilboy N Eitel DR Rosenau A Yazhari R 170176820011115729410.1111/j.1553-2712.2001.tb 01283.x · doi ↗ · pubmed ↗
- 8MELD 3.0: the model for end-stage liver disease updated for the modern era Gastroenterology Kim WR Mannalithara A Heimbach JK 1887189516120213448184510.1053/j.gastro.2021.08.050PMC 8608337 · doi ↗ · pubmed ↗