Tracheal schwannoma: A pseudo-asthmatic syndrome with successful laser Nd-YAG resection as first-line therapy
Ranim Nakhal, Raneem Ahmad, Bassel Ibrahim, Sultaneh Haddad, Arabi Abbas, Nizar Abbas

TL;DR
A rare tracheal tumor called schwannoma was successfully treated with laser surgery, highlighting its potential to mimic asthma symptoms.
Contribution
Demonstrates successful use of Nd-YAG laser as first-line therapy for tracheal schwannoma.
Findings
Nd-YAG laser resection effectively removed the schwannoma with no recurrence observed.
Schwannoma can present with pseudo-asthmatic symptoms, leading to potential misdiagnosis.
Rigid bronchoscopy combined with laser therapy is a viable and effective treatment approach.
Abstract
Neurogenic tumors like schwannoma are sporadic in less than 0.5 % of primary tracheal tumors (PTT). Schwannoma can be misdiagnosed with asthma because of nonspecific symptoms such as wheezing, coughing, or dyspnea. A 39-year-old woman presents to the emergency department with severe dyspnea at rest and needs oxygenation. Rigid Bronchoscopy revealed an intratracheal white pedunculated lesion with visible vessels. A frozen section's result was benign Showannoma. Nd-YAG Laser was performed to melt the tumor, and then the lesion was swept away. After that, the Nd-YAG laser was used to remove tumor remnants. Our case emphasizes that rigid bronchoscopy with Nd-YAG laser resection was a very successful tool for managing schwannoma, and bronchoscopic surveillance showed No Recurrence as the benign nature of pedunculated schwannoma without an extratracheal component. Awareness of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
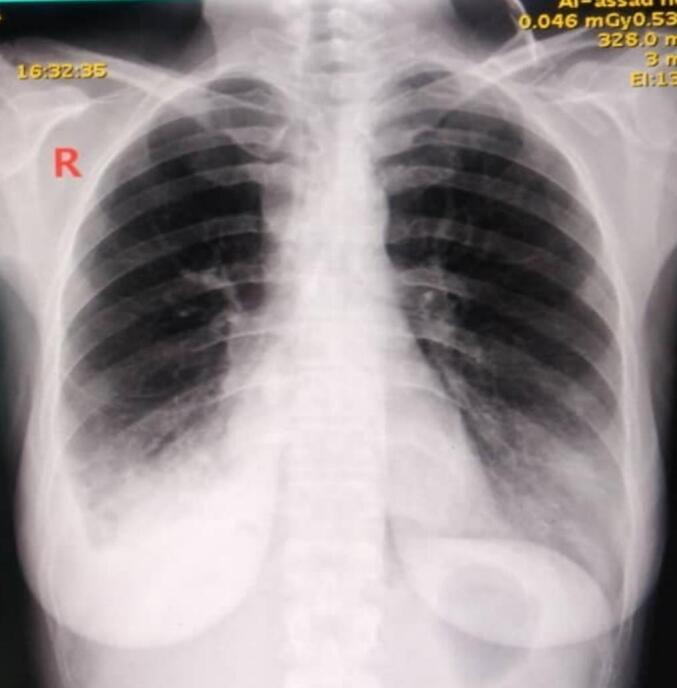 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3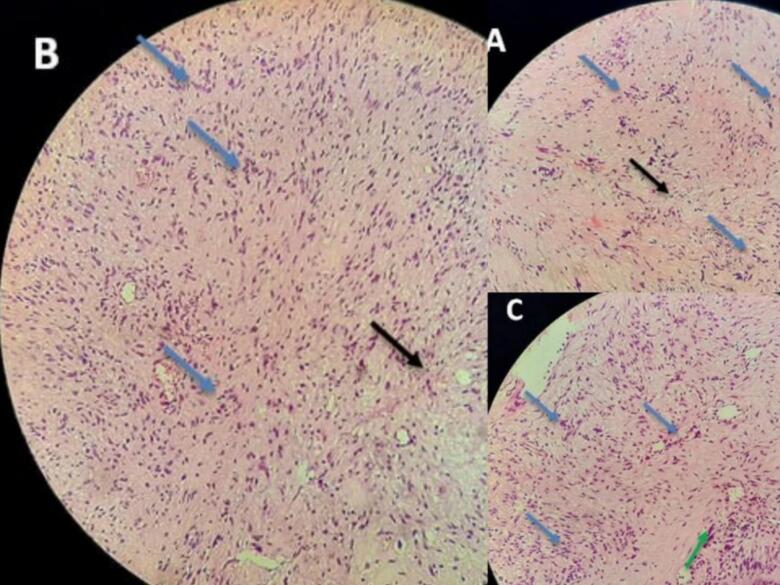 Figure 4
Figure 4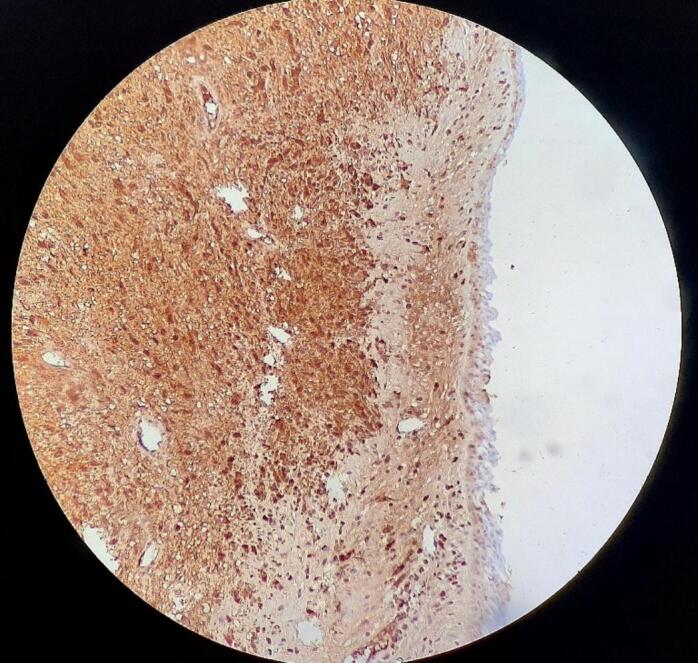 Figure 5
Figure 5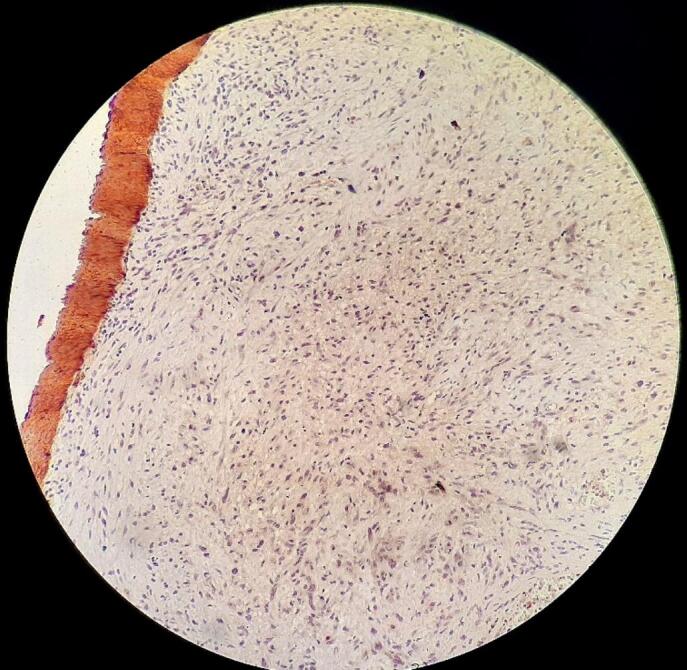 Figure 6
Figure 6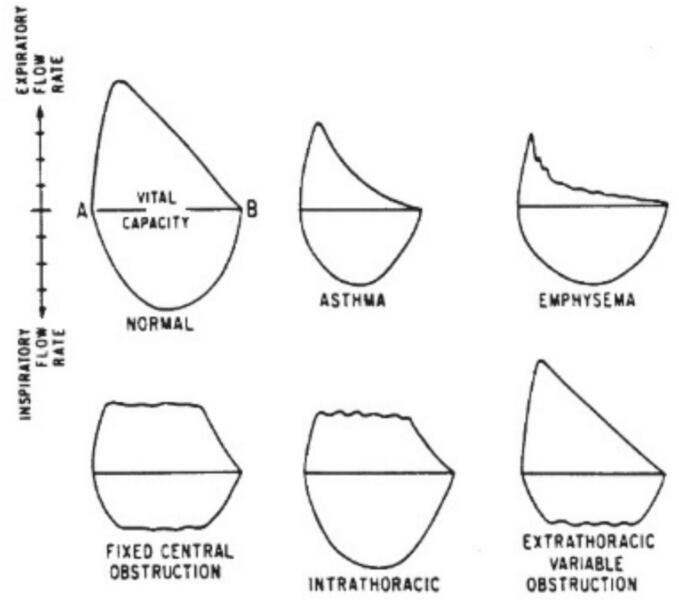 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Neurofibromatosis and Schwannoma Cases · Myasthenia Gravis and Thymoma
Introduction
1
PTT depicts 2 % of upper airway tumors and 0.1–0.4 % of all malignancies. Moreover, 90 % of them are malignant in adults [1,2]. Neurogenic tumors like schwannoma and neurofibromas are sporadic in less than 0.5 % of PTT, and 0.2 % are for schwannoma [1,[3], [4], [5]]. Clinically, schwannoma can be misdiagnosed with asthma because of nonspecific symptoms such as wheezing, coughing, or dyspnea. The response to bronchodilators or corticosteroids is characteristic of asthma. Failure to observe an improvement in lung function should prompt the consideration of other investigative methods to exclude pseudo-asthmatic syndromes. [[6], [7], [8]] Laser resection has been used increasingly over the last decade without significant morbidity, and the Nd-YAG laser should be considered first-line therapy in benign endobronchial tumors within certain conditions [9,10]. In our case, we presented a schwannoma tumor that made a pseudo-asthmatic syndrome, emphasizing that rigid bronchoscopy with Nd-YAG laser resection was a very successful tool for managing schwannoma, and bronchoscopic surveillance showed no recurrence.
Case presentation
2
A 39-year-old female presented to the emergency department with a two-year history of progressive dyspnea and a persistent dry cough. The symptoms had gradually worsened over time, prompting medical evaluation. During that period, she was treated as an asthmatic patient with bronchodilators and steroids with little improvement. Additionally, her respiratory symptoms were significantly exacerbated during pregnancy, necessitating frequent medical interventions for recurrent respiratory infections and hypoxemia, eventually leading to oxygen dependence. Following childbirth, she required urgent hospitalization.
Clinical examination revealed the presence of stridor. Vital signs were as follows: blood pressure 120/70 mmHg, pulse rate 88 beats per minute, body temperature 37 °C, respiratory rate 28 breaths per minute, and oxygen saturation 85 % on room air. The other systems examination showed no additional abnormalities. A shadow in the trachea with bilateral pulmonary infiltrates and right angle closure was on the chest X-ray [Fig. 1]. CT-Scan showed a large lesion obstructing 95 % of the inferior third of the tracheal lumen without extratracheal component [Fig. 2]. Rigid Bronchoscopy revealed an intratracheal white pedunculated lesion with visible vessels, occupying 95 % of the lumen [Fig. 3]. A frozen section's result was benign Showannoma. Nd-YAG Laser was performed to melt the tumor, and then the lesion was removed by large biopsy forceps. After that, the Nd-YAG laser was used to coagulate and remove the tumor remnant. The procedure was performed under general anesthesia and lasted approximately 30 min.Fig. 1. Chest x-ray showing A shadow in the trachea with bilateral pulmonary infiltrates and right angle closureFig. 1Fig. 2CT scan showing a large lesion obstructing 95 % of the inferior third of the tracheal lumen without extratracheal component.Fig. 2. Fig. 3Bronchoscopic view. An intratracheal white pedunculated lesion with visible vessels (the arrow).Fig. 3
A routine pathologic study consistent with schwannoma revealed Spindle cells in short fascicles, hypercellular areas (Antoni A) with nuclear palisading, paucicellular areas (Antoni B), and squamous metaplasia with low-grade dysplasia in the tracheal epithelium [Fig. 4]. S-100 protein immunoreactivity was positive [Fig. 5], and CK stain (Cytokeratin AE1/AE3) was negative [Fig. 6], confirming the schwannoma diagnosis.Fig. 4. Hematoxylin and eosin stain: Spindle cells with twisted nuclei with indistinct cytoplasmic borders, Antoni A areas with nuclear palisading (blue arrows), Antoni B areas (black arrows), and squamous metaplasia with low-grade dysplasia in the tracheal epithelium (green arrow).Fig. 4. Fig. 5S-100 protein was positive on immunohistochemical test.Fig. 5. Fig. 6CK stain was negative on the immunohistochemical test.Fig. 6
No recurrence was observed through follow-up by flexible bronchoscopy at 10 months postoperatively.
Discussion
3
Primary Tracheal Tumors (PTT) depict 2 % of upper airway tumors and 0.1–0.4 % of all malignancies. Moreover, 90 % of them are malignant in adults [1,2].
PTT can originate from epithelial, adenoid, or mesenchymal sources. Two-thirds (85 %) of adults' PTT consists of squamous and adenoid cystic carcinoma, with the same incidence rate [1,2,11].
Benign tumors, low-grade malignancies, and other wide variety of histological subtypes make up the last third. Thus, Neurogenic tumors like schwannoma and neurofibromas are sporadic in less than 0.5 % of PTT [1,3,4].
Schwannoma is a well-circumscribed encapsulated neoplasm, connected to the nerve sheath loosely without invading it, with sporadic occurrence, while a small percentage is associated with von Recklinghausen's disease [12,13]. The most common locations for it are the cerebellopontine angle, flexor surfaces of the extremities, mediastinum, neck, and posterior spinal roots [12,13]. Malignant transformation of schwannoma is exceptionally rare and mostly exhibits an epithelioid morphology [13].
Tracheal schwannoma is an uncommon presentation, most common in the distal bronchial tree or lung parenchyma, with a female gender preference for a male-to-female ratio of 7:21. [7,[14], [15], [16], [17]] The distal third of the trachea is more involved, followed by the proximal and then the middle third [17].
Diagnosis can be challenging, with an average delay of 17 months from the onset of symptoms [17]. Thus, some points need to be highlighted to avoid delay and misdiagnosis:
- •Symptoms appear as non-specific clinical manifestations when the tumor occludes around 50–70 % of the tracheal lumen, while 30–75 % of the chest radiograph shows normal findings [1,18].
- •Symptoms can mimic asthma and create a pseudo-asthma status:
Cough, wheezing, and dyspnea result from causes other than asthma [2,6,8]. Most chronic cough cases in adults are caused by asthma (the most common etiology), gastroesophageal reflux disease, and chronic rhinosinusitis. Thus, it is a presentation of nonpulmonary disorders as well as pulmonary ones [19]. Moreover, stridor or wheezing can be mistaken for asthma, while it may arise in tracheal obstruction, foreign body, bronchomalacia, or even as a physician misestimating various respiratory sounds [1,6,8,20].
Substantial improvement of airway obstruction from an aerosol bronchodilator (greater than 12 % and a greater than 250 mL increase in the forced expiratory volume in 1 s (FEV 1) after bronchodilator) or a short course of reasonably high-dose systemic corticosteroid, 2 mg/kg twice daily to a maximum of 40 mg twice daily, is characteristic of diagnosing asthma. Failure to observe a relief and improvement in lung function within 5 to 7 days or 10 days maximum, should consider a fiberoptic bronchoscopy or CT scan to evaluate the airways for any other causes as the etiology. [[6], [7], [8]] Pseudo-asthmatic syndromes are shown in [Table 1]. [8]Table 1. Pseudo-asthmatic syndromes.Table 1. Bronchial inflammatory diseases Infectious asthma Bronchiolitis and croup Chronic asthmatic bronchitis Cystic fibrosisEmphysemaCentral airway obstructionCardiac asthmaAspiration syndromesPulmonary embolismCarcinoid syndromesHypersensitivity pneumonitisPulmonary infiltration with eosinophiliaSarcoidosisPsychogenic dyspnea and factitious asthma
Central airway obstruction (CAO) as a Pseudo-asthmatic syndrome can result from a wide variety of diseases shown in [Table 2]. [8]Table 2. Important causes of central airway obstruction.Table 2. Obstruction TypeCharacteristicsPharyngealRetropharyngeal abscessLudwig's anginaTonsil or adenoid enlargementLaryngealVocal cord palsyEpiglottitis Laryngeal edemaTumor, polypRelapsing polychondritisExtrinsic trachea/bronchial compressionMediastinal tumorAneurysmMediastinal abscessGoiterIntramural tracheal/bronchial diseaseStrictureFractureTracheomalaciaTracheopathia osteoplasticaRelapsing polychondritisWegener's granulomatosisIntraluminal tracheal diseaseTumors, benign or malignantTracheitis dessicansRelapsing polychondritisForeign bodyNonorganic upper airwayFunctional syndromes obstructionBenign central airway stenosisLung transplantationInfectionCongenital lesionsTracheobronchial malaciaAcquired immunodeficiency syndromeExternal compression from benignmediastinal masses or fibrosis
One or more of the following diagnostic maneuvers should be used if one or more previously mentioned clinical features appear and suggest a CAO [8]:
- •The standard chest roentgenograms with careful inspection of tracheal air shadow.
- •Tracheal tomograms.
- •CT scan of neck or chest with three-dimensional reconstruction.
- •Laryngoscopy.
- •Bronchoscopy.
- •Mediastinoscopy or mediastinotomy.
In our patient, chest roentgenograms and CT scans were the key to diagnosing the tumor. Then, an emergency bronchoscopy was performed.
A CT scan is the most useful radiological way to estimate tracheal tumors (size, site, extratracheal extension). However, bronchoscopy is the most important diagnostic tool for taking crucial information about the trachea, tumor location, and dimensions. Moreover, bronchoscopy allows us to take biopsies for tumor identification and to plan for surgical resection in consideration of all reservations that are needed in suspected CAO [1].
The endoscopic appearance of schwannoma can be well-circumscribed, round, raised, or smooth gray masses, and visible vessels or cystic areas can exist [9,12,13]. However, only microscopic characters can give an accurate diagnosis; typical dense and loose areas known as Antoni A and Antoni B areas respectively, Verocay bodies which are formed by central nuclear-free zones ramified by palisading nuclei, a characteristic spindled elongated nucleus with a wavy of buckled shape, thick-walled hyalinized blood vessels, axons absence, cystic changes, and S100 positivity, calretinin, basal lamina component (such as laminin and type IV collagen) as immunohistochemical features [12,13]. Hence, pathologic spindled cells can be excluded [Table 3]. [12,13,21]Table 3. The key histological differential diagnoses (DD) for schwannoma.Table 3. DiagnosisHistological FeaturesImmunohistochemistry (IHC)Key Distinguishing FeaturesNeurofibromaLoosely arranged spindle cells, wavy nuclei, myxoid background, unencapsulated, lacks Antoni A/B and Verocay bodies.S-100 positive (less diffuse than schwannoma)Not encapsulated, lacks biphasic patternMPNST (Malignant Peripheral Nerve Sheath Tumor)Highly cellular, atypia, high mitoses, necrosis, infiltrative growthSpindeled cells arranged in sweeping fascicles with variations in cellularityS-100 (focal/variable), SOX10 (+), H3K27me3 loss (often)Malignant features, patchy S-100, unencapsulatedLeiomyoma/LeiomyosarcomaIntersecting fascicles of spindle cells with eosinophilic cytoplasm and blunt-ended nuclei, increased mitoses, and necrosis in sarcomaSMA positive, Desmin positive, S-100 negativeSmooth muscle markers positive, different nuclear morphologyFibrosarcomaMalignant spindle cells in herringbone pattern, high mitotic rateVimentin positive, S-100 negativeHerringbone architecture, S-100 negativeSolitary Fibrous Tumor (SFT)Patternless pattern of spindle cells, prominent branching (“staghorn”) vesselsCD34 positive, CD99 positive, STAT6 nuclear positive, S-100 negativeSTAT6 nuclear positivity is diagnosticSpindle Cell MelanomaSpindle cells may mimic schwannoma, sometimes pigmentedS-100 positive, HMB-45 positive, Melan-A positive, SOX10 positiveMelanocytic markers (HMB-45, Melan-A) distinguish itInflammatory Myofibroblastic Tumor (IMT)Spindle cells in myxoid or collagenous stroma, mixed inflammatory infiltrateALK positive (often), SMA positive, S-100 negativeInflammatory background, ALK+, no Antoni/Verocay bodiesMeningiomaWhorled cell pattern, psammoma bodies, with intersecting fascicles of spindled cellsEMA positive, S-100 negative, or focalWhorls and psammoma bodies, EMA+, lack encapsulation
It is noteworthy to highlight other useful steps for forming an early diagnosis to exclude confusion between asthma and CAO: PFTs as an essential step, Spirometry (sensitive for quantifying airway obstruction), and Flow-volume loop (more beneficial in CAO recognition) [Fig. 7] [8,22]. The emergency status of our patient was unable to perform pulmonary function testing.Fig. 7. Flow volume loops; flattening of the inspiratory limb in extrathoracic airflow obstruction; flattening of the expiratory limb in intrathoracic airflow obstruction; obvious reduction in inspiratory and expiratory flows in asthma.Fig. 7
The appropriate choice of treatment should consider the risk of tracheal resection, the tumor's clinical findings, size, shape (pedunculated or sessile), whether an extratracheal component is present, or whether it is a completely intraluminal tumor, as well as the patient's cardiopulmonary function [17,23].
The standard treatment of benign PTT and intermediate aggressiveness is surgical resection with reconstruction of the airway, which is also the optimal procedure for patients with huge and sessile schwannomas [1,17,24]. Other methods to treat tracheal schwannoma include electrocautery snaring, argon plasma coagulation, cryotherapy, endoscopic excision, and microdebridement [Table 4] [17,25]. In addition, an endoscopic laser has successfully managed benign PTT, like schwannoma, and it is what we used in our case, combined with large biopsy forceps, as it was the best option because of the large tumor (95 %), tracheal obstruction, and high vascularity. [10,26,27]Table 4. Other methods to treat tracheal schwannoma.Table 4. Technique LaserElectrocauteryMechanical DebulkingCryotherapyMechanismDehydration Deep coagulationSuperficial cauterization.Cutting.Physical removal using forceps.Destroy tissue by freezing.Efficacy in tumorsVascular/deep tumorsSmall/medium lesions.After laser or electrocautery to remove the remainsAdjunct for devitalized tissueSpeed of actionFastFast to moderateDepends on tumor size and textureSlow(may require multiple sessions)Bleeding riskLowModerateModerate to high if used alone.LowRisk of airway fireHigh (with O2 > 40 %)HighNoneNoneThe best role in multimodal managementVascular tumorsSoft/mucoid lesionsUsed to clean/remain patentPost-thermal for healing
Laser resection has been used increasingly over the last decade without significant morbidity, and Nd-YAG laser should be considered first-line therapy in benign endobronchial tumors within certain conditions: strictly endoluminal, low recurrence possibility, the limited extent within the endobronchial tree, recent lobe/lung collapse, symptomatic airway compromise, and poor surgical risks [9,10]. Prognosis outcomes of different types of lasers are shown in [Table 5] [28]. Bronchoscopic surveillance is highly recommended for remote recurrence if the resection is incomplete. Thus, surgery should be chosen for local recurrence [9,10,17].Table 5. Prognosis outcomes of different types of lasers.Table 5. Nd:YAG LaserCO2 LaserDiode Laser:Benign pedunculated neoplasms-Deep breakthrough.-Ideal.-Very accurate.-Minimal thermal damage.-Surface cutting._Benign sessile neoplasmsIn case of deeper tissue impact is needed (the used care).-Minimal damage.-Superficial ablation._Malignant neoplasms-First-line.-Good coagulation.-Palliative debulking.Superficial only.Similar coagulation to Nd:YAG.
Using rigid equipment enhances the surgeon's ability to remove a tumor more rapidly in combination with laser coagulation. The flexible bronchoscope is then passed through the rigid resection scope to permit the use of the Nd: YAG laser to complete the debridement and obtain hemostasis [29].
Our case emphasizes that rigid bronchoscopy with Nd-YAG laser resection was a very successful tool for managing schwannoma, and Bronchoscopic surveillance showed No Recurrence as the benign nature of the schwannoma without an extratracheal component. The work has been reported in line with the SCARE criteria [30].
Conclusion
4
Awareness of the possibility of schwannoma as a primary tracheal tumor is important, although it is phenomenal, it can make pseudo-asthmatic status because it has non-specific symptoms (persistent cough, whizzing, dyspnea) that are not relieved by bronchodilators and may cause CAO. Therefore, Spirometry, PTFs, CT, and bronchoscopy should be performed to make the correct diagnosis. Treatment choice depends on the tumor's clinical findings, size, shape (pedunculated or sessile), extratracheal component, and the patient's condition. Skilled recognition of the endoscopic appearance is necessary. Rigid bronchoscopy with Nd-YAG laser resection is a successful tool for managing schwannoma. However, long-term follow-up after tumor resection is required.
CRediT authorship contribution statement
RN contributed to drafting, reviewing, editing and approved the final manuscript.
RA contributed to drafting, reviewing, editing and approved the final manuscript.
BI contributed to drafting, reviewing, editing and approved the final manuscript.
SHcontributed to drafting, editing and approved the final manuscript.
AA contributed to drafting, reviewing, editing, corresponding, and approved the final manuscript.
NA contributed to reviewing, supervising and approved the final manuscript.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval is not required for this type of publication.
Guarantor
All authors have read and approved the manuscript, on behalf of all the contributors I will act and guarantor and will correspond with the journal from this point onward.
Sources of funding
Not applicable.
Declaration of competing interest
Not applicable.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sammartino F.Macchiarini P.Primary tracheal tumors Lung Cancer 2014 Wiley 26727710.1002/9781118468791.ch 17 · doi ↗
- 2Al-Qadi M.O.Artenstein A.W.Braman S.S.The “forgotten zone”: Acquired disorders of the trachea in adults Respir. Med.1072013130113132366941310.1016/j.rmed.2013.03.017PMC 7125950 · doi ↗ · pubmed ↗
- 3Hamdan A.L.Moukarbel R.V.Tawil A.El-Khatib M.Hadi U.Tracheal schwannoma: a misleading entity Middle East J. Anaesthesiol.20201061161320394267 · pubmed ↗
- 4Xu L.-T.Clinical and pathologic characteristics in patients with tracheobronchial tumor: report of 50 patients Ann. Thorac. Surg.431987276278382737010.1016/s 0003-4975(10)60611-x · doi ↗ · pubmed ↗
- 5Lina G.Tracheobronchial schwannoma: a case report and literature review J. Int. Med. Res.512023300060522114989110.1177/03000605221149891 PMC 989308036708207 · doi ↗ · pubmed ↗
- 6Weinberger M.Abu-Hasan M.Pseudo-asthma: when cough, wheezing, and dyspnea are not asthma Pediatrics 12020078558641790877310.1542/peds.2007-0078 · doi ↗ · pubmed ↗
- 7Righini C.A.Lequeux T.Laverierre M.-H.Reyt E.Primary tracheal schwannoma: one case report and a literature review Eur. Arch. Otorhinolaryngol.26220051571601506083110.1007/s 00405-004-0778-0 · doi ↗ · pubmed ↗
- 8Lillington G.A.Faul J.L.Differential diagnosis of asthma in adults Bronchial Asthma 2001 Humana Press Totowa, NJ 13715310.1007/978-1-59259-127-5_6 · doi ↗