Perineal endometriosis on an episiotomy scar: diagnosis based on clinical, radiological, and hormonal criteria (case report)
Abdoulrazak Egueh Nour, Chirwa Mahamoud Abdillahi, Samia Bennani, Ahmed Hared Bouh, Bouknani Nawal, Amal Rami

TL;DR
A rare case of perineal endometriosis following an episiotomy is diagnosed using clinical, radiological, and hormonal evidence in a 36-year-old woman.
Contribution
This case report highlights the under-recognized possibility of perineal endometriosis after episiotomy and its successful management with hormonal therapy.
Findings
Clinical and imaging features, along with response to hormonal therapy, supported a diagnosis of perineal endometriosis.
The patient experienced significant symptom improvement with hormonal treatment, avoiding surgery.
Perineal endometriosis should be considered in women with cyclical perineal pain following episiotomy.
Abstract
Endometriosis is a chronic, non-cancerous gynecological disorder that is typically observed in women of fertile age. It describes the presence of functional endometrial components, glands and stroma outside the endometrial cavity, most often involving pelvic structures such as the ovaries, peritoneum, and uterine ligaments. Perineal endometriosis is a rare form of extrapelvic endometriosis, with an estimated incidence of between 0.3% and 1%. We report the case of a 36-year-old woman, gravida 1 para 1(G1P1), with a history of vaginal delivery and no known history of endometriosis, who presented with a painful mass located on the right perineal scar two years after undergoing a mediolateral episiotomy. The mass was associated with cyclical pain and significantly impaired quality of life. Clinical examination, combined with ultrasound and Magnetic Resonance Imaging (MRI), suggested the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
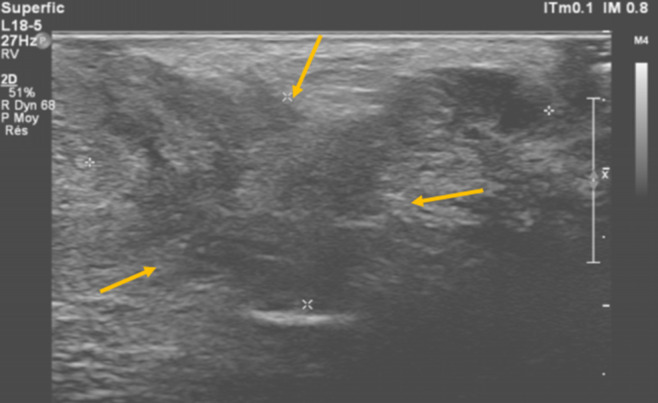 Figure 1
Figure 1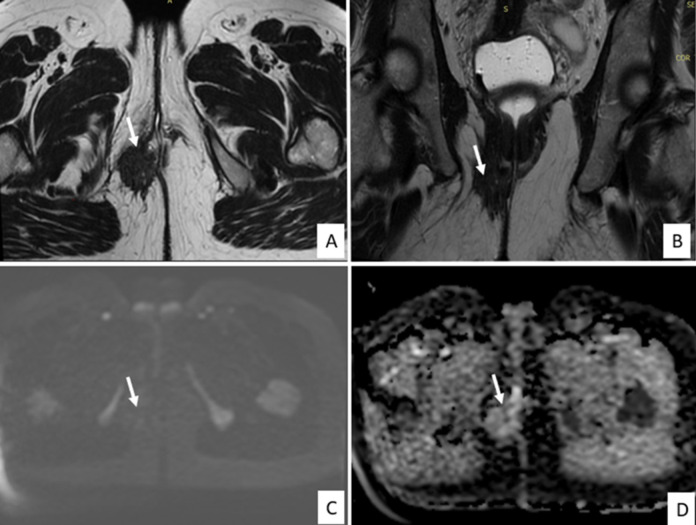 Figure 2
Figure 2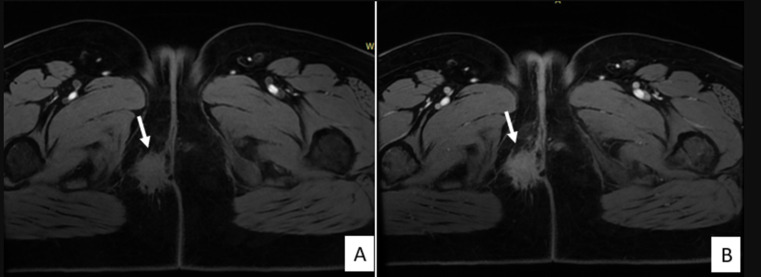 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndometriosis Research and Treatment
Introduction
Endometriosis is a relatively frequent condition in women of reproductive age, with a reported prevalence of 10% to 20% [1]. It is characterized by the presence of functional endometrial tissue outside the uterine cavity, most commonly within the pelvic region. Extrapelvic locations, however, are rare, particularly perineal endometriosis affecting only 0.3% and 1% of women [2]. The classic diagnostic clinical trial for this condition includes a history of vaginal delivery with episiotomy, increasing cyclical perineal pain and a perineal mass located at the episiotomy scar [3]. The pathogenesis of perineal endometriosis remains unclear despite numerous theories. The leading hypothesis proposes that endometrial cells are directly implanted onto scar tissue following obstetric trauma [4].
Patient and observation
Patient information: a 36-year-old woman, gravida 1 para 1, with no known history of endometriosis, presented with a progressive right perineal mass localized at the site of a mediolateral episiotomy performed two years earlier during vaginal delivery.
Clinical findings: the patient reported cyclical perineal pain worsening during menstruation, without associated signs of inflammation, infection, or urinary symptoms. Several consultations with gynecologists over the previous months had failed to identify a cause, and symptoms significantly impacted her quality of life. Clinical examination revealed a firm, tender, non-inflammatory nodule at the episiotomy scar, with healthy surrounding skin and no fistula or discharge.
Timeline of current episode: the patient began experiencing right perineal pain six months before consultation, progressively worsening and becoming cyclical. Imaging investigations were performed eight months after symptom onset, leading to the initiation of hormonal therapy with a favorable clinical response.
Diagnostic assessment: high-resolution ultrasound revealed a 32 x 15 mm hypoechoic, heterogeneous, retractile mass within the episiotomy scar, with no color Doppler flow (Figure 1). Pelvic MRI showed a perineal mass with spiculated, retractile margins, isointense to muscle on T2-weighted images, containing focal T1 hyperintense areas on fat-suppressed sequences, and no contrast enhancement or diffusion restriction. The lesion measured 4 cm in height and 4 x 2 cm in axial diameter (Figure 2 and Figure 3). The uterus, ovaries, rectum, and bladder appeared normal, without signs of deep pelvic endometriosis (Figure 4). Laboratory tests, including inflammatory markers, were normal.
transperineal ultrasound revealed a heterogeneous hypoechoic mass in the right perineum, with retractile and irregular contours measuring 32x15mm (yellow arrows)
axial (A) and coronal (B) T2-weighted MR images demonstrating a right-sided perineal mass with irregular, stellate contours extending toward the posterolateral wall of the distal third of the vagina and infiltrating the subcutaneous fat; The lesion exhibits low signal intensity on T2-weighted sequences, interspersed with small hyperintense cystic foci; no diffusion restriction is observed on DWI and ADC images (C, D)
on the T1-weighted fat-suppressed sequence (A); the lesion appears isointense relative to skeletal muscle, containing small hyperintense foci; Axial post-contrast T1 fat-saturated image showing no enhancement after gadolinium injection (B)
the sagittal T2-weighted sequence revealed no evidence of deep infiltrating endometriosis or adenomyosis
Diagnosis: based on the typical clinical triad (cyclical pain, history of episiotomy, localized mass), characteristic imaging findings, and exclusion of alternative diagnoses, perineal endometriosis was strongly suspected.
Therapeutic interventions: the patient declined surgical management and opted for hormonal therapy with progestins.
Follow-up and outcome of interventions: clinical response was favorable, with significant improvement in symptoms and partial regression of the mass on physical examination. At the 8-month follow-up, no recurrence or complications were observed.
Patient perspective: the patient expressed satisfaction with the non-invasive management and relief of symptoms, and was informed of the possibility of recurrence and the need for long-term monitoring.
Informed consent: written informed consent was obtained from the patient for publication of this case report and accompanying images.
Discussion
Perineal endometriosis is an uncommon but well-defined form of extrapelvic endometriosis, initially described by Schickele in 1923 [3]. Its low incidence, estimated at approximately 0.06% in a retrospective study of 72 patients by Nominato et al. [5], and its frequent association with obstetric scars, particularly episiotomies, make it a singular entity that deserves attention in cases of painful perineal masses in women of reproductive age. Two pathophysiological mechanisms are traditionally described to explain the occurrence of this form of endometriosis: the direct transplantation of endometrial cells during surgical intervention, such as episiotomy, referred to as secondary perineal endometriosis [6], as in our patient´s case. The second mechanism is the lymphovascular dissemination of endometrial cells in cases without prior perineal trauma, known as primary perineal endometriosis [6]. Most reported cases involve patients with a history of episiotomy or obstetric-related perineal tear, with symptom onset varying from several months to years after the procedure, with a median of 30 months. It is essential to consider perineal endometriosis as a possible diagnosis in a young, fertile woman presenting with localized pain or a mass in the ano-perineal region. A retrospective study by Zhu et al. conducted on 36 cases, identified three essential diagnostic criteria with a 100% predictive value when all are present [7]: a history of episiotomy or prior perineal tear, a firm and tender mass at the perineal lesion, and cyclical pain with mass swelling during menstruation (as was the case for our patient).
This clinical profile is crucial for differentiating perineal endometriosis from other differential diagnoses, such as localized recurrent ano-perineal abscess, which presents as a fluctuating and recurrent perineal mass; suture granuloma, urethral cysts, or Bartholin gland cysts, and rarer conditions such as ano-perineal melanoma, which may present similarly [8]. Malignant transformation into clear cell carcinoma should be ruled out in cases of recurrent scar endometriosis [3].
The assessment of perineal endometriosis primarily relies on imaging techniques such as ultrasound and MRI [8], with computed tomography (CT) being generally less useful. Ultrasound, though less specific, is often used as an initial modality for detecting scar endometriosis and may reveal hypoechoic or heterogeneous lesions with internal echoes with size and shape variations [7]. Magnetic resonance imaging, the reference imaging modality, is essential for diagnosing and evaluating the local extent of endometriosis, allowing precise visualization of the endometriotic mass and excluding other deep pelvic or extrapelvic locations. In MRI, endometriosis on an episiotomy scar presents several characteristic aspects that vary depending on disease stage and infiltration extent. In our case, a fibrous thickening with T2 hypointensity and stellate retractile infiltration was observed [8]. Typical MRI characteristics include T1 and T2 hyperintensity without fat saturation, suggesting the presence of endometrial tissue.
In the absence of histological confirmation, the diagnosis in our patient was supported by the convergence of the typical clinical triad, evocative MRI features, and favorable hormonal therapy response. This approach is endorsed by several authors who acknowledge that in typical presentations, diagnosis may be presumed without surgical confirmation, especially when surgery is declined or contraindicated [9].
While surgical excision with clear margins remains the standard of care to minimize recurrence risk, selected cases may benefit from medical management [3]. Progestins or GnRH analogs can offer satisfactory symptom control [10]. In our case, hormonal therapy led to a marked clinical improvement, with pain resolution and mass reduction within a few months. The sustained favorable course over 8 months further supports the presumed diagnosis.
The lack of histological confirmation and surgery remains the main limitation of this case. The diagnosis is based on strong clinical and radiological presumption and therapeutic response, without definitive exclusion of alternative etiologies. This case underscores the importance of an integrated diagnostic approach when excision is not performed.
Conclusion
Perineal endometriosis should be suspected in women presenting with perineal pain that recurs in a cyclical pattern, particularly with a history of episiotomy or perineal tear. Early management and recognition of this rare pathology are essential to prevent potentially serious complications, such as deep invasion of adjacent structures or, in rare cases, malignant transformation. Although perineal endometriosis is rare, its management relies on strong clinical knowledge, judicious imaging use, and appropriate surgical treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vellido-Cotelo R Muñoz-González JL Oliver-Pérez M Rde la Hera-Lázaro C Almansa-González CPérez-Sagaseta Cet al Endometriosis node in gynaecologic scars: a study of 17 patients and the diagnostic considerations in clinical experience in tertiary care center BMC Womens Health 201515132578364310.1186/s 12905-015-0170-9PMC 4337097 · doi ↗ · pubmed ↗
- 2Chen N Zhu L Lang J Liu Z Sun D Leng Jet al The clinical features and management of perineal endometriosis with anal sphincter involvement: a clinical analysis of 31 cases Hum Reprod 2012 Jun 276162472242279310.1093/humrep/des 067 · doi ↗ · pubmed ↗
- 3Bindra V Reddy N Reddy CA Swetha P Alapati KV Nori M Recurrent perineal scar endometriosis: A case report Case Rep Womens Health 2022 Oct 1936 e 004573628124310.1016/j.crwh.2022.e 00457 PMC 9587519 · doi ↗ · pubmed ↗
- 4Liu Y Pi R Luo H Wang W Zhao X Qi X Characteristics and long-term outcomes of perineal endometriosis: A retrospective study Medicine (Baltimore)20209923 e 2063810.1097/MD.0000000000020638 PMC 730633332502046 · doi ↗ · pubmed ↗
- 5Nominato NS Prates LFVS Lauar I Morais J Maia L Geber S Endometriose de cicatriz cirúrgica: estudo retrospectivo de 72 casos Rev Bras Ginecol E Obstetrícia 2007294237
- 6Liang Y Zhang D Jiang L Liu Y Zhang J Clinical characteristics of perineal endometriosis: A case series World J Clin Cases 2021 Feb 1695103710473364416710.12998/wjcc.v 9.i 5.1037 PMC 7896645 · doi ↗ · pubmed ↗
- 7Zhu L Lang J Wang H Liu Z Sun D Leng Jet al Presentation and management of perineal endometriosis Int J Gynaecol Obstet 2009 Jun 105323021932911710.1016/j.ijgo.2009.01.022 · doi ↗ · pubmed ↗
- 8El Houss S Laasri K El Yousfi Z El Halfi I Nassar I Billah NM Isolated perineal endometriosis? Yes ... an exceptional location Radiol Case Rep 20231811402240253768066710.1016/j.radcr.2023.07.072PMC 10480675 · doi ↗ · pubmed ↗