Clinical Outcomes of Patients With Bethesda III or IV Cytology on Fine Needle Aspiration of Thyroid Nodules—A Retrospective Study
Adeel Ahmad Khan, Noor Khalil Ebrahim Jasim, Najlaa Essa A. H. Al‐Mannai, Fateen Ata, Rajen Goyal, Tania Jaber

TL;DR
This study shows that ultrasound patterns can help decide surgery for thyroid nodules with unclear biopsy results when molecular tests aren't available.
Contribution
The study identifies specific ultrasound patterns predictive of thyroid cancer in patients with indeterminate FNA results.
Findings
ATA intermediate and high-risk sonographic patterns predict malignancy in Bethesda III/IV thyroid nodules.
Malignancy rates were 37.9% for Bethesda III and 51.6% for Bethesda IV cytology.
Female patients made up 72.2% of the study population with an average age of 43.7 years.
Abstract
The appropriate management strategy for patients with thyroid nodules and indeterminate cytology on fine needle aspiration (FNA) remains unclear, especially in centres where molecular testing is not available. In this retrospective study, we aimed to identify factors predicting the risk of malignancy in these patients. This retrospective study included consecutive patients with thyroid nodules with Bethesda III/IV cytology who underwent surgical management at Hamad Medical Corporation, Qatar, between 01/01/2015 and 30/08/2023. Patients who did not undergo surgical management were excluded. We performed univariate and multivariate logistic regression analysis to assess the factors predicting the risk of malignancy in this population. Of 449 patients included in the study, the majority were females (72.2%). The mean (SD) age was 43.7 ± 10.7 years. Arab was the most common ethnicity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
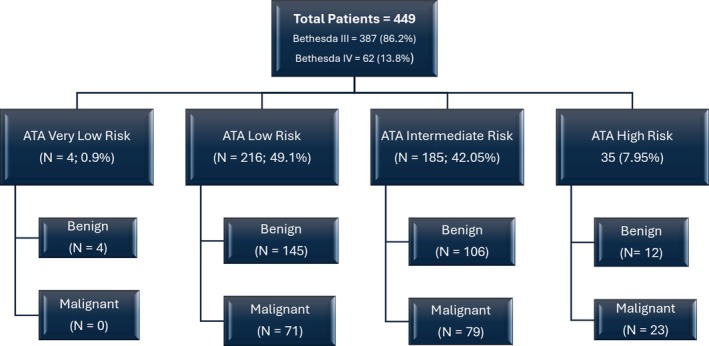 FIGURE 1
FIGURE 1| Characteristic | Units | Result |
|---|---|---|
| Total Patients |
| 449 |
| Age, Mean ± SD | Years | 43.7 ± 10.7 |
| Gender | ||
| Female |
| 324 (72.2) |
| Male | 125 (27.8) | |
| Ethnicity | ||
| South Asian |
| 85 (18.9) |
| South‐East Asian | 80 (17.8) | |
| Arabs | 254 (56.6) | |
|
Qatari | 77 (17.1) | |
|
Other Arabs | 177 (39.4) | |
| Others | 30 (6.7) | |
| Nodule size (cm) ( | ||
| ≤ 1 |
| 28 (6.3) |
| > 1 to ≤ 2 | 92 (20.8) | |
| > 2 to ≤ 4 | 191 (43.2) | |
| > 4 | 131 (29.6) | |
| Nodule echogenicity ( | ||
| Hyperechoic |
| 26 (6.2) |
| Hypoechoic | 204 (48.3) | |
| Isoechoic | 177 (41.9) | |
| Heterogenous | 15 (3.5) | |
| Nodule consistency ( | ||
| Solid |
| 331 (74.7) |
| Cystic | 19 (4.3) | |
| Solid‐cystic | 92 (20.8) | |
| Spongiform | 1 (0.2) | |
| Clacification ( | ||
| Micro |
| 69 (16.8) |
| Macro | 33 (8) | |
| Peripheral | 9 (2.2) | |
| None | 300 (73) | |
| Nodule margins ( | ||
| Regular |
| 373 (90.5) |
| Irregular | 31 (7.5) | |
| Lobulated | 8 (1.9) | |
| Lymph nodes ( | ||
| Benign |
| 154 (36.6) |
| Suspicious | 8 (1.9) | |
| None | 259 (61.5) | |
| ATA risk of malignancy ( | ||
| Very low |
| 4 (0.9) |
| Low | 216 (49.1) | |
| Intermediate | 185 (42.05) | |
| High | 35 (7.95) | |
| Bethesda classification ( | ||
| III |
| 387 (86.2) |
| IV | 62 (13.8) | |
| Cytopathology ( | ||
| AUS |
| 72 (16) |
| FLUS | 316 (70.4) | |
| Follicular Neoplasm | 40 (8.9) | |
| Suspicious for Follicular neoplasm | 21 (4.7) | |
| Total number of FNA done ( | ||
| 1 |
| 312 (69.5) |
| 2 | 11 (24.7) | |
| 3 | 22 (4.9) | |
| 4 | 3 (0.7) | |
| 6 | 1 (0.2) | |
| Characteristic | Units | Result |
|---|---|---|
| Surgical management ( | ||
| Hemithyroidectomy alone |
| 264 (58.8) |
| Hemithyroidectomy followed by completion thyroidectomy | 31 (6.9) | |
| Total thyroidectomy | 154 (34.3) | |
| Surgical histopathology ( | ||
| Benign |
| 270 (60.1) |
| Benign nodular disease | 234 (86.7) | |
| Chronic Lymphocytic thyroiditis | 22 (8.1) | |
| NIFTP | 13 (4.8) | |
| Riedel's thyroiditis | 1 (0.4) | |
| Malignant | 179 (39.9) | |
| PTC | 146 (81.6) | |
|
PTC, classic variant | 79 (44.1) | |
|
Micro PTC | 38 (21.2) | |
|
PTC, Follicular variant | 24 (13.4) | |
|
PTC, oncocytic variant | 3 (1.7) | |
|
PTC, tall cell variant | 2 (1.1) | |
| FTC | 28 (15.6) | |
| Mixed PTC and FTC | 2 (1.1) | |
| MTC | 1 (0.6) | |
| Hurthle cell carcinoma | 1 (0.6) | |
| Mixed PTC and Hurthle cell carcinoma | 1 (0.6) | |
| TNM staging ( | ||
| T1a |
| 70 (40.5) |
| T1b | 30 (17.3) | |
| T2 | 34 (19.6) | |
| T3a | 37 (21.4) | |
| T3b | 2 (1.2) | |
| N1a | 4 (2.3) | |
| N1b | 5 (2.9) | |
| N0/Nx | 164 (94.8) | |
| M1 | 1 (0.6) | |
| Variable | Units | Benign ( | Malignant ( |
|
|---|---|---|---|---|
| Age, Mean ± SD | Years | 43.3 ± 10.7 | 44.2 ± 10.5 | 0.38 |
| Gender | ||||
| Female |
| 199 (73.7) | 125 (69.8) | 0.37 |
| Male | 71 (26.3) | 54 (30.2) | ||
| Ethnicity | ||||
| South Asian |
| 48 (17.8) | 37 (20.7) | 0.47 |
| South‐East Asian | 44 (16.3) | 36 (20.1) | ||
| Qatari | 44 (16.3) | 33 (18.4) | ||
| Other Arabs | 114 (42.2) | 63 (35.2) | ||
| Others | 20 (7.4) | 10 (5.6) | ||
| Nodule size (cm) ( | ||||
| ≤ 1 |
| 18 (6.8) | 10 (5.6) | 0.26 |
| > 1 to ≤ 2 | 47 (17.8) | 45 (25.4) | ||
| > 2 to ≤ 4 | 120 (45.3) | 71 (40.1) | ||
| > 4 | 80 (30.2) | 51 (28.8) | ||
| Nodule echogenicity ( | ||||
| Hyperechoic |
| 16 (2.75) | 10 (5.9) | 0.1 |
| Hypoechoic | 112 (43.9) | 92 (54.4) | ||
| Isoechoic | 119 (46.7) | 58 (34.3) | ||
| Heterogenous | 7 (2.7) | 8 (4.7) | ||
| Nodule consistency ( | ||||
| Solid |
| 194 (72.4) | 137 (78.3) | 0.38 |
| Cystic | 11 (4.1) | 8 (4.6) | ||
| Solid‐cystic | 63 (23.1) | 30 (17.1) | ||
| Spongiform | 1 (0.4) | 0 | ||
| Calcification ( | ||||
| Micro |
| 33 (13.1) | 35 (22) | 0.06 |
| Macro | 21 (8.3) | 12 (7.5) | ||
| Peripheral | 4 (1.6) | 5 (3.1) | ||
| None | 194 (77) | 106 (66.7) | ||
| Nodule margins ( | ||||
| Regular |
| 229 (92.7) | 144 (87.3) | 0.15 |
| Irregular | 15 (6.1) | 16 (9.7) | ||
| Lobulated | 3 (1.2) | 5 (3) | ||
| Lymph nodes ( | ||||
| Benign |
| 87 (34.4) | 67 (39.8) | 0.051 |
| Suspicious | 2 (0.8) | 6 (3.6) | ||
| None | 164 (64.8) | 95 (56.5) | ||
| ATA risk of malignancy ( | ||||
| Very low |
| 4 (1.5) | 0 | 0.001 |
| Low | 145 (54.3) | 71 (41) | ||
| Intermediate | 106 (39.7) | 79 (45.7) | ||
| High | 12 (4.5) | 23 (13.3) | ||
| Bethesda classification ( | ||||
| III |
| 240 (88.9) | 147 (82.1) | 0.04 |
| IV | 30 (11.1) | 32 (17.9) | ||
| Characteristics ( | OR (95% CI) |
|
|---|---|---|
| Age | 1.007 (0.99–1.02) | 0.38 |
| Male gender | 1.21 (0.79–1.84) | 0.37 |
| Ethnicity | ||
| South‐East Asian | 1.48 (0.86–2.53) | 0.15 |
| South‐Asian | 1.39 (0.82–2.36) | 0.22 |
| Qatari | 1.35 (0.78–2.34) | 0.27 |
| Others | 0.9 (0.39–2.05) | 0.8 |
| Nodule consistency | ||
| Solid | 0.97 (0.38–2.47) | 0.95 |
| Solid‐cystic | 0.66 (0.24–1.82) | 0.43 |
| Nodule margins | ||
| Irregular | 1.69 (0.81–3.53) | 0.16 |
| Lobulated | 2.65 (0.62–11.25) | 0.18 |
| Nodule echogenicity | ||
| Hypoechoic | 1.31 (0.57–3.03) | 0.5 |
| Isoechoic | 0.78 (0.33–1.82) | 0.57 |
| Heterogenous | 1.82 (0.51–6.61) | 0.36 |
| Nodule size | ||
| > 4 cm | 1.14 (0.49–2.68) | 0.75 |
| > 2 to ≤ 4 cm | 1.06 (0.46–2.43) | 0.88 |
| > 1 to ≤ 2 cm | 1.72 (0.72–4.13) | 0.22 |
| Nodule calcification | ||
| Microcalcification | 1.94 (1.14–3.3) | 0.01 |
| Macrocalcification | 1.04 (0.49–2.2) | 0.9 |
| Lymph node on US neck | ||
| Suspicious for malignancy | 3.89 (0.76–19.9) | 0.1 |
| None | 0.75 (0.5–1.12) | 0.17 |
| ATA risk of malignancy | ||
| ATA high risk on US neck | 3.9 (1.84–8.3) | < 0.001 |
| ATA intermediate risk on US neck | 1.52 (1.01–2.28) | 0.04 |
| Characteristics ( | OR (95% CI) |
|
|---|---|---|
| ATA high risk on US neck | 3.92 (1.81–8.48) | 0.001 |
| ATA intermediate risk on US neck | 1.57 (1.03–2.4) | 0.03 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Salivary Gland Tumors Diagnosis and Treatment · Head and Neck Anomalies
Introduction
1
Thyroid nodules are a common clinical condition, and their prevalence depends on the population studied and the methods used to assess thyroid nodules. Studies have shown a prevalence of 19%–35% with ultrasound and 8%–65% in patients with autopsy data. The risk factors for thyroid nodules include advanced age, female gender, and iodine deficiency [1]. Management of thyroid nodules depends on ultrasound (US) features of the nodules, including size, margins, echogenicity, solid components, and presence or absence of high‐risk features such as microcalcifications, taller than wide shape, irregular margins, extra‐thyroidal extension, and presence of suspicious cervical lymph nodes [2]. Based on these features, thyroid nodules can be characterised as having benign, very low suspicion, low suspicion, intermediate suspicion, or high suspicion sonographic pattern. These patterns guide size cut‐off for fine‐needle aspiration (FNA) biopsy [2].
FNA cytology is the most commonly used modality to assess thyroid nodules. The sensitivity of thyroid FNA cytology ranges from 65% to 98%, and specificity ranges from 72% to 100% in the assessment of thyroid nodules, with a false positive rate for detection of thyroid cancer between 0% and 7% and a false negative rate between 1% and 11% based on available literature [3]. The addition of cytopathology has greatly reduced the number of unnecessary surgeries, especially with the advent of a standardised reporting system such as the Bethesda classification system. This system divides cytology results into six categories: I. Non‐diagnostic II. Benign, III. Atypia of undetermined significance (AUS), IV. Follicular neoplasm, V. Suspicious for malignancy, and VI. Malignant, and assigns a risk of malignancy for each category [4].
Best management strategies for patients with indeterminate cytology results on thyroid FNA (Bethesda III/IV) remain controversial. The risk of malignancy in patients with Bethesda III ranges from 13% to 30%, and in Bethesda IV ranges from 23% to 34% [4]. Hence, a significant number of these patients can have benign nodules, and better diagnostic accuracy is needed within this subset to further reduce unnecessary surgeries. Any treatment modality suggested for the management of such cases should take this into account. The American Thyroid Association (ATA) recommends three possible options for managing such cases: surveillance with repeated ultrasonography ± repeat biopsy, diagnostic hemithyroidectomy, or molecular testing [5].
Qatar is a country with a significant number of patients with thyroid malignancy. From 2015 to 2019, 549 new cases of thyroid malignancy were diagnosed in Qatar, contributing significantly to healthcare costs [6]. Molecular studies on cytology specimens are not currently available in our institution or within the country, so patients with indeterminate cytology either undergo a repeat FNA or proceed to surgery. A percentage of these patients then have to undergo a completion thyroidectomy depending on the final pathology. Apart from financial toxicity, this approach also increases the number of unnecessary surgeries and potential complications [7]. It has also been previously well reported that patients' quality of life may be severely affected in patients who have undergone total thyroidectomy [8, 9]. In this retrospective study, we aimed to assess the clinical characteristics and outcomes of patients with Bethesda III or IV diagnostic category on thyroid nodule cytology.
Materials and Methodology
2
In this retrospective study, we included consecutive patients who had Bethesda III/IV cytology on FNA of thyroid nodules done at Hamad Medical Corporation, Qatar, between 01/01/2015 and 30/08/2023 and who were surgically managed. All patients had neck ultrasonography in our institution. Patients under 14 years and those with FNA cytology other than Bethesda III/IV or who did not have follow up were excluded from the study. Neck ultrasound images were reviewed by a radiologist and thyroidologist to classify nodules according to the ATA sonographic pattern.
Demographic data was collected from the electronic medical record (Cerner) and included demographic details, ultrasound characteristics of thyroid nodules, number of FNAs performed, type of surgical management, and histopathology of surgically removed thyroid specimens. Cytology and ultrasound reports were correlated with the pathology reports.
We used descriptive statistics to present the demographic data of the study cohort. We used mean (SD) and median (IQR) to summarise continuous variables, while categorical variables were summarised as percentages. We performed univariate and multivariate logistic regression analysis to assess the factors predicting the risk of malignancy in thyroid nodules with Bethesda III or IV category on FNA cytology. A p‐value of < 0.05 was considered significant. We used STATA 18 for the analysis.
Results
3
Table 1 highlights the baseline and demographic characteristics of the study population. A total of 449 patients were included in the study, the majority of whom were females (N = 324, 72.2%). The mean (SD) age was 43.7 ± 10.7 years. Arab was the most common ethnicity (N = 254, 56.6%) followed by South Asian (N = 85, 18.9%) and South‐East Asian (N = 80, 17.8%). Based on ultrasound characteristics, most of the patients had thyroid nodules between > 2 and ≤ 4 cm in size (N = 191, 43.2%), hypoechoic (N = 204, 48.1%), solid (N = 331, 74.7%) and had regular margins (N = 373, 90.5%). Most (N = 300, 73%) of the patients did not have any calcifications on US, whereas microcalcification was noted in 69 (16.8%) patients. US evidence of suspicious lymph nodes was reported only in 8 (1.9%) patients. The majority of the patients had thyroid nodules categorised as ATA very low risk (4, 0.9%), low‐risk for malignancy (216, 49.1%), followed by intermediate‐risk (N = 185, 42.05%) and high‐risk (N = 35, 7.95%). 387 (86.2%) patients had Bethesda III and 62 (13.8%) had Bethesda IV cytology results.
Table 2 highlights the management of the study group. Around 30% of patients had repeat FNA biopsy prior to proceeding with surgery. Hemithyroidectomy alone was the most common surgical intervention performed (N = 264, 58.8%), whereas total thyroidectomy was performed in 154 (34.3%) patients. 31 (6.9%) patients underwent a completion thyroidectomy following initial hemithyroidectomy. Malignancy was reported in 179 (39.9%) patients on final histopathology specimen whereas 270 (60.1%) had benign histopathology (NIFTP have been categorised as benign). Classic variant PTC was the most common thyroid malignancy (N = 79, 44.1%). Malignancy rate in Bethesda III was 37.9% (N = 147/387) and 51.6% (N = 32/62) in Bethesda IV. Figure 1 shows the proportion of benign and malignant histopathologies based on ATA risk categories.
Histopathology results based on ATA risk categories.
Patients with malignant histopathology on thyroidectomy specimens were more likely to have an ATA intermediate (45.7% vs. 39.7%; p = 0.001) and high risk (13.3% vs. 4.5%; p = 0.001) sonographic pattern based on US features. They were also more likely to have Bethesda IV on FNA cytology (17.9% vs. 11.1%; p = 0.04) compared to those with benign histopathology (Table 3).
In univariate logistic regression analysis, only the presence of microcalcifications (OR of 1.94 (1.14–3.3); p = 0.01), ATA intermediate risk (OR of 1.52 (1.01–2.28), p = 0.04), ATA high risk (OR of 3.9 (1.84–8.3); p < 0.001) and Bethesda IV on FNA cytology (OR of 1.74 (1.01–2.98); p = 0.04) were associated with malignancy (Table 4). There was no association between different ethnicities and the risk of malignancy in the univariate analysis (Table 4). In multivariate logistic regression analysis, ATA intermediate (OR of 1.57 (1.03–2.4); p = 0.03) and high risk (OR of 3.92 (1.81–8.48); p = 0.001) sonographic patterns were predictive of malignancy after adjusting for age, gender, ethnicity, and Bethesda categories (Table 5).
Discussion
4
In this retrospective study of 449 patients, we analysed the risk of malignancy and the factors predicting this risk in one of the largest cohorts of patients with thyroid nodules with indeterminate cytology on thyroid FNA who underwent thyroidectomy. To our knowledge, this is the first and largest study in this region to do so. The majority of patients had thyroid nodules with low risk for malignancy ATA sonographic pattern, followed by intermediate risk and high risk. The rate of malignancy in this cohort was 39.9% with classic variant PTC being the most prevalent thyroid cancer subtype. In multivariate logistic regression analysis, ATA intermediate and high risk sonographic patterns were predictive of malignancy.
A major strength of this study is that the estimate of the risk of malignancy in indeterminate thyroid nodules in this study may be more accurate than previously reported, as all patients in this study underwent surgery. Having said that, we are well aware that the heterogeneity in reporting AUS cytology and the subsequent rate of malignancy in indeterminate nodules varies among institutions, which explains the variable literature.
The rate of malignancy in our cohort is considerably higher than that reported by Ali et al., underscoring the importance of conducting region‐specific and institution‐specific studies [4]. Our results are consistent with a study by Alyusuf et al., who, in a cohort of 278 patients with Bethesda III and IV thyroid nodules, showed a 39.9% malignancy rate [10]. In another study by Ho et al. consisting of 381 surgically managed patients with Bethesda III FNA cytology, a malignancy rate of 37.8% was noted, similar to our cohort [11]. On the other hand, a study from the subcontinent showed a much lower malignancy rate in patients with Bethesda III compared to our cohort (29.6% vs. 37.9%) and a similar rate in Bethesda IV patients (47.1% vs. 56.1%) [12]. However, the study cohort was very small and included only 27 patients in Bethesda III and 87 patients in Bethesda IV. Mosca et al. reported a malignancy rate of only 12% (N = 384) in Bethesda III and 11.2% (N = 242) in Bethesda IV patients, much lower than our cohort [13]. This could be related to demographic differences between the two cohorts. A significant proportion of our patients consisted of South Asian and South East Asian origin (N = 165, 36.74%), who are known to have a higher incidence of thyroid malignancy compared to other ethnicities [14, 15, 16].
The variable and heterogeneous results reported in the literature further underscore the need for better diagnostic accuracy for this subset of nodules. Recently, Latia et al. found stiffness on elastography as an indicator of malignancy in patients with Bethesda IV thyroid nodules [17]. Stoian et al. report a sensitivity of 89.5% for detecting thyroid malignancy using combined ultrasound and elastography in patients with Bethesda III nodules [18]. Elastography and contrast‐enhanced ultrasound remain exploratory in their role in distinguishing malignancy in thyroid nodules. While their combined use may be a useful non‐diagnostic adjunct to conventional US, they are yet to be validated as compared to ATA risk patterns [19]. Molecular assays have recently emerged as a diagnostic tool that may offer improved diagnostic accuracy and decrease unnecessary surgeries. In the absence of these markers, however, management of patients with thyroid nodules with indeterminate FNA cytology poses a significant challenge. Several studies have attempted to identify factors that can help in the decision‐making process. Alyusuf et al. concluded that the presence of hypoechogenicity and calcifications on thyroid US was independently associated with two‐fold increased risk of malignancy in patients with indeterminate FNA cytology [10]. In a meta‐analysis, Gao et al. concluded that among patients with Bethesda III thyroid nodules, the presence of one high‐risk US feature (hypoechogenicity, calcifications, irregular margin, taller‐than‐wide shape, or increase in nodule size during follow‐up) had a 75% sensitivity of predicting underlying malignancy. Moreover, the likelihood of malignancy increased as the number of suspicious features on US increased [20]. Similarly, a meta‐analysis performed by Li et al. found that irregular nodule margins, solitary nodules, hypoechogenicity, microcalcifications, and being taller than wide are independently associated with underlying malignancy in thyroid nodules [21]. Similar associations between different sonographic features and thyroid malignancy have been reported in several other studies [22, 23]. On the other hand, Sahin et al. did not find any significant association between sonographic characteristics of thyroid nodules and the risk of malignancy [24]. In our study, except for the presence of microcalcifications, none of the other sonographic features, if taken alone, were predictive of malignancy in thyroid nodules. However, when all the sonographic features were interpreted together as ATA risk sonographic pattern, these features collectively predicted malignancy, as evidenced by the association between ATA intermediate and high‐risk categories and malignancy in our cohort (Tables 4 and 5). This is again in accordance with the latest published guidelines by ATA [4].
Our study has several strengths. With a sample size of 449 patients, this is the largest cohort for predicting malignancy in indeterminate thyroid nodules. Another important strength of our study is the inclusion of a multi‐ethnic population consisting of South Asians, Southeast Asians, and Arabs, thus enabling a deeper understanding of the clinical implications of indeterminate thyroid nodules in this previously understudied group of patients. Moreover, to our knowledge, this is the first study in the region validating the utility of ATA risk categorisation in the assessment of patients with indeterminate thyroid nodules. However, the study is retrospective, which means that the effect of potential confounders cannot be eliminated. Specifically, since the study included only patients with surgically managed Bethesda III and IV nodules, the risk of selection bias needs to be kept in mind while interpreting the results. Such limitations are inherent to the retrospective designs and can only be addressed via prospective studies to follow the outcomes of patients with indeterminate cytology who did not undergo surgery and compare them to those who underwent surgery. Another limitation of this study is the lack of exploration of the impact of non‐invasive follicular thyroid cancer with papillary‐like features (NIFTP) on malignancy rate. Since the sample size of NIFTP patients in our study was very small and the study did not include any prolonged follow‐up of patients diagnosed with NIFTP, the potential impact of NIFTP on malignancy rates in our study could not be calculated.
Conclusion
5
In patients with thyroid nodules with indeterminate cytology and in the absence of molecular assays, clinicians can rely on the ATA sonographic pattern of thyroid nodules and risk of malignancy to help guide the need for surgery. In a low risk pattern, surveillance with neck ultrasonography may be sufficient.
Author Contributions
Adeel Ahmad Khan: conceptualisation, data curation, formal analysis, investigation, methodology, validation, visualisation, writing – original draft, writing – review and editing. Noor Khalil Ebrahim Jasim, Najlaa Essa A. H. Al‐Mannai: data curation, writing – original draft. Fateen Ata: formal analysis, investigation, visualisation, writing – original draft. Rajen Goyal: data curation. Tania Jaber: principal investigator, validation, conceptualisation, supervision, writing – review and editing.
Disclosure
The authors have nothing to report.
Ethics Statement
The study has been approved by the Medical Research Centre (MRC) at Hamad Medical Corporation, Qatar, under the approval ID MRC‐01‐23‐798. The research was conducted in compliance with the ethical principles outlined in the Declaration of Helsinki. Given the retrospective nature of this study and the de‐identified patient data, a waiver of informed consent was obtained from the MRC at Hamad Medical Corporation. We anonymised all data prior to analysis by removing personally identifiable information and assigning unique codes to each participant. All data were handled following institutional and ethical guidelines.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. S. Dean and H. Gharib , “Epidemiology of Thyroid Nodules,” Best Practice & Research. Clinical Endocrinology & Metabolism 22, no. 6 (2008): 901–911, 10.1016/j.beem.2008.09.019.19041821 · doi ↗ · pubmed ↗
- 2B. R. Haugen , E. K. Alexander , K. C. Bible , et al., “2015 American Thyroid Association Management Guidelines for Adult Patients With Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer,” Thyroid 26, no. 1 (2016): 1–133, 10.1089/thy.2015.0020.26462967 PMC 4739132 · doi ↗ · pubmed ↗
- 3C. Y. Eng , M. S. Quraishi , and P. J. Bradley , “Management of Thyroid Nodules in Adult Patients,” Head & Neck Oncology 2 (2010): 11, 10.1186/1758-3284-2-11.20444279 PMC 2877029 · doi ↗ · pubmed ↗
- 4S. Z. Ali , Z. W. Baloch , B. Cochand‐Priollet , F. C. Schmitt , P. Vielh , and P. A. Vander Laan , “The 2023 Bethesda System for Reporting Thyroid Cytopathology,” Thyroid 33, no. 9 (2023): 1039–1044, 10.1089/thy.2023.0141.37427847 · doi ↗ · pubmed ↗
- 5V. Kuta , D. Forner , J. Azzi , et al., “Treatment Choices in Managing Bethesda III and IV Thyroid Nodules: A Canadian Multi‐Institutional Study,” OTO Open 5, no. 2 (2021): 15937, 10.1177/2473974 x 211015937.PMC 823998234250424 · doi ↗ · pubmed ↗
- 6“HMC's Thyroid Unit Records Increase in Malignant Cancer Cases Diagnosed Each Year.”
- 7R. Cirocchi , S. Trastulli , J. Randolph , et al., “Total or Near‐Total Thyroidectomy Versus Subtotal Thyroidectomy for Multinodular Non‐Toxic Goitre in Adults,” Cochrane Database of Systematic Reviews 2015, no. 8 (2015): Cd 010370, 10.1002/14651858.CD 010370.pub 2.26252202 PMC 9587693 · doi ↗ · pubmed ↗
- 8C. U. Jørgensen , P. Homøe , M. Dahl , and M. F. Hitz , “Postoperative Chronic Hypoparathyroidism and Quality of Life After Total Thyroidectomy,” JBMR Plus 5, no. 4 (2021): e 10479, 10.1002/jbm 4.10479.33869995 PMC 8046100 · doi ↗ · pubmed ↗