Neuro-Ophthalmic Manifestation Associated With COVID-19 in a Tertiary Eye Center in Nepal
Sanjeeta Sitaula, Chiranjiwi Shah, Ganga Sagar Shah, Rajeev Ojha

TL;DR
This paper reports three cases of neuro-ophthalmic complications linked to COVID-19 in Nepal, highlighting the eye-related effects of the virus.
Contribution
The study presents novel clinical cases of neuro-ophthalmic manifestations associated with COVID-19 in a Nepalese population.
Findings
A case of nonarteritic ischemic optic neuropathy in a 42-year-old male following COVID-19 infection.
A case of papilledema due to cerebral venous sinus thrombosis in a 41-year-old female with sudden vision loss.
A case of sixth cranial nerve palsy and ischemic stroke in a 40-year-old male with no prior vascular risk factors.
Abstract
The coronavirus disease 2019 (COVID-19) primarily involves the respiratory system, but can manifest with a variety of neuro-ophthalmic symptoms. Here, we describe three cases presenting with neuro-ophthalmic manifestations secondary to COVID-19 at a tertiary center in Nepal. The first case was a 42-year-old male with sudden onset painless loss of vision noticed in the right eye (RE) after COVID-19 infection. Examination findings in the RE showed best corrected visual acuity (BCVA) of 6/18 with relative afferent pupillary defect positive and superior sectoral disk edema in the same eye. The case was diagnosed as RE nonarteritic ischemic optic neuropathy associated with COVID-19 infection. Our second case was a 41-year-old female who developed bilateral sudden diminution of vision associated with headache and vomiting on the third day of testing positive for COVID-19 infection. She had…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
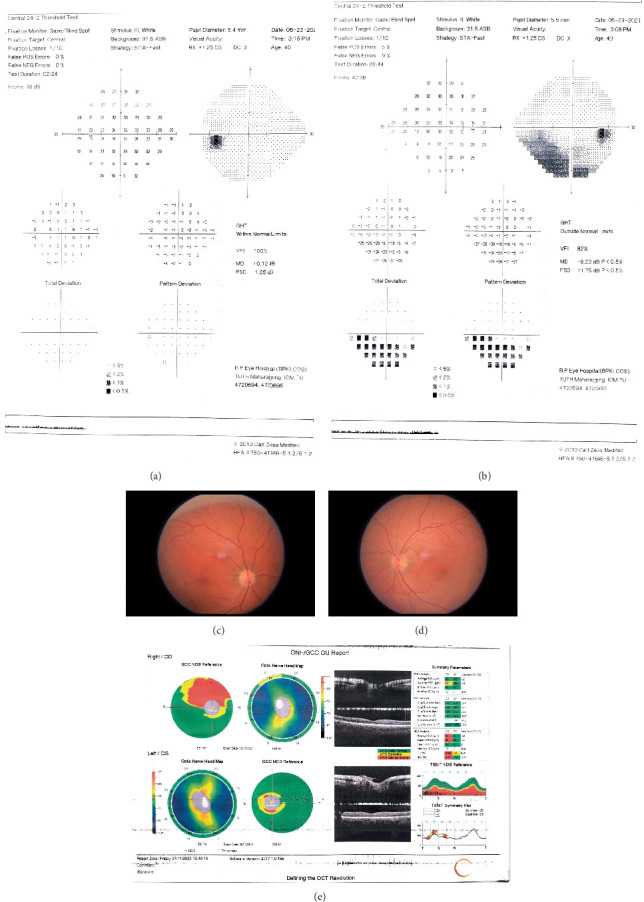 Figure 1
Figure 1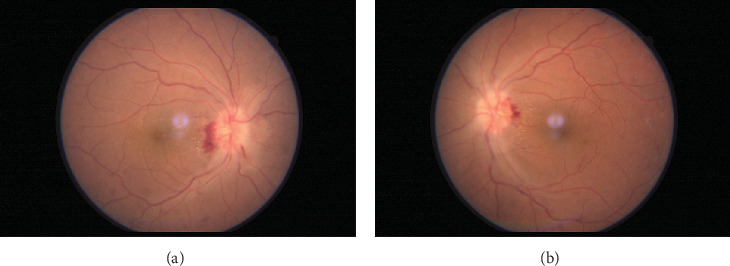 Figure 2
Figure 2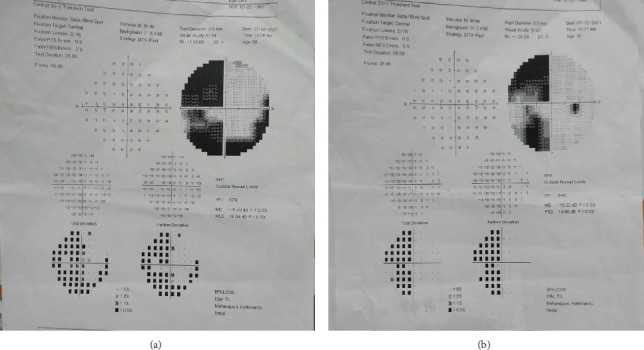 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRetinal and Optic Conditions · Long-Term Effects of COVID-19 · Cerebral Venous Sinus Thrombosis
1. Introduction
The novel coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has caused a global pandemic in the past few years. Although respiratory disease is the most common manifestation of COVID-19, the virus can affect multiple organs, including the eye and the nervous system. Coronavirus comprises a family of enveloped, positive-sense, single-stranded, RNA viruses [1]. Its infection leads to a severe inflammatory response with hypercoagulability, thrombosis, and hypoxemia causing various pulmonary and extrapulmonary disorders [2]. It can also manifest with a variety of afferent and efferent neuro-ophthalmic disorders as recognized by its neurotropic and neuroinvasive capabilities [3, 4]. More than a third of patients with COVID-19 have neurological complications [5, 6], and the incidence appears to be higher in patients with more severe infections [7]. The principal neuro-ophthalmic manifestations reported include nonarteritic ischemic optic neuropathy (NAION) [8, 9], optic neuritis [10, 11], cranial neuropathies [12, 13], Miller–Fischer syndrome [13, 14], and myasthenia gravis [15]. Here, we describe three cases presenting with neuro-ophthalmic manifestations secondary to COVID-19 at a tertiary center in Nepal. This report adheres to the tenets of the Declaration of Helsinki. Written informed consent was obtained for use of clinical information and photographs for educational purposes. The requirement for ethical approval was waived by the institutional review board as this case series involved only three cases.
2. Case Reports
2.1. Case 1
A 42-year-old male presented with sudden onset painless loss of vision noticed in the right eye (RE) on awakening in the morning since the last 7 days following a diffuse, dull aching type of headache not associated with nausea or vomiting. He had tested positive for COVID-19 3 weeks ago after having mild upper respiratory tract symptoms, which were treated with home isolation and symptomatic treatment. He had no systemic comorbidities or vasculopathic risk factors. On examination, he had the best corrected visual acuity (BCVA) of 6/18 in the RE and 6/6 in the left eye (LE) for distance. Examination of the pupil revealed Grade I relative afferent pupillary defect (RAPD) in the RE. Other anterior segment examinations were normal in both eyes. Dilated fundus examination showed superior sectoral disk edema in the RE and a crowded optic disk (disk at risk) in the LE. He had total color blindness in both eyes and had a contrast sensitivity of 1.85 and 1.95 log units in the RE and LEs, respectively, as tested on the Pelli–Robson Chart. His RE had an inferior altitudinal visual field defect, whereas the LE had a normal visual field in automated visual field (AVF) 24-2 examination, as shown in Figure 1a,b.
Blood investigations for HbA1c, liver function test, renal function test, thyroid function test, lipid profile, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) were within the normal range (Table 1). Other blood investigations like ANA, RA, VDRL, serology for HIV and HBsAg, and PT/INR were also negative. Furthermore, hypercoagulability workup was also negative and his sleep study was unremarkable. Magnetic resonance imaging (MRI) of the brain and orbits with contrast and fat suppression showed no abnormalities and NMO/MOG antibody titers were negative. CT angiogram of the neck was found to be normal. As a result, NAION secondary to COVID was diagnosed after an extensive workup which ruled out all other possible causes. At 6-month follow up, the BCVA had improved to 6/6 in both eyes, and the contrast had improved to 1.95 in both eyes; however, there was superior sectoral pallor in the RE as shown in Figure 1c,d and corresponding thinning of the superior retinal nerve fiber layer (RNFL) and the ganglion cell complex in the optical coherence tomography (OCT) as shown in Figure 1e. The inferior altitudinal field defect in the RE persisted.
2.2. Case 2
A 41-year-old female admitted for fever after testing positive for COVID-19 for 3 days complained of bilateral sudden diminution of vision for 1 day associated with headache and vomiting. She had no systemic comorbidities except hyperthyroidism. She did not endorse the use of any hormonal medications, including oral contraceptives. On ophthalmology consultation, she had bilateral BCVA of 6/12 and sluggishly reacting pupils in both eyes. Other anterior segment examinations were within the normal range. Dilated fundus examination showed established disk edema with splinter hemorrhages and tortuous vessels in both eyes, as shown in Figure 2a,b. Color vision was normal, but she had bilateral decreased contrast sensitivity (1.65 log unit). She had a constricted peripheral visual field with an enlarged blind spot on testing of the visual fields. Optical coherence tomography–retinal nerve fiber layer analysis (OCT-RNFL) showed disk edema with a thickened RNFL.
Blood investigations include HbA1c, liver function test, renal function test, thyroid function test, lipid profile, ESR, ANA, VDRL, and CRP within normal limits (Table 1). MRI of the brain and magnetic resonance venography (MRV) showed dural venous sinus (both transverse and sagittal) thrombosis. Thrombotic profile (Protein C, Protein S, Antithrombin III, lupus anticoagulant, b2 glycoprotein and anticardiolipin antibodies, and homocysteine) was also normal. Hence, the diagnosis of papilledema secondary to COVID-19 associated cerebral venous sinus thrombosis (CVST) was established. The patient was evaluated by the neuromedicine team, and treatment was started with injection enoxaparin 60 mg twice/day for 15 days, followed by tablet dabigatran 150 mg once/day and acetazolamide 500 mg twice/day. At 3 months, her visual acuity improved to 6/9 bilaterally, and disk edema resolved with ensuing pallor of the optic disk.
2.3. Case 3
A 40-year-old male was referred for ophthalmological consultation after he complained of inward deviation of the RE associated with diplopia. He had been admitted for COVID-19-associated pneumonia 1 month back. After 10 days of admission, he developed thrombosis of the left common iliac artery for which he had to undergo above-knee amputation of the left leg. He was a Type II diabetic patient for the past 10 years. He had no other systemic illnesses.
On ocular examination, he had BCVA of 6/6 in both eyes. Examination of the extraocular motility showed restriction in the right lateral gaze. Pupillary examination and the rest of the anterior and posterior segment findings were within normal range. He had normal color vision but slightly decreased contrast sensitivity (1.80 log units in the RE and 1.75 log units in the LE) as tested on the Pelli–Robson chart. The Hess chart showed underaction of the right lateral rectus (RLR) and secondary inhibition palsy of the left lateral rectus muscle (LLR). The AVF 30-2 report showed left-sided homonymous hemianopsia as shown in Figure 3a,b. His blood investigation findings are reported in Table 1. MRI of the brain revealed findings suggestive of infarction involving the right occipital lobe and posterior limb of the right internal capsule.
His treatment was continued on tablet aspirin (150 mg), tablet clopidogrel (75 mg), and tablet pregabalin (75 mg) from the neurology side. In the subsequent visit at 3 months, his lateral rectus palsy and diplopia had resolved with full ocular motility in all cardinal gazes; however, his visual fields remained unchanged.
3. Discussion
Neurologic manifestations of COVID-19 have been described since the beginning of the pandemic, with the incidence ranging from 36% [5] to more than 50% [6] in various studies. Although various neuro-ophthalmologic manifestations of COVID-19 infection have been reported, the exact incidence is unknown, and our knowledge is built on case reports. In this article, we report three cases of COVID-19 infection with neuro-ophthalmic manifestations. The mechanisms causing neuro-ophthalmic manifestations are proposed to be due to direct viral invasion, hypoxia, hypercoagulability, inflammatory reactions related to cytokine storm, delayed autoantibody formation, endothelial dysfunction, or retrograde axonal transport of the infection via cranial and peripheral nerves [3, 7, 10].
NAION is caused by occlusion of the short posterior ciliary arteries and presents as unilateral, sudden, painless irreversible vision loss, which typically occurs upon waking. It has a higher prevalence in patients with diabetes, hypertension, and ischemic heart disease, hyperlipidemia, hypercoagulability states, tobacco smokers, and in patients with small cup-to- disk ratios [16]. Our first case did not have any vascular comorbidities like diabetes and hypertension, hyperlipidemia but did have an anatomically crowded disk and had a COVID-19 infection. Infection with COVID may have led to a severe inflammatory response with hypercoagulability and hypoxemia and probably decreased vascular compliance in a crowded disk leading to NAION. Arteritic ischemic optic neuropathy (AION) is a mandatory differential diagnosis to rule out in a patient presenting with ischemic optic neuropathy. The difference between AION and NAION in the funduscopic examination is the pallor of the optic nerve head in the AION in contrast to the hyperemic and swollen one in the NAION, along with laboratory tests of elevated ESR and CRP in AION [17]. Our patient did not have any clinical signs or laboratory features compatible with AION or giant cell arteritis, thus ruling out the diagnosis.
The presence of a hypercoagulable state and evidence for the development of thrombotic complications in patients with COVID-19 was gathered early on in the COVID pandemic and even treatment guidelines for thromboembolism in COVID-19 had been published by the World Health Organization (WHO) [2, 18–20]. The mechanism for hypercoagulability could be due to severe inflammatory response, viral endothelitis, blood viscosity, and complement-mediated microangiopathy. The hypercoagulability induced by COVID-19 could have a role in our first case with NAION, resulted in the development of dural sinus thrombosis in our second case, and caused cerebrovascular accidents and deep vein thrombosis in our last case. There are numerous other case reports where patients with COVID-19 developed CVST and papilledema and variable vision loss [21–27]. Our second patient developed CVST and mild respiratory symptoms simultaneously. She did not have any identifiable predisposing factors for CVST other than COVID-19; however, it is still debatable whether COVID-19 was contributing or causal factor in the development of CVST.
Our last case, a 40-year-old male, had right sixth cranial nerve palsy, ischemic stroke involving the right occipital lobe and posterior limb of the right internal capsule, along with thrombosis of the left common iliac artery with diabetes, again proving that hypercoagulability secondary to COVID-19 may be the contributing factor. Various other case reports in the literature have reported isolated cranial nerve palsy, with most commonly sixth nerve involvement, as in our case [12, 13]. There are several other case reports of patients with visual impairment and blindness due to occipital ischemic stroke [28–30]. Most of the cases reported were either elderly and/or had other vasculopathic risk factors like hypertension, diabetes, and SLE. Our patient was a relatively young male with diabetes and multiple site involvement, indicating severe disease.
4. Conclusion
Although novel coronavirus (SARS-CoV-2) mainly causes severe acute respiratory syndrome with manifestation seen in the lungs, it can affect multiple organ systems and cause various neuro-ophthalmic manifestations. Neuro-ophthalmic manifestations in our series caused mild to moderate vision loss, probably due to a severe inflammatory response to COVID-19, leading to hypercoagulability, thrombosis, hypoxemia, and endotheliopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rabi F. A. Al Zoubi M. S. Kasasbeh G. A. Salameh D. M. Al-Nasser A. D. SARS-Co V-2 and Coronavirus Disease 2019: What We Know So Far Pathogens 202093 p. 23110.3390/pathogens 9030231 PMC 715754132245083 · doi ↗ · pubmed ↗
- 2Kichloo A. Dettloff K. Aljadah M. COVID-19 and Hypercoagulability: A Review Clinical and Applied Thrombosis/Hemostasis 202026107602962096285310.1177/1076029620962853 PMC 759231033074732 · doi ↗ · pubmed ↗
- 3Tisdale A. K. Dinkin M. Chwalisz B. K. Afferent and Efferent Neuro-Ophthalmic Complications of Coronavirus Disease 19 Journal of Neuro-Ophthalmology 202141215416510.1097/WNO.000000000000127633935220 · doi ↗ · pubmed ↗
- 4Sen M. Honavar S. G. Sharma N. Sachdev M. S. COVID-19 and Eye Indian Journal of Ophthalmology 202169348850910.4103/ijo.IJO_297_2133595463 PMC 7942063 · doi ↗ · pubmed ↗
- 5Mao L. Jin H. Wang M. Neurologic Manifestations of Hospitalized Patients With Coronavirus Disease 2019 in Wuhan, China JAMA Neurology 202077668369010.1001/jamaneurol.2020.112732275288 PMC 7149362 · doi ↗ · pubmed ↗
- 6Romero-Sánchez C. M. Díaz-Maroto I. Fernández-Díaz E. Neurologic Manifestations in Hospitalized Patients With COVID-19: The ALBACOVID Registry Neurology 2020958 e 1060 e 107010.1212/WNL.000000000000993732482845 PMC 7668545 · doi ↗ · pubmed ↗
- 7Feizi M. Isen D. R. Tavakoli M. Neuro-Ophthalmic Manifestations of Coronavirus Disease 2019 and Its Vaccination: A Narrative Review Journal of Ophthalmic & Vision Research 202318111312210.18502/jovr.v 18i 1.1273136937195 PMC 10020789 · doi ↗ · pubmed ↗
- 8Sitaula S. Poudel A. Gajurel B. P. Non-Arteritic Anterior Ischemic Optic Neuropathy in COVID-19 Infection – A Case Report American Journal of Ophthalmology Case Reports 202227 p. 2710.1016/j.ajoc.2022.10168435990799 PMC 9376983 · doi ↗ · pubmed ↗