Evaluation of Short-Term Postoperative Outcomes of Lateral Lymph Node Dissection After Neoadjuvant Radiotherapy for Rectal Cancer Patients: The Early Learning Phase After Surgical Training in the Netherlands
Eline G. M. van Geffen, Tsuyoshi Konishi, Sanne-Marije J. A. Hazen, Tania C. Sluckin, Charmaine M. Tjin-A-Koeng, Eric H. J. Belgers, Johanna G. Bloemen, Esther C. J. Consten, Rogier M. P. H. Crolla, Michalda S. Dunker, Klaas Havenga, Christiaan Hoff, Fatih Polat, Maria Verseveld

TL;DR
This study assesses the early outcomes of lateral lymph node dissection after neoadjuvant radiotherapy for rectal cancer in the Netherlands, showing acceptable complication rates and good cancer control.
Contribution
The study evaluates the implementation and outcomes of LLND in a real-world setting after surgical training in the Netherlands.
Findings
Minimally invasive LLND had acceptable complication rates with 54% experiencing complications, 21% grade 3 or higher.
41% of LLND specimens contained malignant lymph nodes, and no ipsilateral LLRs occurred.
The 18-month local recurrence rate was 14%, and disease-free survival was 55%.
Abstract
Distal, locally advanced rectal cancer might spread to lateral lymph nodes (LLNs), posing a risk of lateral local recurrence (LLR). This study evaluated quality-controlled implementation of lateral lymph node dissection (LLND) in the Netherlands. This retrospective multicenter cohort study included consecutively treated rectal cancer patients who underwent neoadjuvant therapy, total mesorectal excision (TME) surgery, and nerve-sparing minimally invasive LLND by trained surgeons across 10 Dutch hospitals. Training involved cadaver sessions, monthly video meetings, and proctoring. Outcome measures included intra- and postoperative complications, urogenital dysfunction and 18-month LLR, local recurrence (LR), and disease-free survival (DFS). The study comprised 41 patients (median follow-up period, 16 months; interquartile range, IQR, 8–21 months) with advanced tumors (27% cT4, 49% cN2,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
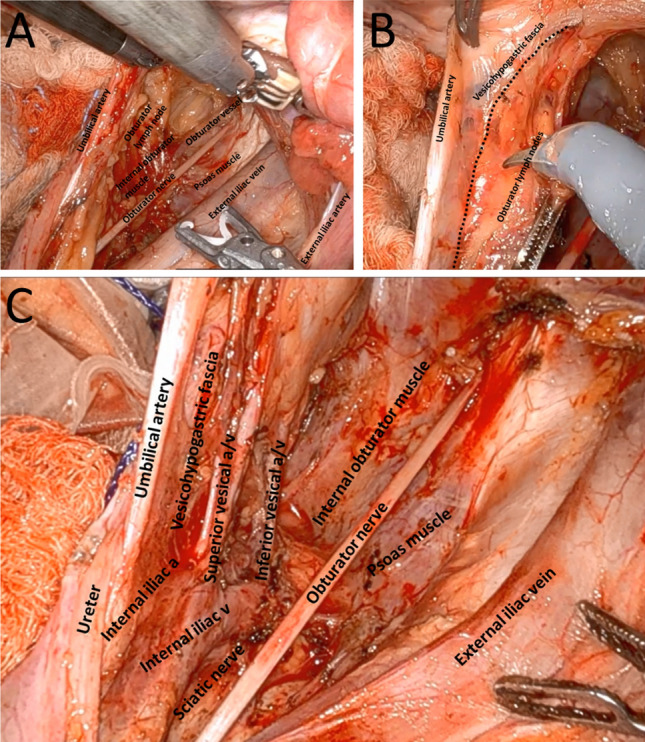 Figure 1
Figure 1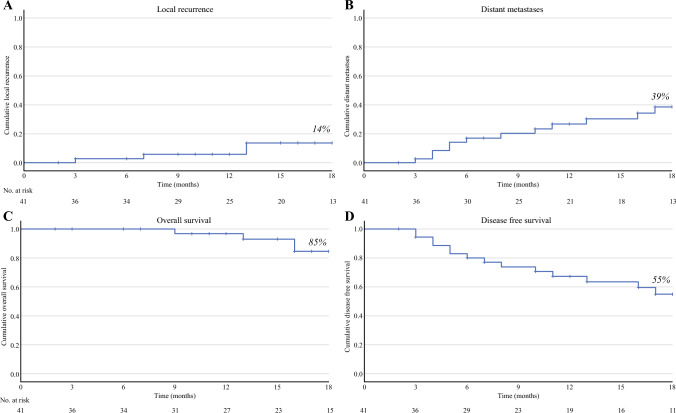 Figure 2
Figure 2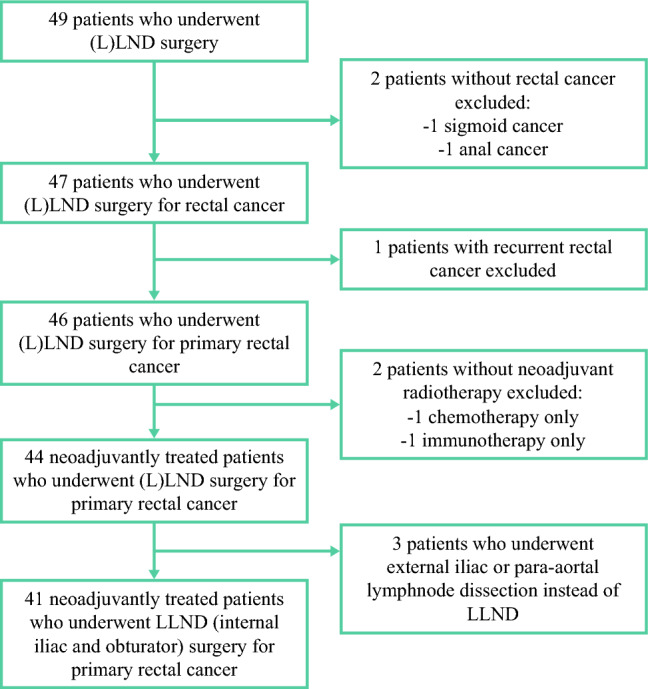 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Surgical Treatments · Colorectal and Anal Carcinomas · Anorectal Disease Treatments and Outcomes
In approximately 4% of rectal cancer patients treated with curative intent, cancer spreads to the lateral lymph nodes (LLNs) located around the internal iliac and obturator vessels.^1,2^ As shown on primary MRI, these LLNs become enlarged (≥7 mm), which is associated with a high 5-year risk of lateral local recurrence (LLR) reaching 20% despite neoadjuvant (chemo)radiation ([C]RT) and total mesorectal excision (TME).^3,4^ Lateral lymph node dissection (LLND) as an addition to ([C]RT and TME is thought to lower this risk.^5,6^
In Japan and other Eastern countries, this procedure has been widely adopted, and minimally invasive, nerve-sparing unilateral LLND seems not to worsen functional outcomes.^7–9^ Nevertheless, Dutch surgeons remain apprehensive about the procedure due to concerns about possible urogenital dysfunction, obturator nerve damage, and blood loss^5,10–12^ associated with the procedure, especially in a Western population wherein obesity is more common,^13^ and prior radiotherapy is standard practice for patients with extra-mesorectal lymph nodes.^14–18^
This topic was discussed during several meetings endorsed by the Dutch Society of Colorectal Surgery. It was concluded that to gain oncologic benefit from the procedure while minimizing the post-procedural complications, LLND surgery must be centralized. A few colorectal surgeons from each region in the Netherlands were subsequently trained in a minimally invasive nerve-sparing technique.^19^ Moreover, radiologists have been trained in recognition, measurement, and classification of LLNs,^20^ and radiation oncologists have been trained in tailored radiation of the lateral compartments according to updated national guidelines.^21^ This multidisciplinary collaboration after dedicated training of radiation oncologists, radiologists, and pathologists will be evaluated in the currently recruiting prospective LaNoReC study.^19^
The current study aimed to determine surgical and mid-term oncologic outcomes from the quality-controlled implementation of minimally invasive nerve-sparing LLND in the Netherlands.
Methods
Data collection for this multicenter retrospective cohort study was conducted between April 2024 and June of 2024 in the Netherlands. All consecutive patients with neoadjuvant radiotherapy (with or without chemotherapy) who underwent LLND of the internal iliac and obturator compartment for primary rectal cancer after the surgical training (September to November 2021) and before the LaNoReC trial were included from 10 centers (“Appendix 1”). Selection for LLND was predominantly based on short-axis size of ≥7 mm on primary MRI. If the size remained ≥7 mm on restaging MRI, this was routinely considered an indication for LLND, and in case of downsizing with a short-axis size of <7 mm, LLND was performed based on shared decision-making, thereby weighing potential oncologic benefit versus additional mortality.
Eligible patients were identified by trained surgeons. Training of radiologists was not part of the study, nor was centralized review of MRI. Data, including radiologic, surgical, and oncologic variables, were retrospectively collected by electronic patient file assessment. The Medical Ethics Committee of the Amsterdam UMC approved this study and determined it to be exempt from the Dutch Medical Research Involving Human Subjects Act.
LLND Training
After several consensus meetings organized by the Dutch Society of Colorectal Surgery, LLND surgery was centralized. This centralization aimed to ensure adequate surgical exposure for each trained surgeon given the low incidence of enlarged LLNs. After regional oncology group meetings, 16 surgeons were appointed by each region to attend two training days in September and November 2021. During these sessions, an expert in LLND surgery (Dr. Konishi) provided extensive and video-assisted lectures on the anatomy of the lateral compartments, the oncologic impact of LLNs, and examples of LLND surgery.
The surgeons practiced the minimally invasive, nerve-sparing technique in hands-on cadaver sessions, as previously outlined and illustrated in Fig. 1.^22,23^ During these sessions, the surgeons received live feedback from Dr. Konishi and their peers. Of the 16 surveons, 2 were already experienced in LLND surgery (1 in laparoscopic and 1 in robotic surgery), and were selected as proctors for further implementation. The remaining surgeons were paired geographically to ensure that each LLND procedure involved two trained surgeons. Many surgeons preferred local proctoring for their first few cases.Fig. 1. Intraoperative images of robot-assisted lateral lymph node dissection. A Overview of the lateral compartment during dissection of obturator lymph nodes. B The medial plane of lateral lymph node dissection as indicated by the umbilical artery and the vesicohypogastric fascia. C Overview of the lateral compartment after dissection of the internal iliac and obturator lymph nodes.
After these training sessions, monthly online meetings were held, with recorded LLND procedures reviewed and feedback provided by Dr. Konishi and the group. The meetings were recorded for a repeat review by surgeons and served also for presentation of new cases and discussion of preoperative planning.
Outcome Measures and Definitions
The primary outcomes were a postoperative complication rate in fewer than 30 days and the presence of urinary dysfunction at the end of the follow-up period. For nerve damage of the obturator and hypogastric nerve, intraoperative reported damage and functional loss during the follow-up period were collected. Urinary dysfunction was assessed by the need for a urinary catheter at the end of the follow-up period or by functional urinary complaints reported in the electronic patient file. No standardized urinary function assessment was performed as part of this study, and data regarding urinary residual volume or flow were not collected. Sexual dysfunction at any point during the follow-up period was evaluated based on electronic patient files.
The postoperative complication rate encompassed any deviation from the expected recovery in fewer than 30 days. For each complication, the corresponding Clavien–Dindo classification (CDC) and date of occurrence were collected. The secondary outcomes included LLN characteristics observed on primary and restaging MRI, as well as pathologic findings such as lymph node harvest in the lateral compartment. The intraoperative variables included blood loss and damage to the hypogastric and obturator nerves. Surgical complications and duration of surgery also were assessed. Additionally, midterm postoperative outcomes were evaluated, including readmissions, 18-month rates of (L)LR, distant metastases (DM), disease-free survival (DFS), and overall survival (OS).
Statistical Analysis
Categorical data are presented as frequencies and percentages. Numeric data are presented as mean with standard deviation (SD) or median with interquartile range (IQR), depending on the distribution. Kaplan-Meier analysis was used to describe (L)LR, DM, DFS, and OS rates. To compare subgroups, the chi-square or Mann–Witney U test was used, and significance was set at a p value lower than 0.05. All analyses were performed using IBM SPSS statistics version 28 (IBM, Chicago, IL, USA).
Results
From November 2021 onward, 41 consecutive patients were enrolled in this study (“Appendix 1”). The median follow-up period was 16 months (IQR, 8–21 months). The number of resections performed by the surgeons in this cohort ranged from 2 to 20. Of these 41 procedures, 28 were either performed or proctored by a surgeon with prior experience. Among the remaining 13 procedures, 3 were performed in dual-surgeon teams, after which one of the two surgeons performed an additional 5 procedures. Two other surgeons performed LLNDs individually: the one performed two procedures, and the other performed three procedures.
Patient, tumor, and treatment characteristics are detailed in Table 1. Most of the patients were classified as ASA 2 (73%) and had a distally located tumor (median distance of 6 mm from the anorectal junction). The tumor stages were predominantly advanced (cT3, 66%; cT4, 27%), and most of the patients had suspected regional lymph nodes (cN1, 27%; cN2, 49%). Three patients (7%) had synchronous distant metastases at diagnosis, which were considered to be eligible for intentional curative treatment.Table 1. Patient, tumor, and treatment characteristicsWhole cohort (n = 41)n (%)n (%)Male sex24 (59)Initially watch and wait9 (22)Mean age at resection (years)60 ± 12Ostomy for obstruction preceding resection5 (12)Mean BMI (kg/m^2^)27 ± 5Type of surgeryPrevious abdominal surgery10 (24) TME with anastomosis8 (20)Previous malignancy2 (5) TME without anastomosis2 (5)ASA classification APE29 (70) 230 (73) LLND alone (no TME)2 (5) 311 (27)Surgical approachMedian distance from the ARJ: mm (IQR)^a^6 (0–26) Conventional laparoscopic18 (44)cT Stage Robot-assisted laparoscopic19 (46) cT23 (7) TaTME4 (10) cT327 (66)Beyond TME11 (28) cT410 (27) Partial prostate/vagina4 (10)Threatened MRF by primary tumor (≤1 mm)^b^26 (65) Seminal vesicle4 (10)cN Stage Os coccyx/S51 (2) cN010 (24) Posterior exenteration2 (5) cN111 (27) M. puborectalis1 (2) cN220 (49)LLND surgerymrEMVI (grade 3 or 4)^c^12 (32) Unilateral37 (90)Lesion other than tumor ≤1 mm of MRF Bilateral4 (10) No lesion/not reported37 (90)LLND resection mrEMVI1 (2) En bloc6 (15) mrTD3 (7) Separately35 (85)cM StageTotal surgical time (min)^d^330 ± 92 cM0/cMx38 (93)Median total blood loss: ml (IQR)^e^250 (100–400) cM13 (7)Intraoperative complications12 (29)Neoadjuvant treatment Bleeding (>500 ml)4 (10) Chemoradiation therapy28 (68) Ureter damage2 (5) Short course radiotherapy + consolidation therapy8 (20) Tumor perforation2 (5) Induction systemic therapy + chemoradiation therapy4 (10) Bladder perforation1 (3) Chemoradiation therapy + consolidation therapy1 (2) Vagina perforation2 (5)Radiotherapy boost2 (5) Damage to the obturator nerve1 (3)BMI, body mass index; ASA, American Society of Aaesthesiologists; ARJ, anorectal junction; IQR, interquartile range; MRF, mesorectal fascia; mrEMVI, MRI-detected extramural venous invasion; mrTD, MRI-detected tumor deposits; TME, total mesorectal excision; APE, abdominoperineal excision; LLND, lateral lymph node dissection; TaTME, transanal total mesorectal excision^a^5 Missing values^b^1 Missing value^c^3 Missing values^d^5 Missing values^e^6 Missing values
LLNs on Primary and Restaging MRI
The mean short-axis diameter of LLNs on primary MRI was 11 ± 5 mm; Table 2). In approximately half of the patients (n = 20, 49%), the largest LLN was located in the internal iliac compartment, whereas the remaining half (n = 21, 51%) had their largest LLN in the obturator compartment. Of the 41 patients, 11 patients (28%) had multiple enlarged LLNs on one side, and 3 (8%) had bilateral enlarged LLNs. Neoadjuvant therapy consisted mainly of CRT (68%; Table 1). Restaging MRI showed that the LLNs had decreased to a mean short-axis diameter of 8 ± 3 mm, with 22 (54%) remaining ≥7.0 mm in size and three measuring ≤4.0 mm.Table 2. Lateral lymph node size on primary and restaging MRIPrimary MRI****Whole cohort (n = 41)n (%**)**Median no. of LLNs (IQR)1 (1–2)Mean short-axis size of largest LLN (mm)11 ± 5LLN compartment of the largest LLN Internal iliac20 (49) Obturator21 (51)Short-axis size of largest LLN (mm) ≥7.039 (95) 5.0–6.92 (5)Multiple enlarged LLNs on one side^a^11 (28)Bilateral enlarged LLNs^a^3 (8)Restaging MRIWhole cohort (n = 41)n (%)Mean short-axis size of largest LLN (mm)8 ± 3Largest LLN (mm) ≥7.022 (54) 4.1–6.916 (39) ≤4.03 (7)MRI, magnetic resonance imaging; IQR, interquartile range; LLN, lateral lymph node^a^As percentage of patients with an enlarged LLN (≥ 7.0 mm)
Treatment
After neoadjuvant therapy, nine patients (22%) initially pursued a watch-and-wait approach. Ultimately, 39 patients (95%) proceeded with surgical resection of the primary tumor, whereas 2 patients with a clinical complete response of the primary tumor underwent LLND only. One of these patients later experienced regrowth and subsequently required TME surgery. The surgical procedures included abdominoperineal excision (APE) in 29 cases (70%) and a beyond-TME approach in 11 cases (28%). Approximately half of the surgeries (n = 22, 54%) were performed laparoscopically, with the remaining half (n = 19, 46%) performed using robotic-assisted laparoscopy. Unilateral LLND was performed for 37 patients (90%), whereas 4 patients (10%) required bilateral LLND due to the presence of bilateral LLNs. Of these four patients, three had bilateral enlarged LLNs and 1 had an enlarged LLN on one side and intermediate LLN with malignant features on the other side.
The majority of the patients underwent nerve-sparing LLND (85%), whereas an en bloc resection of the tumor together with the LLN (not nerve-sparing) was performed in six cases (15%). Intraoperative complications occurred in 12 cases (29%), including significant blood loss exceeding 500 ml in four patients (10%). Among these patients, intraoperative bleeding accounted for total blood loss volumes of 1400 mm, 700 mm, and 600 ml in each of the two remaining cases. Injury to the ureter occurred in two cases (5%), and in one patient, the obturator nerve was injured. In no case was laparoscopic surgery converted to open surgery. The median blood loss was 250 ml (IQR, 100–400 ml), with three cases of major blood loss reported (500 ml in 2 cases and 1400 ml in 1 case). The mean surgical time was 330 min for combined TME and LLND, but could not be specified for LLND alone. None of the patients received adjuvant chemotherapy according to the Dutch colorectal cancer guideline.
Pathology
The pathologic characteristics of the primary tumors and LLNs are described in Table 3. In 15% of the cases (n = 6), TME was performed with involved margins (R1). A average of five LLNs were harvested per unilateral resection specimen. In 41% (18/45) of the LLND resection specimens, malignancy was detected in one or more of the LLNs. For one patient, pathologic assessment of the LLND specimen was not reported separately from that of the TME specimen. In the patients with pathologically positive LLNs, the mean short-axis size at restaging was significantly higher than in those without positive LLNs (9.2 vs. 6.9 mm, respectively; p = 0.04), whereas the mean short-axis size on primary MRI did not differ significantly between the two groups (12.5 vs. 10.8 mm, respectively; p = 0.19). None of those with lateral lymph nodes smaller than 4 mm (n = 2) on restaging MRI had a positive lateral lymph node. Of those with a lateral lymph node 4–5 mm in size on restaging MRI (n = 6), two were pathologically positive for malignancy (“Appendix 2”).Table 3. PathologyWhole cohort (n = 41)n (%)ypT Stage^a^ ypT04 (10) ypT11 (3) ypT29 (23) ypT320 (51) ypT45 (13)ypN Stage^a^ ypN012 (31) ypN122 (56) ypN25 (13)Resection with clear margins (R0)^a^35 (85)Type of tumor Adenocarcinoma38 (93) Mucinous carcinoma2 (5) Signet ring cell1 (2)Differentiation Well/moderate31 (95) Poorly2 (5) Not reported4Tumor regression grade^a^ Complete regression4 (11) Partial regression33 (89) No signs of regression1 (3) Not reported1Tumor deposits (≥1)11 (27)Presence of EMVI^a^7 (18)Not reported2Presence of lymphatic invasion^a^8 (21)Not reported2Mean no. of harvested LLNs^b^5 ± 3Not reported4Positive LLN^b^18 (41)Not reported1ypT Stage, pathologic T/N-stage after neoadjuvant treatment; EMVI, extramural venous invasion; LLN, lateral lymph node^a^As percentage of patients who underwent TME surgery (n = 39)^b^As percentage of each unilateral LLND (in which a bilateral LLND accounts for 2 LLNDs) (n = 45)
Post-Procedural Morbidity and Functional Outcomes
Short-term postoperative complications within 30 days were observed in 22 patients (54%; Table 4), 9 of whom had a complication classified as CDC grade 3 or higher. Pelvic abscess (n = 8) and superficial wound infections (n = 8) were the most common complications. During this period, urogenital complications occurred for three patients, including ureter leakage in two patients. Beyond the 30 days, a ureteral injury was identified in a third patient. Ureteral reconstruction was performed in all three patients. Two of these three patients had undergone a beyond TME procedure, including a total pelvic exenteration in the one patient and the seminal vesicle in the other patient. The remaining patient underwent a bilateral LLND. Three other patients were readmitted due to urosepsis or hydronephrosis.Table 4. Post-procedural morbidityWhole cohort (n = 41)n (%)Median time to discharge after surgery: days (IQR)6 (4–12)Short-term postoperative complications (<30 days)22 (54) Pelvic abscess8 Ileus/gastroparesis6 Superficial wound infection8 Urogenital complications3Short-term postoperative complications (<30 days) according to CDC grade22 (54) Grade 14 Grade 29 Grade 3a1 Grade 3b8Planned readmittance (until end of follow-up)^a^13 (32) Revision stoma3 Treatment metastases or recurrence5 Correction herniation (parastomal/perianal/incisional)3 Ureteral injury repair3Unplanned readmission (until end of follow-up)^a^18 (44) Pelvic abscess9 Ileus/gastroparesis7 Wound complications2 Urosepsis3Urinary catheter at discharge No27 (66) Yes, however, also before surgery3 (7) Yes, new urinary catheter11 (27)Urinary catheter (Foley or intermittent) at last follow-up No32 (78) Yes (permanent or intermittent)9 (22)New urinary complaints (of those without catheter)8 (35) Problems with emptying the bladder3 (38) Frequent urination2 (35) Difficulty delaying urination1 (13) No urge for urination1 (13) Problems with emptying the bladder, frequent urination, and difficulty delaying urination1 (13)Not reported9Sexual dysfunction (male) No sexual dysfunction1 (13) Not sexually active3 (38) Erectile dysfunction2 (25) Ejaculation dysfunction1 (13) Erectile and ejaculation dysfunction1 (13)Not reported16Sexual dysfunction (female) No sexual dysfunction3 (100)Not reported14LLND-specific complications Lymphocele on MRI postoperatively3 (7) Lymphedema leg1 (2) Function loss upper leg adductors3 (7)IQR, interquartile range^a^Numbers do not add up due to overlap between categories.
At the end of the follow-up period, nine patients (22%) had a newly placed urinary catheter (either self-catheterization or permanent Foley), and among those without a urinary catheter (n = 28), eight experienced new urinary complaints, as described in Table 4. Sexual dysfunction was not reported in most cases, although new sexual dysfunction was explicitly mentioned by four patients. Specific to LLND complications, three patients experienced a lymphocele detectable on postoperative MRI or computed tomography (CT). One patient experienced minor leg lymphedema, and three patients had functional impairment of the upper leg adductors, which had not recovered at the last follow-up visit.
A permanent urinary catheter was present more often after beyond-TME surgery (36% vs. 18%; p = 0.22) or en-bloc resection of the lateral compartment (33% vs. 20%; p = 0.47), but the difference did not reach statistical significance. Bilateral dissection resulted in a permanent urinary catheter rate comparable with that for unilateral dissection (25% vs. 22%; p = 0.88).
Oncologic Outcomes
After 18 months of follow-up evaluation, six patients (14%) had experienced an local recurrence (LR; Fig. 2A). Among the six observed recurrences, two were located anteriorly, and four were located presacrally. None of these recurrences occurred in the lateral compartment, resulting in a 0% LLR rate at 18 months. Notably, two of these patients had resections with positive margins (R1), and one had a signet ring cell carcinoma (“Appendix 3”). Distant metastasis developed in 39% of the patients by 18 months (Fig. 2B). Detailed tumor and treatment characteristics of the patients with local and distant recurrences are provided in “Appendix 3”. The 18-month DFS rate was 55% (Fig. 2C), and the OS rate was 85% (Fig. 2D).Fig. 2. Survival outcomes. A The 18-month local recurrence rate is 14%. B The 18-month distant metastases rate is 39%. C The 18-month overall survival rate is 85%. D The 18-month disease-free survival rate is 55%.
Discussion
This study is the first study to assess intraoperative and short-term postoperative outcomes of minimally invasive LLND post-neoadjuvant irradiation in a Western cohort after standardized training and proctoring. During 2 years, only 41 patients underwent LLND surgery for this low-incidence rectal cancer entity, underscoring the need to assess outcomes. Complication rates and functional outcomes were within acceptable limits for locally advanced distal tumors requiring complex procedures, with few CDC grade ≥3 or LLND-associated complications.
One of the primary concerns among Western surgeons regarding LLND is the risk of significant blood loss due to the need for dissection along the internal iliac vessels and their multiple branches. In the current cohort, the median blood loss was 250 ml, with bleeding more than 500 ml reported in only 10% of the cases. This is comparable with TME-only data such as that from the COLOR-II trial and the MRC CLASSIC trial (median blood loss, 200 ml [7%], significant bleeding).^24,25^
The average surgery (TME+LLND) time was 330 min, which is slightly longer than for TME alone (240–250 min),^24,26^ but considerably shorter than the previously described 531 min for TME and LLND.^23^ These findings suggest that LLND adds approximately 90 min of surgery time without significantly increased bleeding risk and should be interpreted in light of the majority of procedures beyond TME and/or APE.
High APE rates are associated with increased morbidity due to the larger pelvic floor defects from more extensive distal dissection.^27^ Previous studies describe perineal wound problems in up to 40% of APE cases, with major morbidity rates of 10–30%.^28,29^ In the current cohort, the unplanned readmission rate was similarly high (42%), primarily involving wound infections, abscesses, and ileus. The LLND-specific complications included intraoperative damage to the obturator nerve in one patient and motoric dysfunction of the upper leg adductors at end of follow-up period in three patients.
Urogenital complications (e.g., neurogenic bladder) were described in 22% of the cases, which aligns with previous studies with complication rates ranging from 0 to 22%.^23,30,31^ This seems acceptable given the differences in therapy (neoadjuvant [C]RT), population (Dutch vs Asian), high rate of en-bloc resections (15%), and/or bilateral dissections (10%) compared with the previous studies. Nevertheless, three cases of ureteral injury necessitating ureter reconstruction were described, but all these cases were managed by extensive primary surgery, including a beyond-TME procedure in two cases and a bilateral LLND in the remaining case.
Although not standard practice for LLND in the Netherlands, ureteric catheter insertion may be considered when a challenging dissection along the ureter is anticipated. Sexual dysfunction was reported in four cases, but limited documentation hampered further analysis.
Specific elements or phases during the dissection with potential to cause urogenital dysfunction were identified, either intraoperatively by the proctor or during the video meetings, and these were fed back to surgeons to reduce complication rates in the future. The ongoing LaNoReC study will provide more insights on urogenital and sexual dysfunction after LLND, whereas extensive (open) procedures with en-bloc lateral compartment resection will be evaluated separately in a registration cohort.
To minimize surgical complications and improve exposure, the procedure was centralized, and procedures were performed in dual-surgeon teams. Previous studies found a reduced operating time after 21 procedures,^32^ with a 20% increased lymph node yield after 30 procedures.^33^ The LLND learning curve had three phases: the learning phase involving the first 51 cases, the proficiency phase involving 52–83 cases, and the mastery period involving 84 or more case.^34^
Despite efforts to centralize this procedure, each surgeon in the current cohort performed only 2–20 procedures, suggesting that they are still in the early learning phase and highlighting the need for additional proctoring and video review, with the expectation of further improvement in lymph node harvest and complication rates.
The primary goal of adding LLND for patients with enlarged LLNs is to reduce the LLR rate. Although the sample size and follow-up time for this cohort were limited, the 0% LLR rate at 18 months was promising. This appears lower than in previous studies, with Kaplan-Meier curves from Sluckin et al.^2^ and Ogura et al.^3^ suggesting an approximate 10% LLR rate at 18 months after (C)RT and TME. The high pathologic positivity rate of 41% after (C)RT compared with 17–29% after node-picking or partial regional lymph node dissection,^35^ reflects both the advanced nature of this cohort (mean LLN size, 11 mm) and the necessity to perform a complete LLND according to anatomic landmarks. Moreover, the persistence of LLNs on restaging MRI highlights the necessity of performing an LLND, even with the risk of urinary dysfunction given the inferior treatment if an LLR develops. The mean retrieval of five LLNs indicates room for improvement in surgical techniques or pathologic assessment because more than 10 LLNs per unilateral minimally invasive LLND were reported previously.^36^ This issue was addressed during the video meetings, and a protocol was developed for clear communication and optimal harvest of LLNs from a resection specimen by pathologists for future improvement in the LaNoReC. Despite this low LLR rate, the 18-month DM rate of 39% is notably high compared with the rate in previous studies investigating locally advanced tumors, even in light of the 7% rate with synchronous metastases.^37,38^
The RAPIDO study included patients with similar clinical characteristics in terms of cT-stage (cT4: 32% vs. 27%), cN-stage (cN2: 69% vs. 49%), mesorectal fascia involvement (67% vs. 65%), and mrEMVI positivity (36% vs. 32%), but reported a lower DM rate after adding systemic therapy to short-term RT.^37^ Tumor location might have contributed to the higher DM rate^39^ because the tumors in this cohort were located very distally (median of 6 mm from the ARJ), in contrast to those in the RAPIDO study (32% located ≥10 cm from the anal verge).^37^ These findings, combined with the small sample of the current study, raise the possibility that only the most advanced cases (with large LLNs and poor oncologic features) are referred to expert centers for LLND surgery, whereas less extensive tumors may be treated without it.
There is a growing shift toward organ-preserving treatment strategies, with increasing use of total neoadjuvant therapy for locally advanced tumors. In this evolving treatment landscape, restaging and follow-up MRI scans have gained importance, especially for cases with a complete response of the primary tumor. Although the Organ Preservation for Rectal Adenocarcinoma (OPRA) study reported a low incidence of LLNs and recurrence rates,^40^ these findings were based on all stages II and III rectal cancer patients including more proximal tumors, and conclusions about restaging or disappearance were drawn from the entire group with visible LLNs rather than from those with enlarged LLNs. Additionally, the OPRA study was conducted in an era wherein the implications of LLNs were less well-known, which may have influenced adequate recognition and assessment. The MRI scans were not re-reviewed for this report, which inevitably has affected its reliability. In our cohort, downsizing of LLNs to 4 mm or smaller, as suggested by Ogura et al.,^4^ occurred in only three cases, but downsizing to 5 mm or smaller carried a significant risk of pathologic nodal positivity. This underscores the critical role of primary MRI for LLND selection and emphasizes the need for caution in omitting LLND in cases of reduced LLN size.
This study had several limitations. First, the small cohort size, reflecting the rarity of the disease, raises concerns about whether radiologists consistently recognize enlarged LLNs because previously only 41% were identified.^41^ Even when enlarged LLNs are detected, not all patients may be referred to expert centers for LLND surgery.
Additionally, the descriptive nature of this study and its specific patient characteristics limit comparison with previous studies on distally located, locally advanced rectal cancer. The newly implemented LLND technique and retrospective data collection hamper the assessment of outcomes not routinely reported during follow-up evaluation, such as sexual or urinary complaints.
Despite its limitations, this study is the first to report these outcomes in a Western population during an early learning period after extensive surgical training. The participation of nearly all LLND surgeons provides a comprehensive overview of current practice and offers valuable insights for preoperative counseling. The currently recruiting LaNoReC trial will provide more detailed data on urogenital and long-term oncologic outcomes.
Conclusion
Minimally invasive nerve-sparing LLND by trained surgeons shows acceptable complications rates, making it a safe procedure. No LLRs occurred, and the pathologic positivity rate of LLNs in the resection specimen (41%) underscores the potential oncologic value, particularly for locoregional control.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NICE guideline colorectal cancer 2020 [updated 15 December 2021]. Retrieved 30-09-2024 at https://www.nice.org.uk/guidance/ng 151.
- 2Colorectaal carcinoom–Richtlijn–richtlijnendatabase: NVVH [updated 8 April 2024]. Retrieved 18-09-2024 at https://richtlijnendatabase.nl/richtlijn/colorectaal_carcinoom_crc/startpagina_-_colorectaal_carcinoom.html.
- 3van Geffen EGM, Sluckin TC, Witte MG, Hazen SJA, Peters FP, Intven MPW, Tanis PJ, Kusters M, Marijnen CAM, Dutch Lateral Compartment Delineation Group. Variations in radiation therapy delineation of the lateral compartments in patients with rectal cancer: results after an updated national guideline. Pract Radiat Oncol. 2025;S 1879-8500(25)00018-9. 10.1016/j.prro.2025.01.014.10.1016/j.prro.2025.01.01439971233 · doi ↗ · pubmed ↗