Distal Abdominal Aortic Thrombus With Approximately Full Occlusion—A Case of Pre‐Endovascular Care in Resource‐Limited Settings
Hilary Chipongo, Abizer Sarkar, Esmail Sangey, Kishan Chudasama, Amar Swali, Shaffin Rajan

TL;DR
This case report describes a rare arterial emergency in a resource-limited setting where a patient's limb was saved using an intra-arterial infusion.
Contribution
The paper presents a novel case of successful intra-arterial papaverine use in managing a distal abdominal aortic thrombus.
Findings
Conservative thrombolytic treatments failed for the patient with a distal abdominal aortic thrombus.
Intra-arterial papaverine infusion successfully salvaged the patient's ischemic lower limb.
The case highlights challenges in managing vascular emergencies in resource-limited settings.
Abstract
Up‐to‐date management of a distal abdominal aortic thrombus is challenging as no dedicated guideline for treating this condition exists. In our setting, it is one of the rare arterial vascular emergencies that can lead to devastating consequences and an increase in patient morbidity or mortality. For this publication, we have a case report of an elderly female of Asian descent who failed multiple attempts of conservative management with thrombolytics but benefited from an intra‐arterial papaverine infusion to salvage her ischemic lower limb.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
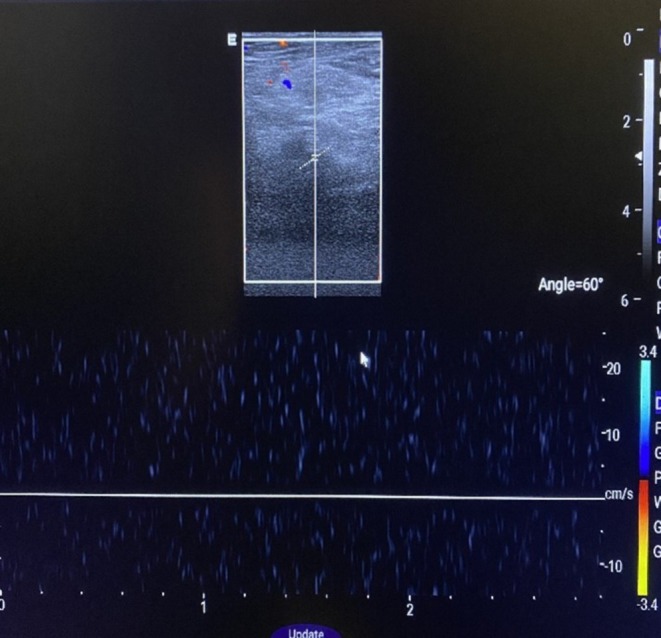 FIGURE 1
FIGURE 1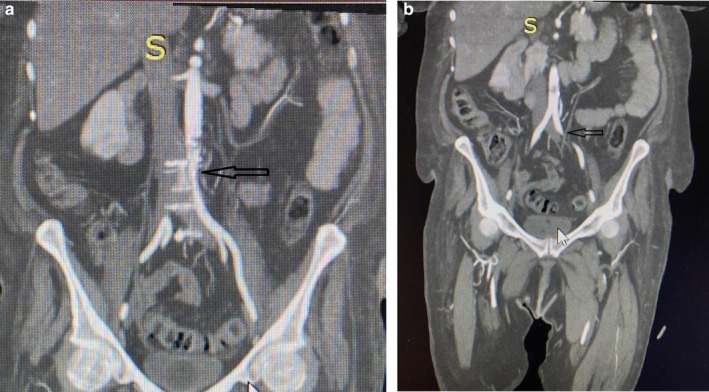 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Thrombus and Embolism · Aortic aneurysm repair treatments · Peripheral Artery Disease Management
Summary
- Aortic thrombus is a rare and life‐threatening condition.
- Few guidelines are proposed for its management, as few cases are reported in the literature.
- Herein we present a deadly occlusion of the distal abdominal aorta, which was managed conservatively as a pre‐endovascular care in a resource‐limited setting.
AbbreviationsAPTTactivated partial thromboplastin timeCT‐SCANcomputed tomography scanINRinternational normalized ratioMRImagnetic resonance imaging
Introduction
1
Distal abdominal aortic thrombus is one of the rare entities in cardiovascular pathologies [1], and being spontaneous makes it unique. Only a few cases are encountered in clinical practice; thus, it is rare to diagnose before the patient suffers embolic complications. This makes the true incidence of this particular disease unknown [2] and therefore a high index of suspicion in patients without risk of coagulability states or any previous risk factors predisposing them to thrombus formation should be thought of, especially in patients presenting with signs of lower extremity ischemia which may mimic signs of venous insufficiency due to deep vein thrombosis [3]. The management guidelines for this condition are still lacking as there is no clear consensus on whether conservative pharmacological versus endovascular surgery is the best option [3]. These guidelines are referenced from developed countries, which possess the full availability of resources and equipment, as opposed to our medical setting. In this case, we present a 69‐year‐old female of Asian descent who was diagnosed with distal aortic occlusion of approximately more than ninety percent (90%) and was managed with intra‐arterial papaverine and streptokinase infusion before being referred for endovascular therapy to salvage the limb.
Case Presentation
2
A 69‐year‐old female patient of Asian descent presented to the emergency department with a complaint of sudden onset of left calf pain approximately 12 h before admission. Upon further inquiry, she also reported having experienced numbness in her left lower limb, which was progressively worsening in the past 4 days before admission. Her only reported chronic comorbidity was Type 2 diabetes mellitus, for which she was on regular oral medications. On physical examination at the emergency department, she had a positive Homan's sign, dorsiflexion of the left foot produced significant calf pain, and dorsalis pedis and posterior tibial pulses were faint. A 12‐lead ECG (electrocardiography) showed an incidental atrial fibrillation (chronic) because a previous ECG done months earlier was similar.
Investigations
3
Laboratory investigations revealed HbA1c of 5.56%, D‐dimer of 2.47, a negative rheumatoid factor, APTT 66.8, and INR 1.32. All other blood investigations were within the normal parameters. Doppler ultrasound of the left lower limb showed no vascular blood flow. A spectral Doppler waveform of the popliteal artery suggested thrombotic versus embolic occlusion with an undetectable Doppler distal flow (Figure 1). The patient was thrombosed with tenecteplase 30 mg and transferred to the ICU for monitoring. Second day post admission, the patient's left lower limb was found to be cyanotic at the medial toe and was cold and tender on palpation. No palpable foot pulse and pulse oximetry of the toes yielded no measurable plethysmograph, and no saturation could be recorded. The initial range of mobility of the toe at this level was significantly reduced; the patient could no longer flex her toes. An urgent CT angiography was done which showed a thrombus occluding approximately 90% of the distal abdominal aorta (Figure 2a). Figure 2b shows the absence of blood flow with a filling defect in the left iliac artery.
Doppler ultrasound of the left lower limb showed no color and spectral Doppler waveform of the popliteal artery suggestive of thrombus versus embolism with undetectable Doppler distal flow.
(a) A coronal view of contrast‐enhanced CT angiography showing an approximately full occlusion of the distal abdominal aorta black arrow. (b) A black arrow indicates left iliac artery filling defect.
Results
4
The patient was given a loading dose of 250,000 IU of intravenous streptokinase followed by an infusion of 50,000 IU/h. Despite this, no clinical improvement was noted. Following a failure of this treatment, a decision was made to insert an arterial catheter in the left femoral artery, which was used to infuse medications directly into the obstruction. An intra‐arterial infusion of papaverine at 30 mg/h and streptokinase at 50,000 IU/h was initiated. Approximately 6 h after the initiation of this treatment, cyanosis of the left toe reduced significantly. The posterior tibial pulse could be palpated and pulse oximetry yielded a plethysmograph with saturations ranging from 50% to 69%. This treatment continued for 48 h and improved her left lower limb. The patient was thereafter referred to a higher facility for a vascular surgeon review and possible vascular stenting. Our country lacks the appropriate vascular stents required for such procedures. This was the justification for using intra‐arterial pharmacological therapy to salvage and maintain the arterial integrity of the limb until definitive care could be obtained.
Conclusion
5
Distal abdominal aortic thrombus is still a rare and often poorly diagnosed cardiovascular emergency that requires prompt management. Timely referral in resource‐limited settings is crucial to reduce morbidity and mortality in such patients. Treatment guidelines or protocols are still lacking for this particular condition, especially for patients who present in set‐ups with a lack of vascular surgeons and interventional devices such as stents. Taking note of the case we encountered, in surgical interventional resource‐limited settings like ours, timely diagnosis and aggressive pharmacological therapy remain the only options preceding a referral.
Discussion
6
These cases mostly present with manifestations of thromboembolism and can mostly be asymptomatic [4]. Common symptoms seen in the literature are extremity pain, skin discolouration, gangrene, and necrosis. These are the most common initial presentation symptoms accounting for more than 45% of cases [4]. Risk factors such as peripheral arterial diseases, autoimmune disorders, poorly controlled glycemic levels, and hypercoagulability states (Virchow's triad) have been reported to increase the risk of arterial thrombosis formation [5]. In our patient, the notable clinical presentation was calf pain, preceded by numbness of the left lower limb 4 days before admission.
Several modalities of diagnosis of distal abdominal aortic thrombus have been used in clinical practice, including echocardiography, computed tomography, MRI (magnetic resonance imaging), and angiography [4]. Up‐to‐date CT angiography is the investigation of choice and has been used in approximately 78% of cases to diagnose distal abdominal aortic thrombus [4, 6]. Prompt diagnosis is still a challenge, and clinical judgment is of paramount importance to even consider the possibility of an arterial thrombosis, as it is likely to be rare in distal regions without affecting axial parts of the body. Literature has shown that diagnosis is usually made very late after embolization has occurred, which will manifest with all the signs and symptoms associated with the loss of arterial integrity of the affected limb, that is, gangrene [4].
Multiple treatment options with varying degrees of invasiveness are available for the management of distal abdominal aortic thrombus, although established guidelines are still lacking [4]. Currently, there are three management approaches: conservative, endovascular intervention, and surgery. A review done by Quynh et al. (2022) showed that conservative management involving thrombolysis such as (streptokinase and alteplase) was most frequently used for the management of the condition [4]. Further review showed that the choice of endovascular management such as the use of stenting and intravascular ballooning depends on the clinical condition of the patient, failure of initial conservative therapy, and recurrent thrombus after surgical intervention [7, 8, 9, 10]. Surgical thrombectomy was recommended if the thrombus was found to be occluding large vessels and there was a deterioration in the patient's clinical condition despite initial conservative pharmacological management. The location and mobility of the thrombus were also factors that affected the choice of treatment between surgery and an endovascular approach. More distal thrombi, such as those affecting the distal abdominal aorta, were found to be better for surgical rather than endovascular intervention [11, 12].
Author Contributions
Hilary Chipongo: conceptualization. Abizer Sarkar: visualization, writing – original draft. Esmail Sangey: supervision. Kishan Chudasama: writing – review and editing. Amar Swali: writing – original draft. Shaffin Rajan: writing – original draft, writing – review and editing.
Ethics Statement
The case report was conducted following ethical standards, and patient confidentiality was maintained.
Consent
Written consent for publication was obtained, and if needed, may be provided to the editor‐in‐chief.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. M. Abdi , M. Shieb , and M. Shafiei , “Idiopathic Extensive Abdominal Aortic Thrombosis With Extension to the Celiac Trunk and Mesenteric Arteries in a Previously Healthy Female,” Dubai Medical Journal 6, no. 3 (2023): 169–174.
- 2K. Dingli and V. Dhingra , “Thoracic Aortic Mural Thrombus as a Cause of Multiorgan Failure,” Minerva Anestesiologica 80 (2014): 121–122.23857452 · pubmed ↗
- 3K. Khine , A. Toor , K. Khalighi , and M. Krishnamurthy , “Incidental Descending Thoracic Aortic Thrombus: The Conundrum of Medical Versus Surgical Therapy,” Journal of Community Hospital Internal Medicine Perspectives 9, no. 6 (2019): 491–494.32002156 10.1080/20009666.2019.1684230 PMC 6968514 · doi ↗ · pubmed ↗
- 4Q. Nguyen , X. Ma , D. Vervoort , and J. G. Y. Luc , “Management Strategies for Descending Thoracic Aortic Thrombus: A Review of the Literature,” Innovations 17, no. 4 (2022): 283–296.35866207 10.1177/15569845221107011 PMC 9403384 · doi ↗ · pubmed ↗
- 5T. Yagyu , M. Naito , M. Kumada , and T. Nakagawa , “Aortic Mural Thrombus in the Non‐Atherosclerotic Aorta of Patients With Multiple Hypercoagulable Factors,” Internal Medicine 58 (2019): 381–385.30210102 10.2169/internalmedicine.0691-17PMC 6395124 · doi ↗ · pubmed ↗
- 6N. M. Shaukat , F. Taha , E. Vortsman , P. Desai , and M. Kindschuh , “Diagnosis of Abdominal Mural Aortic Thrombus Following Discovery of Common Femoral Artery and Vein Thrombosis by Point‐Of‐Care Ultrasound,” Journal of Ultrasound 18, no. 4 (2015): 415–420.26550078 10.1007/s 40477-015-0183-0PMC 4630275 · doi ↗ · pubmed ↗
- 7C. Battocchio , T. Dezi , A. D'Andrea , M. Taurino , and L. Rizzo , “Acute Occlusion of Descending Thoracic Aorta,” Annals of Vascular Surgery 60 (2019): 477.e 15–477.e 19.10.1016/j.avsg.2019.03.02431200033 · doi ↗ · pubmed ↗
- 8R. Jamjoom , M. M. Zagzoog , and S. Sait , “Outcome of Endovascular Approach for Management of Thoracic Aortic Thrombus,” Annals of Vascular Surgery 59 (2019): 307.e 7–307.e 12.10.1016/j.avsg.2019.02.04331075448 · doi ↗ · pubmed ↗