Recurrent Hypoglycemia in a Non-diabetic: A Case of Suspected Insulinoma Lost to Follow-Up
Ateetmani Pannu, Simant Shah

TL;DR
A non-diabetic woman experienced severe hypoglycemia and a seizure, suggesting an insulinoma, but failed to follow up for confirmation.
Contribution
Highlights the importance of considering insulinoma in non-diabetic patients with unexplained hypoglycemia.
Findings
A 56-year-old non-diabetic woman presented with hypoglycemia and seizure, suggesting insulinoma.
Imaging identified a pancreatic lesion consistent with insulinoma, but follow-up testing was not completed.
Emergency physicians should consider rare causes like insulinoma in cases of unexplained hypoglycemia.
Abstract
Insulinomas are rare insulin-secreting pancreatic neuroendocrine tumors (PNETs) that can cause profound hypoglycemia, particularly in non-diabetic patients. We report the case of a 56-year-old female who presented to the emergency department with altered mental status, a witnessed seizure, and recurrent, refractory hypoglycemia. She had no history of diabetes or hypoglycemic agent use and was reportedly in her usual state of health until the event. Initial emergency evaluation revealed persistent hypoglycemia despite dextrose administration. Cross-sectional imaging identified a pancreatic lesion concerning for insulinoma in the appropriate clinical context. Although confirmatory outpatient biochemical testing (e.g., insulin, C-peptide levels) was planned, the patient was ultimately lost to follow-up. This case underscores the critical role of emergency physicians in maintaining a broad…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
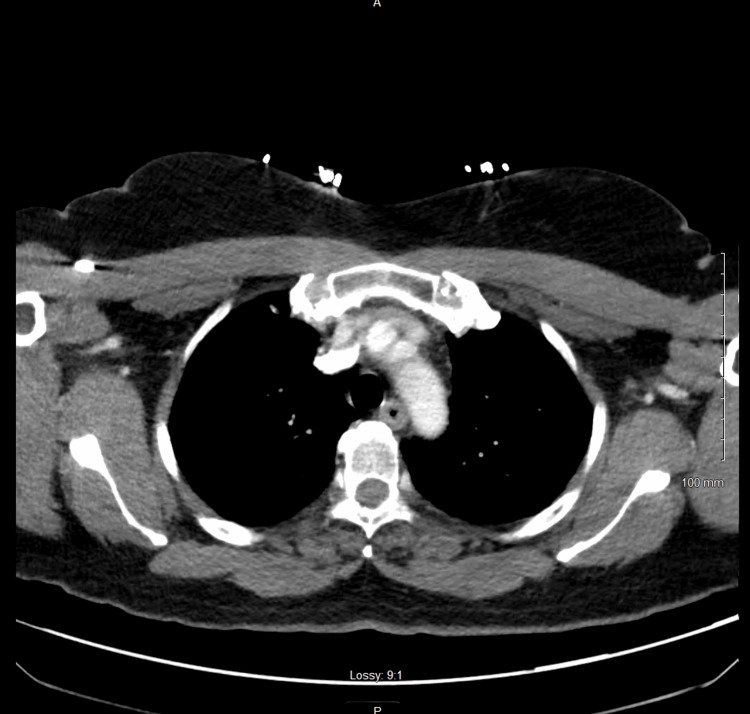 Figure 1
Figure 1| Patient’s Value | Normal Range | Abnormal Values | |
| WBC | 16 (cells/µL) | 4.0 - 11.0 (cells/µL) | 16 (cells/µL) |
| RBC | 4.41 (million cells/µL) | 3.50 - 5.10 (million cells/µL) | |
| HGB | 13.3 (g/dL) | 11.0 - 15.2 (g/dL) | |
| HCT | 41 (%) | 32.0 - 45.0 (%) | |
| MCV | 93 (fL) | 80 - 98.0 (fL) | |
| MCH | 30.2 (pg/cell) | 27.6 - 34.5 (pg/cell) | |
| MCHC | 32.4 (g/dL) | 33.0 - 36.0 (g/dL) | |
| RDW | 12 (fL) | 11.0 - 15.0 (fL) | |
| Platelets | 348 (µL) | 140 - 380 (µL) | |
| MPV | 10 (fL) | 9.4 - 12.4 (fL) | |
| Neutrophil Auto | 68.4 (cells/µL) | 40.0 - 74.0 (cells/µL) | |
| Lymphocyte Auto | 19.1 (cells/µL) | 19.0 - 48.0 (cells/µL) | |
| Monocyte Auto | 11.3 (cells/µL) | 3.0 - 9.0 (cells/µL) | 11.3 (cells/µL) |
| Eosinophil Auto | 0.2 (cells/µL) | 0.0 - 7.0 (cells/µL) | |
| Basophil Auto | 0.5 (cells/µL) | 0.0 - 1.0 (cells/µL) | |
| IG Auto | 0.5 (cells/µL) | 0.0 - 1.0 (cells/µL) | |
| NRBC Auto | 0 (µL) | 0.0 - 0.0 (µL) | |
| Neutrophil Absolute | 11 (cells/µL) | 1.8 - 7.0 (cells/µL) | 11 (cells/µL) |
| Lymphocyte Absolute | 3.1 (cells/µL) | 1.0 - 4.8 (cells/µL) | |
| Monocyte Absolute | 0.8 (cells/µL) | 0.0 - 0.8 (cells/µL) | |
| Eosinophil Absolute | 0.03 (cells/µL) | 0.0 - 0.45 (cells/µL) | |
| Basophil Absolute | 0.1 (µL) | 0.0 - 0.2 (µL) | |
| IG Absolute | 0.08 (g/dL) | 0.0 - 0.03 (g/dL) | 0.08 (g/dL) |
| Patient’s Value | Normal Range | |
| U Amphetamine screen | Negative | Negative |
| U Barbiturate screen | Negative | Negative |
| U Benzodiazepine | Negative | Negative |
| U Cannabis screen | Negative | Negative |
| U Cocaine screen | Negative | Negative |
| U Methadone | Negative | Negative |
| U Opiate screen | Negative | Negative |
| U PCP screen | Negative | Negative |
| Urine analysis | ||
| UA Color | Yellow | Yellow |
| UA Appearance | Clear | Clear |
| UA Glucose | Negative | Negative |
| UA Bilirubin | Negative | Negative |
| UA Ketones | Negative | Negative |
| UA Specific Gravity | 1.013 | 1.001 - 1.030 |
| UA Blood | Negative | Negative |
| UA pH | 6 | 5.0 - 8.0 |
| UA Protein | Negative | Negative |
| UA Urobilinogen | 0.2 | 0.2 - 1.0 |
| UA Nitrite | Negative | Negative |
| UA Leukocyte Esterase | Trace | Negative |
| Patient’s Value | Normal Range | |
| SARS-CoV-2 (COVID-19) | Negative | Negative |
| MRSA DNA probe | Negative | Negative |
| Adenovirus | Negative | Negative |
| Coronavirus 229E | Negative | Negative |
| Coronavirus HKU1 | Negative | Negative |
| Coronavirus NL63 | Negative | Negative |
| Coronavirus OC43 | Negative | Negative |
| Metapneumovirus | Negative | Negative |
| Influenza A | Negative | Negative |
| Influenza B | Negative | Negative |
| Parainfluenza virus 1 | Negative | Negative |
| Parainfluenza virus 2 | Negative | Negative |
| Parainfluenza virus 3 | Negative | Negative |
| Parainfluenza virus 4 | Negative | Negative |
| Respiratory Syncytial Virus A+B | Negative | Negative |
| Rhinovirus/Enterovirus | Negative | Negative |
|
| Negative | Negative |
|
| Negative | Negative |
|
| Negative | Negative |
|
| Negative | Negative |
| Patient’s Value | Normal Range | |
| Glucose Level | 88 (mmol/L) | 74 - 106 (mmol/L) |
| BUN | 20 (mg/dL) | 9.0 - 23 (mg/dL) |
| Creatine Level | 0.67 (mg/dL) | 0.55 - 1.02 (mg/dL) |
| BUN/Creatinine Ratio | 29.9 (mg/dL) | 5.0 - 35.0 (mg/dL) |
| Sodium Level | 140 (mEq/L) | 136 - 145 (mEq/L) |
| Potassium Level | 3.7 (mEq/L) | 3.4 - 4.5 (mEq/L) |
| Chloride Level | 108 (mmol/L) | 98 - 107 (mmol/L) |
| CO2 | 22.9 (mEq/L) | 22.0 - 30.0 (mEq/L) |
| Anion Gap | 9 (mEq/L) | 6.0 - 16.0 (mEq/L) |
| Osmolality Calculation | 281 (mOsm/kg) | 275 - 295 (mOsm/kg) |
| Calcium Level | 8.8 (mmol/L) | 8.4 - 10.2 (mmol/L) |
| Protein Total | 6.9 (g/dL) | 5.7 - 8.2 (g/dL) |
| Albumin Level | 4.4 (g/dL) | 3.5 - 5.0 (g/dL) |
| Globulin | 2.5 (g/dL) | 3.5 - 5.0 (g/dL) |
| A/G Ratio | 1.8 | 0.8 - 2.0 |
| Alk Phos | 92 (IU/L) | 46 - 116 (IU/L) |
| ALT | 27 (U/L) | 10.0 - 49.0 (U/L) |
| AST | 30 (U/L) | 0 - 34 (U/L) |
| Bilirubin Total | 0.2 (mg/dL) | 0.2 - 1.3 (mg/dL) |
| Bilirubin Direct | 0.1 (mg/dL) | 0.0 - 0.3 (mg/dL) |
| Patient’s Value | Normal Range | |
| HS Troponin Baseline | < 3 (ng/L) | < 3 (ng/L) |
| HS Troponin 2 Hours | 6 (ng/L) | < 3 (ng/L) |
| Delta Baseline 2 Hours | No Calc | < 3 (ng/L) |
| Patient’s Value | Normal Range | |
| PT | 9.8 (s) | 9.7 - 13.3 (s) |
| INR | 0.9 | 0.8 - 1.2 |
| PTT | 27.3 (s) | 22.2 - 37.6 (s) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Neuroblastoma Research and Treatments · Pancreatic and Hepatic Oncology Research
Introduction
Insulinomas are rare, functional pancreatic neuroendocrine tumors (PNETs) that originate from beta cells of the islets of Langerhans and are characterized by unregulated insulin secretion, leading to recurrent episodes of hypoglycemia. These tumors are typically small, solitary, and benign in over 90% of cases, but their clinical presentation can be elusive and variable. The estimated incidence of insulinoma is approximately 1-4 cases per million people annually, accounting for 1-2% of all pancreatic neoplasms [1].
The hallmark symptoms of insulinomas result from neuroglycopenia - seizures, visual disturbances, behavioral changes, and even loss of consciousness - making them easily mistaken for primary neurologic or psychiatric conditions [2]. If left unrecognized, repeated episodes of hypoglycemia can result in permanent neurologic injury and significant morbidity [3]. Prompt diagnosis and intervention are critical in the emergency setting, where delayed recognition of atypical hypoglycemia may lead to irreversible neurologic sequelae [3, 4].
This case explores the emergency department evaluation of a non-diabetic patient with recurrent, unexplained hypoglycemia and a clinical picture concerning for insulinoma, underscoring the importance of early clinical suspicion even when the definitive diagnosis is not immediately attainable.
Case presentation
A 56-year-old female with a history of hypertension presented to the emergency department (ED) after experiencing a witnessed seizure while traveling. According to family members, she had multiple episodes of altered consciousness without return to baseline mentation, prompting emergency medical services (EMS) activation. Upon EMS arrival, the patient was obtunded, with a point-of-care glucose of 18 mg/dL. She received 250 mL of dextrose 10% (D10), resulting in improvement of both her mental status and serum glucose.
Upon ED arrival, the patient again became diaphoretic and confused, with a repeat glucose of 14 mg/dL. A second D10 bolus was administered with resolution of symptoms. She denied any history of diabetes, seizure disorders, recent medication changes, supplement use, alcohol intake, or illicit drug use. She did report eliminating sugar from her diet one month earlier due to pre-diabetes concerns. A review of systems was negative for chest pain, gastrointestinal symptoms, or recent illnesses.
Vital signs were notable for mild hypothermia (34.3°C) and tachypnea (respiratory rate of 23). Physical examination, including a complete neurologic exam, was non-focal. Despite the patient’s return to baseline mentation, the witnessed seizure and prior unresponsiveness warranted further evaluation for alternative causes of her altered mental status, including structural central nervous system (CNS) pathology. A non-contrast computed tomography (CT) scan of the brain was obtained to evaluate for possible acute intracranial abnormalities (e.g., seizure focus, mass lesion, or infarction), and was unremarkable.
Given the patient’s recurrent hypoglycemia in the setting of abnormal vital signs, additional laboratory workup was pursued to assess systemic causes such as infection, ischemia, or metabolic derangements. A complete blood count revealed leukocytosis with monocyte predominance, which, although nonspecific, raised consideration for infectious triggers of hypoglycemia (Table 1). However, infectious workup - including a urinalysis and a comprehensive respiratory viral panel - was unremarkable (Tables 2-3). A complete metabolic panel was also obtained to evaluate for electrolyte abnormalities (e.g., hyponatremia-induced seizure) and was within normal limits (Table 4). Despite the absence of chest pain or anticoagulation use, troponin and coagulation studies were obtained due to her altered mental status and abnormal vital signs - hypothermia and tachypnea - both of which may indicate systemic illness, infarction, or sepsis; these studies were also unremarkable (Tables 5-6).
Following the second D10 bolus, the patient’s repeat serum glucose was 88 mg/dL. However, given the refractory nature of her hypoglycemia and absence of identifiable iatrogenic or toxicologic causes, a CT of the abdomen and pelvis was performed to evaluate for potential endocrine, hepatic, or malignant pathology. Imaging revealed a 1.2-cm cystic lesion at the pancreatic body-tail junction without associated ductal dilation (Figure 1). Chest X-ray and CT thorax were negative for acute findings.
Computed Tomography of Abdomen and Pelvis
The patient was admitted to the intensive care unit (ICU) on a dextrose 5% in water (D5W) infusion for persistent glucose instability. During her ICU stay, the patient disclosed prior semaglutide (Ozempic) use, which she had discontinued one month earlier due to gastrointestinal side effects. Although large-scale clinical trials and real-world observational studies have not demonstrated a definitive association between semaglutide use and pancreatic neoplasia, preclinical models suggest a theoretical risk of glucagon-like peptide-1 (GLP-1) receptor agonists contributing to the proliferation of neuroendocrine tissue - particularly in lesions expressing GLP-1 receptors. This consideration prompted heightened clinical vigilance during evaluation of her pancreatic lesion. [5, 6].
Given the patient’s recurrent hypoglycemia in the absence of diabetes or hypoglycemic agents and the pancreatic lesion on imaging, insulinoma was strongly suspected. Outpatient biochemical testing, including serum insulin, C-peptide, proinsulin, and sulfonylurea screen, was planned to confirm the diagnosis. Unfortunately, the patient was lost to follow-up before a confirmatory workup or surgical evaluation could be completed.
Discussion
Insulinomas are the most common functioning PNETs, characterized by inappropriate and autonomous insulin secretion, often resulting in symptoms of neuroglycopenia such as confusion, seizure, and altered mentation. In non-diabetic individuals, unexplained hypoglycemia - particularly when symptoms improve with glucose administration - should raise strong clinical suspicion for insulinoma, as outlined by Whipple’s Triad [2].
This case highlights the diagnostic challenges insulinomas can pose in the emergency setting, especially when patients present with altered mental status or seizure activity in the absence of common risk factors. Our patient had no history of diabetes, seizure disorders, oral hypoglycemic agents, insulin use, or critical illness to explain her profound hypoglycemia. The repeated cycle of symptomatic resolution followed by recurrent hypoglycemia despite dextrose administration and the presence of a cystic pancreatic lesion on imaging heightened concern for an insulin-secreting tumor.
While laboratory testing for insulin, C-peptide, and sulfonylurea levels was not completed in the ED, the clinical scenario strongly suggested endogenous hyperinsulinemic hypoglycemia. In the absence of exogenous insulin or sulfonylurea use, and with no evidence of adrenal insufficiency or liver dysfunction, insulinoma remained the leading differential diagnosis. Although the patient met systemic inflammatory response syndrome (SIRS) criteria - including hypothermia, tachypnea, and leukocytosis - all infectious studies, including urinalysis, chest imaging, and a comprehensive respiratory viral panel, were negative. Blood cultures were not drawn in the ED, which is a limitation; however, the patient demonstrated rapid clinical improvement with glucose administration alone, without antibiotic therapy, making sepsis a less likely etiology.
Cross-sectional imaging, particularly CT of the abdomen and pelvis, was instrumental in narrowing the differential diagnosis. While endoscopic ultrasound or magnetic resonance imaging (MRI) are often used to further characterize pancreatic lesions, CT remains the preferred initial modality in the ED due to its accessibility and high detection rates for insulinomas [7].
Early recognition of insulinoma in the emergency setting is crucial, particularly given the nonspecific and neurologically mimicking nature of its presentation. Emergency physicians may be the first to detect subtle red flags and initiate appropriate diagnostic pathways, even when confirmatory biochemical testing is deferred to the outpatient setting [3].
Although our patient was lost to follow-up, this case underscores the importance of initiating the workup early. Non-metastatic insulinomas, once resected, typically have an excellent prognosis with survival rates reaching the general population. However, some studies suggest an increased risk of subsequent comorbidities - including atrial fibrillation, intestinal obstruction, and possibly breast and renal cancers - among patients with PNETs [8]. While causality remains unconfirmed, these associations may reflect broader neuroendocrine dysregulation and merit consideration in long-term surveillance strategies. For this patient, earlier definitive diagnosis and close follow-up could have led to timely intervention and improved long-term care planning.
Conclusions
Recurrent hypoglycemia in non-diabetic patients warrants consideration of insulinoma, particularly when no exogenous or iatrogenic cause is identified. Emergency physicians should be familiar with Whipple’s Triad and the initial workup for endogenous hyperinsulinemia. Early recognition and stabilization in the ED are critical, given the potential for neurologic injury and diagnostic delays. This case reinforces the importance of diagnostic vigilance and maintaining a broad differential when evaluating unexplained hypoglycemia while also highlighting the essential role of emergency clinicians in identifying rare but serious conditions before they become life-threatening.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Approach to the patient: Insulinoma J Clin Endocrinol Metab Hofland J Refardt JC Feelders RA Christ E de Herder WW 110911181092024 https://academic.oup.com/jcem/article/109/4/1109/73343933792566210.1210/clinem/dgad 641PMC 10940262 · doi ↗ · pubmed ↗
- 2Insulinoma Zhuo F Menon G Anastasopoulou C Treasure Island, FL Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/31335019/31335019 · pubmed ↗
- 3A systematic review of localization, surgical treatment options, and outcome of insulinoma Pancreas Mehrabi A Fischer L Hafezi M 675686432014 https://doi.org/10.1007/s 00268-020-05445-x 2492120210.1097/MPA.0000000000000110 · doi ↗ · pubmed ↗
- 4Glycemic control in patients with insulinoma Hormones Matej A Bujwid H Wroński J 4894991520162822240410.14310/horm.2002.1706 · doi ↗ · pubmed ↗
- 5Safety of Semaglutide Front Endocrinol Smits MM Van Raalte DH 645563122021 https://doi.org/10.3389/fendo.2021.64556310.3389/fendo.2021.645563 PMC 829438834305810 · doi ↗ · pubmed ↗
- 6Semaglutide and cancer: A systematic review and meta-analysis Diabetes Metab Syndr: Clin Res Rev Nagendra L Bg H Sharma M Dutta D 102834172023 https://doi.org/10.1016/j.dsx.2023.10283410.1016/j.dsx.2023.10283437531876 · doi ↗ · pubmed ↗
- 7Insulinoma: pathophysiology, localization and management Future Oncol Shin JJ Gorden P Libutti SK 22923762010 https://doi.org/10.2217/fon.09.1652014658210.2217/fon.09.165PMC 3498768 · doi ↗ · pubmed ↗
- 8Long-term morbidity and mortality in patients diagnosed with an insulinoma Eur J Endocrinol Peltola E Hannula P Huhtala H 57758618520213437465110.1530/EJE-21-0230 PMC 8784472 · doi ↗ · pubmed ↗