Multigenerational thyroid hormone resistance due to THRβ mutation
Stylianos Kopanos, Joachim Feldkamp

TL;DR
A rare genetic mutation in the THRβ gene causes thyroid hormone resistance with severe heart problems requiring a heart transplant.
Contribution
Highlights the underrecognized cardiac manifestations of thyroid hormone resistance and emphasizes the need for early diagnosis.
Findings
A THRβ mutation caused progressive heart failure unresponsive to standard treatment.
The mutation followed an autosomal dominant pattern across multiple family members.
Thyroidectomy and levothyroxine therapy complicated management in this case.
Abstract
Resistance to thyroid hormone (RTH) is a rare genetic disorder caused by mutations in the thyroid hormone receptors α or β (THRα, THRβ) genes, leading to impaired tissue responsiveness to thyroid hormones. While its systemic effects are well-documented, the cardiac manifestations of RTH, including hypertrophic and dilated cardiomyopathy (DCM), arrhythmias, and heart failure, are often underrecognized, particularly in cases of treatment refractory heart failure. This case report aims to highlight the importance of cardiological awareness in diagnosing and managing RTH-related cardiomyopathy. We report the case of a 50-year-old Caucasian female with a confirmed variant c.1357C > A, p.P453T mutation in the THRβ gene, presenting with recurrent goitre, hypothyroidism, and progressive cardiovascular complications. Her clinical course was marked by episodes of angina-like symptoms, atrial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
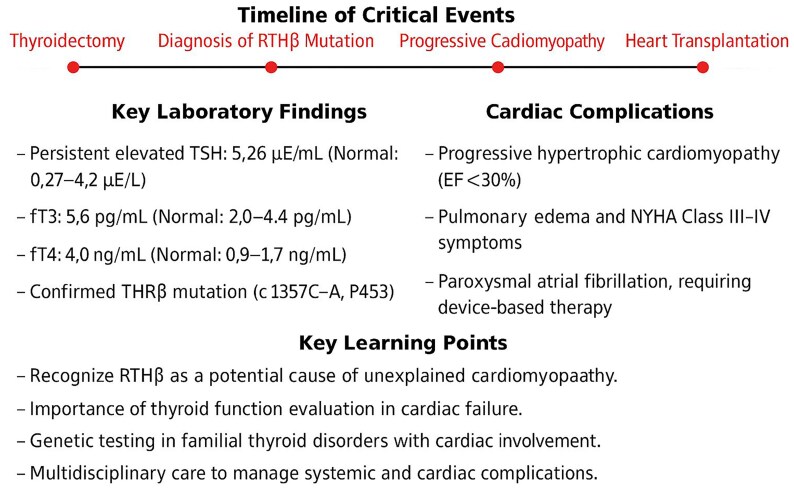 Figure 1
Figure 1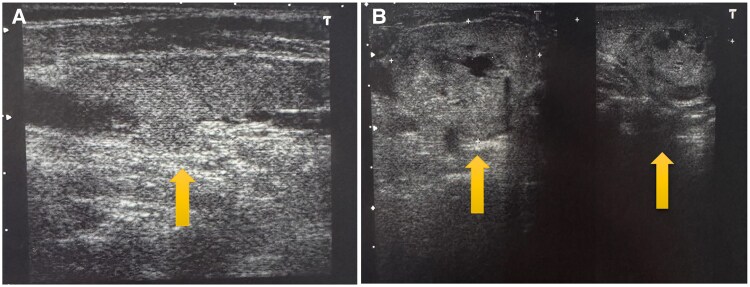 Figure 1
Figure 1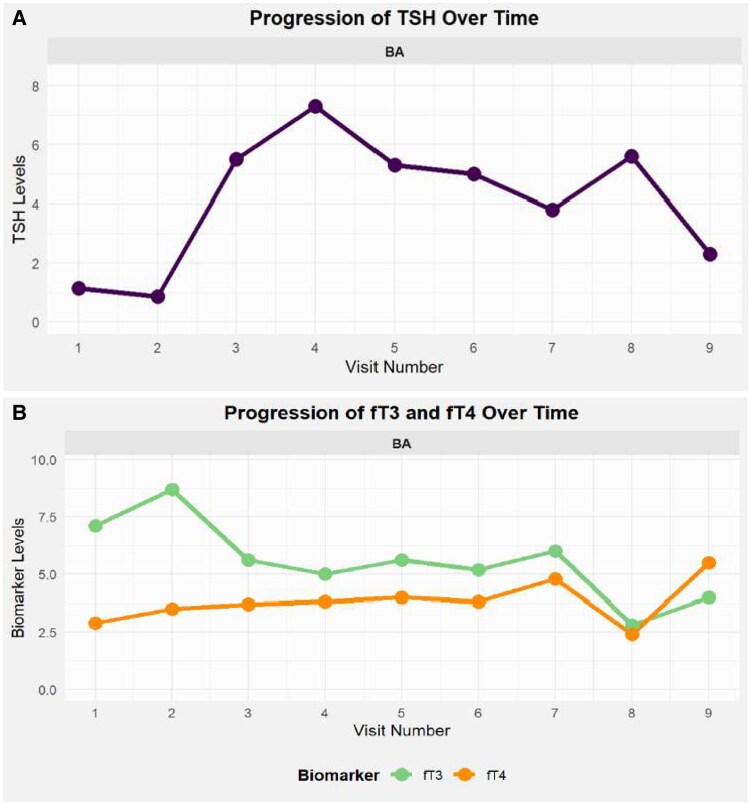 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Ion channel regulation and function · Thyroid Cancer Diagnosis and Treatment
Introduction
Resistance to thyroid hormone (RTH) results from mutations that impair thyroid hormone receptor (THR) function, classified as a syndrome of reduced thyroid hormone (TH) sensitivity. It disrupts TH transport, metabolism, and receptor signalling. TH acts through receptor isoforms encoded by the THRα and THRβ genes. Loss-of-function or dominant-negative mutations in these genes impair thyroid-stimulating hormone (TSH) signalling, causing resistance.^1^
Resistance to thyroid hormone manifests with elevated free thyroxine (fT4) and free triiodothyronine (fT3) levels and unsuppressed TSH. The condition, occurring in approximately 1 in 40 000 individuals, is associated with goitre, growth delays, cognitive impairments, and cardiac arrhythmias. Diagnosis is often delayed due to its nonspecific symptoms.^2,3^
Management aims to normalize TSH and maintain an euthyroid state, with genetic counselling for affected families.^4^ Selective thyromimetic analogues can bypass receptor mutations but must be carefully monitored to avoid overactivation of TRα and cardiac issues.^5^ Here, we describe the case of a 50-year-old woman with a heterozygous THRβ c.1357C > A, p.P453T mutation, confirmed in multiple first-degree relatives, leading to severe cardiovascular complications, including hypertrophic cardiomyopathy and heart failure, ultimately requiring heart transplantation. This case emphasizes the need for incorporating thyroid-related history into cardiological evaluations.
Summary figure
**
Case presentation
A 50-year-old woman was referred for persistent hypothyroidism, presenting with fatigue, cold intolerance, weight gain, and depressive symptoms. She had undergone a thyroidectomy 2 years earlier for obstructive goitre and was on levothyroxine therapy. Physical examination was unremarkable, but family history revealed thyroid hormone resistance in her mother and brother. Her brother had restrictive cardiomyopathy, arrhythmias, and died shortly after heart transplantation, while her mother exhibited atrial fibrillation and hypertension.
Investigations revealed elevated TSH (5.26 μE/mL; normal: 0.27–4.2 μE/mL), fT3 (5.6 pg/mL; normal: 2.0–4.4 pg/mL), and fT4 (4.0 ng/mL; normal: 0.9–1.7 ng/mL) despite levothyroxine therapy. Autoimmune markers were normal, and neck ultrasound showed patchy hypoechoic parenchyma. Thyroid scintigraphy revealed 2.4% technetium uptake with no nodules. Genetic testing confirmed a heterozygous THRβ c.1357C > A, p.P453T mutation.
Over subsequent years, the patient experienced angina-like symptoms, panic attacks, and heart failure, necessitating hospitalization for pulmonary oedema, left ventricular dysfunction (EF < 30%), and pericardial effusion. She underwent a second thyroidectomy for recurrent goitre, with an uneventful postoperative course (Figure 1). However, inadequate levothyroxine replacement led to weight gain, requiring initiation of liothyronine (Teatrois) at 30 mcg/day alongside levothyroxine (Figure 2).
(A,B). Recurrent goitre identified liquefaction and calcifications. Images before and after thyroidectomy.
(A,B). Dynamic progression of TSH, fT3 and fT4 values over time.
Despite treatment, the patient developed progressive dilated cardiomyopathy, dialysis- dependent renal failure, and NYHA Class III-IV heart failure, leading to frequent hospitalizations. Orthotopic biatrial heart transplantation was performed, with no evidence of graft rejection. Post-transplant, thyroid hormone therapy was adjusted to levothyroxine 200 μg/day, while liothyronine was discontinued. Immunosuppressive therapy included tacrolimus, mycophenolate mofetil, and prednisolone. Secondary adrenal insufficiency was identified (ACTH: 4.7 pg/mL, cortisol: 32.2 μg/L).
The patient’s two sons were genetically tested, confirming TSHβ mutations. Both exhibited symptoms of hyperthyroidism and nodular goitre but discontinued follow-up care.
Discussion
Thyroid hormones regulate myocardial contractility, vascular resistance, and metabolism. In RTH, particularly with THRβ mutations, hormone resistance leads to selective cardiac effects as THRα, expressed in the heart, remains functional. This causes a hyperthyroid state in cardiac tissues, promoting hypertrophy, arrhythmias, and heart failure.^6^
Excess thyroid hormone activity increases sarcoplasmic reticulum Ca²⁺ ATPase activity, predisposing patients to arrhythmias like atrial fibrillation.^7,8^ Simultaneously, impaired calcium reuptake and titin phosphorylation reduce myocardial contractility and relaxation, contributing to diastolic dysfunction and pulmonary congestion.^9,10^ Over time, these processes drive cardiac remodelling, transitioning from hypertrophic to dilated cardiomyopathy due to energy depletion and fibrosis.^11^
Genetic variability affects RTHβ presentation within families, with differences in mutation expression, severity of hormone resistance, and compensatory mechanisms.^12^ Thyroid hormone analogues like triiodothyroacetic acid bypass receptor mutations and reduce cardiac remodelling but require careful monitoring to avoid exacerbating systemic effects.^4^
Management involves balancing levothyroxine therapy while preventing cardiac overstimulation. Regular monitoring of thyroid function, echocardiography, and cardiac MRI is critical. Anti-arrhythmic therapies, beta-blockers, and RAAS inhibitors are often needed to stabilize cardiac status. In severe cases like this, heart transplantation offers the only viable solution but introduces challenges, including immunosuppressive therapy interactions with thyroid hormones.^13,14^
Conclusion
This case highlights the significant cardiovascular impact of RTHβ, emphasizing the need for its consideration in treatment-resistant cardiomyopathy. Importantly, it underlines the critical role of early diagnosis: prompt identification of thyroid hormone resistance could enable earlier therapeutic interventions, potentially preventing the development of severe cardiac remodelling, arrhythmias, and heart failure.
Incorporating routine thyroid function screening and detailed family history analysis into the diagnostic workup of unexplained cardiomyopathy could significantly improve outcomes. Recognizing elevated thyroid hormone levels with non-suppressed TSH should prompt genetic evaluation for RTHβ, particularly in the presence of cardiac symptoms. Early multidisciplinary intervention combining endocrine, cardiological, and genetic expertise can prevent disease progression and reduce the need for advanced interventions such as heart transplantation.
Increased clinical awareness of this underdiagnosed syndrome will foster earlier detection, personalized management, and better long-term prognoses for affected patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Concolino P, Costella A, Paragliola RM. Mutational landscape of Resistance to Thyroid Hormone Beta (RTHβ). Mol Diagn Ther 2019;23:353–368.30976996 10.1007/s 40291-019-00399-w · doi ↗ · pubmed ↗
- 2Grasberger H, Refetoff S. Resistance to thyrotropin. Best Pract Res Clin Endocrinol Metab 2017;31:183–194.28648507 10.1016/j.beem.2017.03.004PMC 5569899 · doi ↗ · pubmed ↗
- 3Khan K, Moriwala A, Siddiqui Z. Thyroid hormone resistance with a novel mutation. Cureus 2024;16:e 72898.39624568 10.7759/cureus.72898 PMC 11611320 · doi ↗ · pubmed ↗
- 4Pappa T, Refetoff S. Resistance to thyroid hormone Beta: a focused review. Front Endocrinol 2021;12:656551.10.3389/fendo.2021.656551 PMC 804468233868182 · doi ↗ · pubmed ↗
- 5van Gucht ALM, Moran C, Meima ME, Visser WE, Chatterjee K, Visser TJ, et al Resistance to thyroid hormone due to heterozygous mutations in thyroid hormone receptor alpha. Curr Top Dev Biol 2017;125:337–355.28527577 10.1016/bs.ctdb.2017.02.001 · doi ↗ · pubmed ↗
- 6Illouz F, Briet C, Mirebeau-Prunier D, Bouhours-Nouet N, Coutant R, Sibilia P, et al Cardiac complications of thyroid hormone resistance syndromes. Ann Endocrinol 2021;82:167–169.10.1016/j.ando.2020.03.00832513415 · doi ↗ · pubmed ↗
- 7Moran C, Chatterjee K. Resistance to thyroid hormone due to defective thyroid receptor alpha. Best Pract Res Clin Endocrinol Metab 2015;29:647–657.26303090 10.1016/j.beem.2015.07.007PMC 4559105 · doi ↗ · pubmed ↗
- 8Biondi B . The management of thyroid abnormalities in chronic heart failure. Heart Fail Clin 2019;15:393–398.31079697 10.1016/j.hfc.2019.02.008 · doi ↗ · pubmed ↗