Pediatric Posttraumatic Cerebral Venous Sinus Thrombosis: Successful Resolution With Rivaroxaban
Yuxuan Zhang, Hui Liu, Hongfang Ding

TL;DR
A 7-year-old girl with posttraumatic cerebral venous sinus thrombosis was successfully treated with rivaroxaban after a delayed diagnosis.
Contribution
Demonstrates the efficacy and safety of rivaroxaban in treating pediatric posttraumatic CVST.
Findings
Initial CT imaging findings were subtle and led to a delayed diagnosis of CVST.
Rivaroxaban achieved complete thrombus resolution without bleeding complications.
NOACs like rivaroxaban are viable and safe treatment options for pediatric CVST.
Abstract
Cerebral venous sinus thrombosis (CVST) is rare in children (0.5%–1.0% of pediatric strokes) and uncommonly associated with closed traumatic brain injury. A 7-year-old girl presented with neurological symptoms following a mild closed craniocerebral injury. Early CT imaging revealed subtle findings that were initially overlooked, leading to delayed diagnosis. Subsequent magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) confirmed the diagnosis of CVST. The patient was successfully treated with enoxaparin bridging followed by rivaroxaban, achieving complete thrombus resolution without bleeding complications. This case highlights the diagnostic challenge of posttraumatic CVST in children, where initial imaging signs may be overlooked. It underscores the importance of vigilant imaging interpretation in pediatric brain trauma with persistent symptoms and demonstrates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
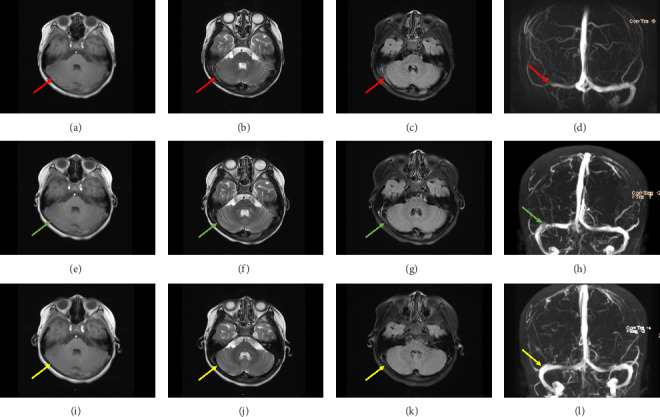 Figure 1
Figure 1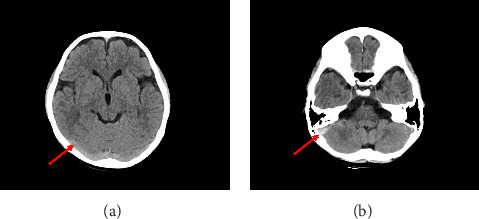 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebral Venous Sinus Thrombosis · Venous Thromboembolism Diagnosis and Management · Neurosurgical Procedures and Complications
1. Introduction
Cerebral venous sinus thrombosis (CVST) in children is a rare but potentially devastating condition, accounting for approximately 0.5%–1.0% of all strokes [1]. Its incidence is particularly low in children, estimated at about 7 cases per million [2]. CVST is even rarer after closed traumatic brain injury [3]. Diagnostic complexity stems from nonspecific symptoms (e.g., headache and vomiting) overlapping with concussion, frequently delaying neuroimaging confirmation. Current guidelines recommend D-dimer screening and neuroimaging for suspected cases, yet pediatric-specific data on biomarker reliability and optimal anticoagulation remain scarce. Low-molecular-weight heparin (LMWH) is traditionally preferred in the acute stage, followed by a transition to oral warfarin or novel oral anticoagulants (NOACs) based on individual differences [4].
This report presents a 7-year-old girl who developed CVST following a minor household fall, initially misdiagnosed as a concussion due to isolated symptoms and error report of computed tomography (CT) in the community hospital. Her subsequent diagnosis via magnetic resonance imaging (MRI)/magnetic resonance venography (MRV) and successful treatment with anticoagulant therapy, achieving complete recanalization without complications, highlight critical clinical lessons.
2. Case Presentation
A 7-year-old girl was admitted to the hospital due to dizziness and vomiting after trauma. Three days before admission, the girl jumped up on the slippery ground at home and accidently slipped, causing dizziness and vomiting. Fifteen hours after the fall, the child experienced repeated episodes of vomiting and persistent dizziness, prompting a visit to a community hospital. The patient was evaluated and underwent a CT scan of the head, which did not reveal any abnormalities. She was diagnosed with a concussion and managed conservatively with fluid replacement and rest. However, her headaches and vomiting persisted for up to 60 h following initial treatment, showing no significant relief.
Given the lack of clinical improvement, the child was brought to our institution for further evaluation. Preliminary assessment showed stable vital signs (including normotension) and a Glasgow Coma Scale score of 15. The neurological examination showed no abnormalities, with equal and reactive pupils, and no optic disc edema. Laboratory tests (complete blood count, C-reactive protein, procalcitonin, and coagulation function) including D-dimer were within normal limits. Considering the persistent and progressive symptoms, a more advanced neuroimaging was deemed necessary. A head MRI along with MRV was performed, revealing thrombosis in the right transverse sinus, sigmoid sinus, and intracranial segment of the internal jugular vein (Figures 1(a), 1(b), 1(c), and 1(d)).
Following the diagnosis of CVST, the patient was started on a regimen of subcutaneous enoxaparin sodium (25 mg/2500 IU every 12 h), with gradual resolution of dizziness and vomiting. After a week of hospitalization and clinical stabilization, followed-up MRV showed a significant reduction in thrombus burden, with visible contrast in the right internal jugular vein, transverse sinus, and sigmoid sinus (Figures 1(e), 1(f), 1(g), and 1(h)). She was discharged on oral rivaroxaban (5 mg twice daily) for a planned 3-month anticoagulation therapy. Over the subsequent 3-month outpatient visits, monthly complete blood count, coagulation parameters, and renal/liver function tests revealed consistently normal results. Follow-up head MRI at 3 months confirmed complete resolution of thrombosis in the right transverse sinus, sigmoid sinus, and intracranial segment of the internal jugular vein. Coagulation parameters remained within normal limits, and no residual symptoms or long-term sequelae were observed, indicating a favorable therapeutic outcome (Figures 1(i), 1(j), 1(k), and 1(l)).
After the event, we reviewed the initial CT images to look for clues and observed that there were hyperdense signals noted in the right transverse and sigmoid sinuses, indicative of early signs of venous sinus thrombosis (Figure 2), which were unfortunately overlooked during the initial interpretation.
3. Discussion
CVST is a rare and severe cerebrovascular disease that exhibits distinct pediatric–adult differences in risk profiles, clinical manifestations, and outcomes [5]. Pediatric CVST is predominantly associated with infections (e.g., otitis media), dehydration, minor trauma, and inherited thrombophilia [6], whereas adult cases are frequently driven by hormonal factors (oral contraceptives, pregnancy, and puerperium) [7], malignancy [8], autoimmune disorders [9], or prothrombotic disorders. Children often present with nonspecific symptoms (e.g., dizziness, persistent vomiting, and lethargy) mimicking benign conditions such as concussion, which may delay diagnosis [10]. In contrast, focal deficits (hemiparesis) or intracranial hypertension (papilledema) are more common in adults [4]. On imaging, CVST mainly involves the superior sagittal sinus/transverse sinus in both adults and children. However, children often demonstrate more extensive sinus involvement and a higher incidence of parenchymal changes, such as hemorrhagic infarcts or edema. Notably, diagnostic accuracy in children may be compromised by skull-related imaging artifacts. [11]. Prognostically, more than 80% pediatric CVST cases can achieve recanalization with early anticoagulation, yet children face higher risks of long-term neurodevelopmental sequelae (cognitive deficits and epilepsy) compared to adults' generally favorable recovery [12]. The differences between children and adults necessitate that clinicians must recognize subtle pediatric presentations, particularly posttraumatic symptoms persisting beyond 48 h, to mitigate diagnostic delays.
The association between minor head trauma and pediatric CVST may involve synergistic effects of endothelial injury [13], hemodynamic alterations [14], and developmental vascular vulnerability. Mechanical forces from low-impact trauma could disrupt venous sinus endothelium, triggering tissue factor release and platelet activation [13]. Pediatric venous systems, with thinner walls and lower baseline blood flow velocity, are prone to shear stress–induced thrombosis even following minor trauma. Concurrently, trauma-induced local inflammation may upregulate prothrombotic cytokines (e.g., IL-6) while suppressing anticoagulant pathways [15]. Hemodynamic stasis due to perivascular edema could further amplify thrombus formation, aligning with the delayed symptom onset (15–72 h posttrauma) observed here [14]. Notably, this contrasts with adult trauma-related CVST, which typically requires direct sinus injury (e.g., skull fractures) or preexisting hypercoagulable states. In children, the developmental immaturity of fibrinolysis and endothelial repair mechanisms may act as a “second hit” enabling thrombosis without traditional risk factors. This case highlights a potential pediatric-specific “two-hit” model: mechanical endothelial disruption caused by minor trauma occurring on a background of age-dependent vascular fragility. In addition, studies have shown that genetic variations in genes, such as SCN1A, MTHFR, and PROS1, may increase susceptibility to CVST [16–18]. As a multifactorial disease, although the patient in this case has no medical history or family history, the occurrence of CVST cannot completely rule out the influence of genetic factors. Unfortunately, we were unable to obtain genetic testing data for this patient.
The therapeutic management of pediatric CVST continues to evolve, with ongoing debate regarding the optimal anticoagulation strategy. While conventional agents (LMWH/warfarin) have well-established safety profiles and long-term clinical experience, the emergence of NOACs offers notable advantages in terms of convenience, predictable pharmacokinetics, and reduced monitoring requirements. Current guidelines predominantly recommend conventional anticoagulation as first-line therapy [19]. This case illustrates a successful transition strategy: After 7 days of subcutaneous enoxaparin, the patient received 3 months of oral rivaroxaban. Follow-up imaging confirmed complete thrombus resolution without bleeding complications or neurological deficits. This outcome is consistent with recent clinical trials and meta-analyses showing that NOACs are noninferior to traditional anticoagulation regimens in terms of efficacy, with potentially lower rates of minor bleeding events [20–22]. While concerns remain about child-specific NOAC dosing due to limited pharmacokinetic data in pediatric populations, this case provides pragmatic evidence supporting their judicious use: The normalization of coagulation profiles and serial imaging–confirmed thrombus resolution aligns with the ASH guidelines permitting NOACs in selected patients. This outcome underscores NOACs' viability for uncomplicated pediatric CVST. Further prospective studies are needed to establish age-specific dosing recommendations and long-term safety profiles.
This case highlights the importance of recognizing subtle imaging findings and maintaining a high index of suspicion for CVST in pediatric patients presenting with persistent headache and vomiting following head trauma, even if the initial CT report indicated no abnormalities. Notably, a normal D-dimer level (observed here at 60 h posttrauma) cannot exclude CVST due to potential late testing after thrombus stabilization. The successful use of rivaroxaban demonstrates the efficacy and safety of NOACs in this population while underscoring that early anticoagulation is crucial to prevent irreversible complications such as epilepsy. Furthermore, this patient's atypical presentation reinforces that developmental venous fragility in children lowers the threshold for thrombosis, suggesting that active imaging examinations and careful image interpretation should be carried out in prolonged postconcussive syndromes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bano S. Farooq M. U. Nazir S. Structural Imaging Characteristic, Clinical Features and Risk Factors of Cerebral Venous Sinus Thrombosis: A Prospective Cross-Sectional Analysis From a Tertiary Care Hospital in Pakistan Diagnostics 2021 May 116p. 95810.3390/diagnostics 11060958 PMC 822901234073620 · doi ↗ · pubmed ↗
- 2Filippidis A. Kapsalaki E. Patramani G. Fountas K. N. Cerebral Venous Sinus Thrombosis: Review of the Demographics, Pathophysiology, Current Diagnosis, and Treatment Neurosurgical Focus 2009 November 275p. E 310.3171/2009.8.FOCUS 091672-s 2.0-7334909666319877794 · doi ↗ · pubmed ↗
- 3Ma L. Nail T. J. Hoz S. S. Traumatic Cerebral Venous Sinus Thrombosis: Management and Outcomes World Neurosurgery 2024 July 187e 949e 96210.1016/j.wneu.2024.05.01938735561 · doi ↗ · pubmed ↗
- 4Saposnik G. Bushnell C. Coutinho J. M. Diagnosis and Management of Cerebral Venous Thrombosis: A Scientific Statement From the American Heart Association Stroke 2024 March 553e 77e 9010.1161/STR.000000000000045638284265 · doi ↗ · pubmed ↗
- 5John C. Ismail N. Clarke R. Anadure R. K. A Study on the Distinctive Clinical Profile and Thrombophilia in Pediatric Cerebral Venous Sinus Thrombosis Journal of Pediatric Neurosciences 2021 July 16322523110.4103/jpn.JPN_121_2036160607 PMC 9496605 · doi ↗ · pubmed ↗
- 6Cornelius L. P. Elango N. Jeyaram V. K. Clinico-Etiological Factors, Neuroimaging Characteristics and Outcome in Pediatric Cerebral Venous Sinus Thrombosis Annals of Indian Academy of Neurology 2021 November 24690190710.4103/aian.AIAN_221_2135359540 PMC 8965941 · doi ↗ · pubmed ↗
- 7Uluduz D. Sahin S. Duman T. Cerebral Venous Sinus Thrombosis in Women: Subgroup Analysis of the VENOST Study Stroke Research and Treatment 2020 September 20201810.1155/2020/8610903 PMC 748199332953038 · doi ↗ · pubmed ↗
- 8Xian Z. Chen Y. Chen L. A Clinical Research on the Potential Pathogenesis of Somatic Cancer Related Cerebral Venous Sinus Thrombosis Medicine (Baltimore) 2019 May 9819 p. e 1513410.1097/MD.00000000000151342-s 2.0-8506606112331083150 PMC 6531122 · doi ↗ · pubmed ↗