Cherry-Pit Perforation of an Ileocecal Diverticulum: A Case Report
Yoichi Miyaoka, Shingo Shimada, Kazuhiro Ogasawara, Akinobu Taketomi

TL;DR
A man experienced severe abdominal pain due to a cherry pit perforating a pseudodiverticulum, highlighting the rare but serious risk of fruit seeds causing bowel injury.
Contribution
This case report adds to the understanding of seed-induced colonic perforation and its diagnostic challenges.
Findings
A cherry pit was found to have perforated a pseudodiverticulum in the ileocecal region.
Right-sided pseudodiverticula are more common in Asian populations and lack a muscularis layer.
Imaging features like hyperdense intraluminal objects can help differentiate this condition from cancer or inflammation.
Abstract
Seed-induced colonic perforation is exceptionally rare but may mimic malignancy or complicated diverticulitis, leading to diagnostic challenges. We report the case of a middle-aged man who presented with acute right lower quadrant abdominal pain. Contrast-enhanced computed tomography (CT) revealed mural thickening and a target-like lesion at the ileocecal junction, raising suspicion for intussusception or carcinoma. Emergency surgery identified a cherry pit perforating a pseudodiverticulum in the ileocecal region. This case highlights the potential for hard fruit seeds to cause full-thickness bowel injury, especially in right-sided pseudodiverticula, which are more prevalent in Asian populations and lack a protective muscularis layer. Characteristic imaging features, such as hyperdense intraluminal objects with surrounding inflammation, can assist in differentiating these cases from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
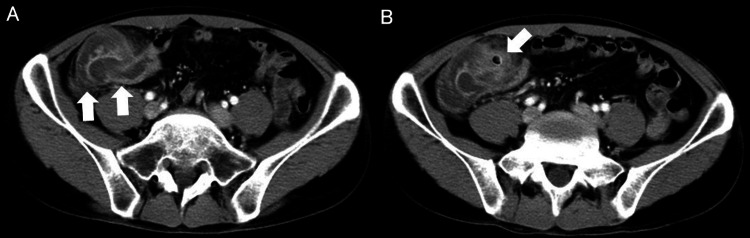 Figure 1
Figure 1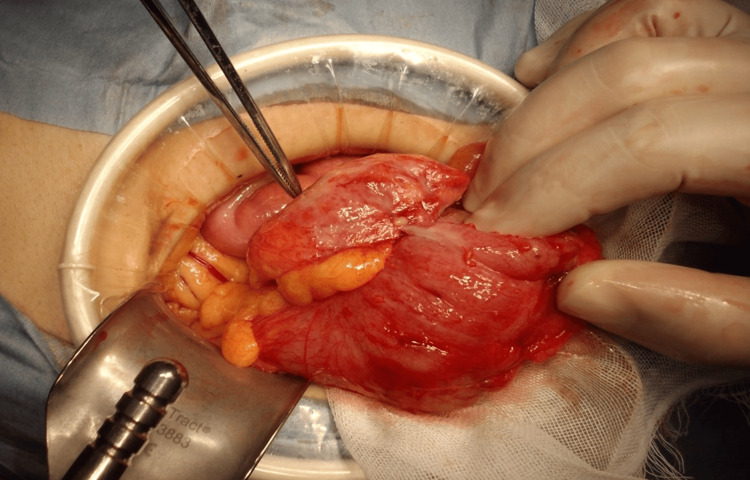 Figure 2
Figure 2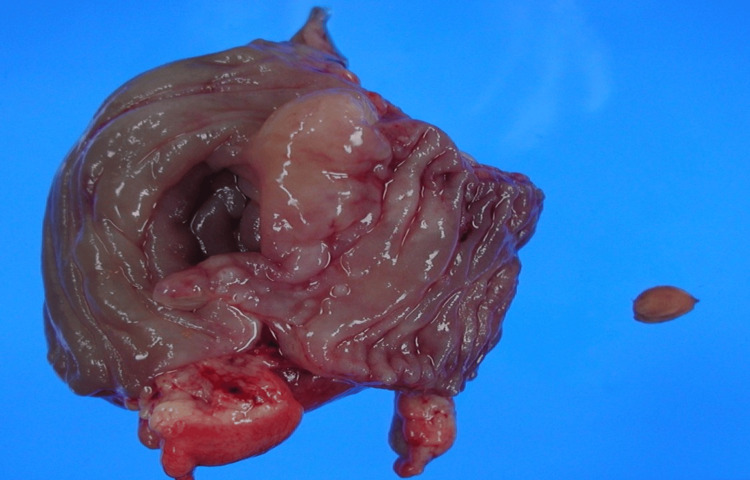 Figure 3
Figure 3| Year | Study | Seed/pit | Site | Presentation → management | Outcome | Age/sex | Country |
| 1999 | Fujikawa et al. [ | Pickled-plum seed | Cecum | Perforated peritonitis → segmental colectomy | Survived | NR | Japan |
| 2005 | Otani et al. [ | Persimmon × 5 | Cecum + ascending colon | Large-bowel obstruction → emergency R-hemicolectomy | Discharged POD 26 | 82 years/male | Japan |
| 2006 | Ashida et al. [ | Pickled-plum seed | Ascending-colon cancer ulcer | Ileus → right hemicolectomy | Uneventful | 78 years/female | Japan |
| 2008 | Yamaguchi et al. [ | Watermelon and corn seeds (multiple) | Ascending colon | Seed-bezoar ileus → right hemicolectomy | Discharged POD 23 | 71 years/male | Japan |
| 2011 | Puia et al. [ | Multiple fruit stones | Ascending colon | Perforation → right hemicolectomy | Uneventful | Two cases/NR | Romania |
| 2016 | Gupta et al. [ | Plum seed | Terminal ileum | Perforation in hernia → ileocecal resection | Well | 11 months/male | India |
| 2025 | Present case | Cherry pit | Ileocecal | Ileocecal perforation → ileocecal resection | Discharged POD 5 | 46 years/male | Japan |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiverticular Disease and Complications · Gastrointestinal disorders and treatments · Esophageal and GI Pathology
Introduction
Foreign-body ingestion is common, yet less than 1% of objects cause perforation [1]. Fish bones dominate such injuries, whereas fruit seeds are rarely implicated. Seeds become hazardous when they lodge at anatomical narrows or within diverticula and are exposed to propulsive peristalsis [2,3]. The sigmoid colon is classically affected, but right-sided lesions are increasingly recognized in regions with prevalent right-colon diverticulosis. Notably, the prevalence of colonic diverticulosis varies by geography: while left-sided diverticula are more common in Western populations, right-sided diverticula predominate in East Asian countries, where prevalence among adults can exceed 20% [4,5]. We present a case of cherry-pit perforation of an ileocecal diverticulum and summarize recently reported seed-related large-bowel complications.
Case presentation
A 46-year-old man with chronic low back pain managed by regular nonsteroidal anti-inflammatory drugs (NSAIDs) and no history of abdominal surgery presented with a two-day history of progressively worsening colicky pain in the right iliac fossa. The pain persisted despite his ingestion of a greater-than-usual dose of NSAIDs. He denied nausea and vomiting. On arrival at our hospital, his vital signs were stable. Abdominal examination revealed marked tenderness with rebound in the right lower quadrant. Laboratory investigations showed a white-blood-cell count of 21 × 10³/µL and a C-reactive protein level of 9.12 mg/dL.
Contrast-enhanced abdominal computed tomography (CT) revealed concentric mural thickening at the ileocecal junction, surrounding fat stranding, and a target configuration consistent with intussusception. A discrete intraluminal hyperdense focus, slightly denser than bowel contents, was present but not definitively characterized or diagnosed (Figure 1).
Abdominal CT. (A) Contrast-enhanced CT shows ileocolic intussusception with concentric mural thickening of the terminal ileum and cecum and surrounding inflammatory fat stranding (arrows). (B) An intraluminal structure with a centrally hypoattenuating core and hyperattenuating rim is visible (arrow)CT: computed tomography
Emergency midline laparotomy uncovered dense inflammatory adhesions around the cecum (Figure 2).
Intraoperative photograph demonstrating marked inflammation and adhesions around the cecum, with telescoping (intussusception) of the adjacent bowel
Several small pseudodiverticula were identified on the antimesenteric border; one diverticulum was perforated by an oval brown cherry pit measuring 13 × 10 mm, which extended into the mesentery (Figure 3).
Resected ileocecal specimen with a 13 × 10 mm cherry pit lodged in a perforated pseudodiverticulum and surrounding acute serositis
An ileocecal resection with side-to-side stapled anastomosis was completed. Oral intake was resumed on postoperative day 3, and the patient was discharged on day 5. Postoperative dietary questioning revealed that he had swallowed whole cherries one week before admission.
Discussion
This case underscores that even a small cherry pit can precipitate a life-threatening perforation of the right colon. Three pathophysiologic mechanisms appear to be involved. First, the pit’s rigid, lignin-rich shell withstands enzymatic degradation, and its microscopic ridges mechanically abrade the intestinal mucosa [6]. Second, after dehydration, the pit absorbs intraluminal fluid and swells in situ; its rough surface facilitates bacterial adherence, thereby amplifying local inflammation and ischemia [2,7]. Third, once the impacted pit lodges within a false diverticulum lacking muscularis propria, peristaltic forces exert focal pressure that can culminate in full-thickness necrosis and perforation [8].
Recent case reports (Table 1) [6,9-13] indicate that seed-related colonic complications can also arise in the right colon, particularly in Asian populations. This predominance reflects both the high prevalence of cecal and ascending colon diverticulosis in these populations and regional dietary habits that include the consumption of seed-containing fruits. Although the right colon has a wider lumen, its thinner wall can rapidly fail when a hard seed becomes impacted in a false diverticulum; peristaltic compression then produces focal necrosis and full-thickness perforation, explaining the dramatic presentations observed.
Fruit seeds may exhibit mixed attenuation on CT, with the dense outer shell appearing hyperattenuating (approximately 100-300 Hounsfield units) and the hollow or pulp-deficient core appearing hypoattenuating. Such findings can be mistaken for stool or contrast material, but bone window settings and multiplanar reconstructions aid in accurate identification [14]. Host factors also modulate risk: in this case, the patient had been taking NSAIDs regularly. Previous reports, including a case of a solitary cecal ulcer that resolved after discontinuation of loxoprofen [15], as well as several cases of ileocecal ulceration or stenosis associated with long-term NSAID use [16], suggest that chronic loxoprofen therapy can compromise mucosal integrity in the terminal ileum to the ascending colon. Therefore, it is possible that long-term loxoprofen use in this patient contributed to intestinal wall fragility, facilitating seed impaction and subsequent perforation. Therefore, chronic NSAID therapy, impaired mastication, and consuming fruits without removing their seeds are risk factors for seed impaction that can lead to obstruction or perforation in patients with right-sided colonic diverticulosis, especially in populations where large fruit pits or seeds are commonly eaten.
Conclusions
Cherry pits lodged in the ileocecal pseudodiverticula can cause acute perforation that mimics intussusception or carcinoma. Accurate CT interpretation and prompt surgery are pivotal for favorable outcomes; in particular, clinicians should remain vigilant for seed-related perforations throughout the colon, especially in regions where right-sided diverticulosis predominates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies World J Surg Goh BK Chow PK Quah HM Ong HS Eu KW Ooi LL Wong WK 3723773020061647933710.1007/s 00268-005-0490-2 · doi ↗ · pubmed ↗
- 2Gastrointestinal seed bezoars: a systematic review of case reports and case series Cureus Manatakis DK Acheimastos V Antonopoulou MI Balalis D Korkolis DP 011201910.7759/cureus.4686 PMC 663669731333915 · doi ↗ · pubmed ↗
- 3Harry Potter's occlusion: report of a case of pumpkin seed bezoar rectal impact Front Surg Gentile M Vergara L Schiavone V Cestaro G Sivero L 902701920223591047510.3389/fsurg.2022.902701 PMC 9329672 · doi ↗ · pubmed ↗
- 4Right colonic diverticulitis J Korean Soc Coloproctol Lee IK 2412452620102115222410.3393/jksc.2010.26.4.241PMC 2998007 · doi ↗ · pubmed ↗
- 5Epidemiology, pathophysiology, and treatment of diverticulitis Gastroenterology Strate LL Morris AM 1282129815620193066073210.1053/j.gastro.2018.12.033PMC 6716971 · doi ↗ · pubmed ↗
- 6"Pseudo-phytobezoar" due to seed from pickled plum resulting in perforated peritonitis Am J Gastroenterol Fujikawa T Matsusue S Nishimura S Takakuwa H 3373337494199910.1111/j.1572-0241.1999.3373 a.x 10566753 · doi ↗ · pubmed ↗
- 7Cocoa seeds as a phytobezoar causing intestinal obstruction in a Ghanaian child: a case report Cureus Nsoh LN Asiedu-Asante AK Yakubu HA Nyame K 016202410.7759/cureus.76562 PMC 1177463839881926 · doi ↗ · pubmed ↗
- 8Gastrointestinal perforation: clinical and MDCT clues for identification of aetiology Insights Imaging Pouli S Kozana A Papakitsou I Daskalogiannaki M Raissaki M 311120203208662710.1186/s 13244-019-0823-6PMC 7035412 · doi ↗ · pubmed ↗