Connectivity between long-term care homes and subsequent SARS-CoV-2 outbreaks
Yiqing Xia, Huiting Ma, Kamil Malikov, Sharon E. Straus, Christine Fahim, Gary Moloney, Qing Huang, Sahar Asgari, Jamie M. Boyd, Irene Ferro, Jaimie Johns, Kamran Khan, Jaydeep Mistry, Linwei Wang, Adrienne K. Chan, Stefan D. Baral, Mathieu Maheu-Giroux, Sharmistha Mishra

TL;DR
This study found that workers moving between long-term care homes increased the risk and timing of SARS-CoV-2 outbreaks, but not their size.
Contribution
The study introduces a novel analysis linking staff movement between care homes to the risk and timing of SARS-CoV-2 outbreaks.
Findings
Higher staff connectivity between long-term care homes increased outbreak risk by 8% per additional connection.
Staff connectivity was linked to earlier outbreak onset but not outbreak size.
Structural improvements in facilities are crucial to manage outbreaks after initial infection importation.
Abstract
To examine the relationship between individual workers employed at more than one LTCH (inter-LTCH connectivity) across LTCH and SARS-CoV-2 outbreaks. We conducted a retrospective cohort study using secondary, aggregate data (surveillance and mobile geolocation data) from 179 LTCH in the Greater Toronto Area of Ontario, the province where close to one-third of the Canada’s SARS-CoV-2 cases among long-term care homes residents were reported, between 2020-02-26 and 2020-08-31. The main exposure of interest was the inter-LTCH connectivity, generated from geographic location data procured across mobile apps. Three outcomes were examined: 1) at least one SARS-CoV-2 diagnosis among residents, 2) cumulative cases among residents in each facility, and 3) time to first outbreak. The median degree of connectivity for LTCH that experienced an outbreak (59%; 106/179) was 1.2 times the degree of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
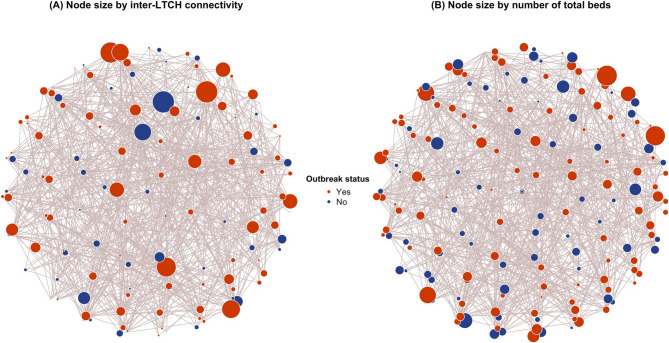 Figure 1
Figure 1- —https://doi.org/10.13039/100011094Public Health Agency of Canada
- —https://doi.org/10.13039/501100001804Canada Research Chairs
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGeriatric Care and Nursing Homes · Health disparities and outcomes · Migration, Aging, and Tourism Studies
Introduction
Long-term care home (LTCH) residents and workers were disproportionately affected by the COVID-19 pandemic [1]. In Canada, LTCH residents accounted for 80% of COVID-19 related deaths during the first wave of the epidemic [2, 3]. LTCH in Ontario, the most populous province of Canada, were among the hardest hit [4–6]. During the first wave of the SARS-CoV-2 epidemic in early 2020, LTCH residents in Ontario accounted for nearly one-third of the total number of SARS-CoV-2 diagnoses and deaths among LTCH residents in Canada [7]. In comparison, Ontario represents approximately 20% of Canada’s total number of LTCH residents [8, 9].
Even prior to the COVID-19 pandemic, respiratory virus outbreaks including influenza and SARS-CoV-1 have represented sustained threats to the health of residents in LTCH [10]. The elevated risks of nosocomial transmissions (i.e., infections acquired among LTCH residents, staff, or visitors due to pathogen spread within the facility) are multifactorial, stemming from resident vulnerability (e.g., old age, comorbidities), facilities design not suitable for infection control (e.g., communal spaces, multiple-occupancy rooms), and inadequate infection control protocols and personal protective equipment [11].
As such, efforts to reduce nosocomial outbreaks largely centered on infection control practices (such as masking, hand hygiene, etc.), improved environmental cleaning and ventilation, and strategies to reduce the introduction of infections acquired outside the facility. The latter include infections acquired in the community or in other healthcare institutions if personnels work in multiple facilities. Thus, in addition to restrictions on visitors to LTCH [12], one of the earliest pandemic response strategies employed in Ontario was provincial guidance to restrict LTCH personnel from working in more than one congregate facility–strategy implemented across jurisdictions in Canada and other countries [4, 13, 14]. That is, nurses, personal support workers (PSWs), and other care providers had to choose one facility for employment, in an effort to reduce SARS-CoV-2 transmission between LTCH.
However, movement of workers between different LTCH and other congregate settings (e.g. retirement homes, shelters) or home care, is common. This is especially true in the context of the shortage of healthcare workers across Canada [15]. Working in multiple facilities is particularly common among part-time LTCH staff and agency-staff (i.e., temporary caregivers employed by a third party) [16]–it is estimated that 24% of LTCH staff work in multiple facilities [17]. The majority of direct care personnels for residents are PSWs who earn lower-than-average wages [18–20]. In Ontario and across Canada, a combination of exposure risks—both within healthcare settings and the broader community—led to disproportionately high SARS-CoV-2 infection rates among LTCH staff, particularly PSWs, with key outbreak drivers including structural barriers to isolation (e.g., inadequate paid sick leave, overcrowded housing) and repeated exposure risks in workplace and community settings [21, 22].
The rationale for restricting movement of staff to only work on one facility during pandemic was to limit the potential spread of SARS-CoV-2 between facilities [23]. In the context of ongoing staffing shortages, however, there may have been negative consequences such as workloads exceeding capacity leading to burnout and moral injury among staff [24], and gaps in the quality of care [25, 26]–all of which might have contributed to the spread of SARS-CoV-2 [27]. To date, it is unknown to what extent staff movement between LTCH could explain outbreaks within these congregated settings such in Canada. The overarching goal of this study is to characterize the association between LTCH worker connectivity and SARS-CoV-2 outbreaks in the Greater Toronto Area (Canada). Specifically, we aim to examine whether the inter-facility connectivity was associated with (1) an outbreak in LTCH, (2) cumulative numbers of SARS-CoV2 cases in LTCH residents, and (3) time-to-first SARS-CoV-2 case in each LTCH.
Methods
Study design and study population
We conducted a retrospective cohort study using secondary aggregate-level data from the public health surveillance system and a secondary mobility database. The unit of analyses was at the level of the long-term care home, and our study included all 179 LTCH in the Greater Toronto Area, the largest urban center in Ontario, Canada from February 26, 2020, to August 31, 2020 (the first major wave of COVID-19 epidemic). The Greater Toronto Area includes Toronto, York, Peel, Halton, and Durham municipalities, where close to 50% of the Ontario’s population resides (6.7 million).
Data sources
Secondary data used for this study comprised aggregated facility-level total number of SARS-CoV-2 cases. These aggregate data were extracted from the provincial public health surveillance system databases which houses information on reportable diseases in Ontario: the Case and Contact Management System, a central data repository for SARS-CoV-2 case and contact management [28]) and the Integrated Public Health Information System (a centralized information system for the reporting and surveillance of all Diseases of Public Health Significance [29]) which includes all suspected and laboratory-confirmed cases of SARS-CoV-2 infections in Ontario. Facility-level characteristics of each LTCH were obtained from a provincial, publicly-available Ministry of Health and Long-Term Care database of standard and routinely measured indicators on LTCH attributes and the total number of residents in each LTCH [30]. This LTCH-attribute database does not include individual-level information on residents. These aggregate data were obtained from Ontario Ministry of Health and Long-Term Care under a data sharing agreement.
We used secondary aggregated LTCH facility-level mobility data (a summary of cumulative connectivity over the study period at the level of each LTCH) provided by BlueDot [31, 32]. These data were generated by BlueDot using anonymized geographic position system (usually within a few meters’ error [33]) location data procured across apps on different platforms with users’ consent from Pelmorex and Veraset. Home location and footprint of the LTCH were derived from Statistics Canada’s Open Database, and a 50-m buffer around the facility’s latitude-longitude coordinates were used if there was no information available within the database [34].
Finally, we extracted the area-level cumulative incidence of SARS-CoV-2 cases in the surrounding dissemination area (a small geographic unit with around 400–700 people; thereafter, “neighborhood”) where the LTCH were located during study period from an online, publicly-available database that was verified by the Ontario Ministry of Health [35].
Measures and outcomes
The main exposure of interest was the movement of LTCH workers across facilities. Due to lack of administrative data, we used the overall degree of connectivity between facilities during the study period (thereafter, “inter-LTCH connectivity”) as proxy. This was measured as the number of facilities a LTCH shared at least one smartphone connection with [36]. A connection between two facilities was recorded when a mobile device made a visit (a minimum of 30 min within the facility geographic unit) to one facility and made another visit to a different facility within 14-days of visiting the first. This method filters for visits that were probable staff entries into homes, distinguishing them from passing visits like deliveries or other short-term stops [37]. Additionally, as the lockdown and visiting restriction measures were also implemented at the same time as the study period [38, 39], which limited the movement of the general population and banned visiting of LTCH residents, we assumed the observed connectivity between facilities was due to worker movement.
We adjusted for facility-level factors that were related to COVID-19 outbreaks and transmission in LTCH, including for-profit ownership (Yes/No), total number of beds, proportion of private beds (i.e., 1 bed per room), and the number of residents [40]. Due to data availability limitations, we used the facility attributes on February 1, 2020, and assumed they were constant throughout the study period given the short time frame of the study. Additionally, we included an area-level measure that was associated with SARS-CoV-2 diagnosis in LTCH: number of cases in the surrounding community [23]. Given the large heterogeneities in the numbers of cases within surrounding community, we categorized a LTCH as being located in a hotspot if the cumulative rate of SARS-CoV-2 diagnoses in the neighbourhood surrounding the LTCH during the study period was high (> 300 per 100,000 population), using information from a dataset verified by Ontario Ministry of Health [35].
The primary outcome was the outbreak status (Yes/No) of a LTCH, which is defined as at least one SARS-CoV-2 case diagnosed among the residents [7]. We examined two secondary outcomes: outbreak size (measured as the total number of SARS-CoV-2 cases in each LTCH during the study period); and time-to-first SARS-CoV-2 case (measured as the time between the beginning of the epidemic in Ontario–2020-02-26, and the date of first case being reported to the Ministry of Health at each LTCH). A SARS-CoV-2 case was defined as a confirmed laboratory test using the polymerase chain reaction among residents [41].
Statistical analyses
To examine whether the inter-LTCH connectivity was associated with LTCH outbreaks, a Bayesian logistic regression model (Model 1) was built. Additionally, a Bayesian negative binomial model (Model 2) and a Bayesian Cox proportional hazard model (Model 3) were used to detect whether the inter-LTCH connectivity was associated with the outbreak size and time-to-first case, respectively. For each of the three models, we considered two types of covariates: facility-level factors (the degree of connectivity, the number of beds, the proportion of private beds, and for-profit status), and area-level factors (hotspot status). Missing data in the degree of connectivity during our study period was imputed using a missingness model as a function of the baseline degree of connectivity before the pandemic (from 2019-01-01-2020-02-25), assuming missing at random. Given the small sample size, the results are reported using 90% credible intervals (CrI). The detailed model structures are summarized in Supplementary text.
Each of the models was calibrated using 8 chains and 10,000 iterations with the rstan package [42]. All analyses were performed under R version 4.3.1.
Ethical approval
Ethics approval for use of the secondary data was obtained from the Unity Health Toronto Research Ethics Board (#23–198). This study is in compliance with the Helsinki Declaration. Participant consent for this study was deemed unnecessary, as it relied exclusively on de-identified secondary data and did not involve access to or collection of any individual-level data, in accordance with TCPS 2 (2022, Article 5.5B). We procured secondary, aggregate mobility data from BlueDot [31]. The data on cases and LTCH-level attributes comprised secondary, aggregate-level data for each LTCH, and were obtained from the routine public health surveillance system and existing databases held at the Ministry of Health Data Branch.
Results
Of the 179 LTCH in Greater Toronto Area, Ontario, 106 (59%) experienced an outbreak (at least one case among residents during the study period, Table 1). Among LTCH with an outbreak, the median cumulative diagnosis rate of SARS-CoV-2 during the study period was 237 per 1,000 residents (interquartile range [IQR]: 4 to 474). The median time-to-first case since the beginning of the epidemic in Ontario (2020-02-26) was 47 (IQR: 33-69) days. LTCH that experienced an outbreak were homes with a larger number of residents, a larger number of beds, and homes with a smaller proportion of beds that were private. A higher proportion of LTCH with outbreaks were located in SARS-CoV-2 neighbourhood hotspots.
The average degree of inter-LTCH connectivity between the LTCH during the study period decreased by 53%, compared to their baseline level. LTCH with an outbreak had slightly higher degree connectivity than those without an outbreak (Fig. 1). Regardless of outbreak status, LTCH located in neighbourhood hotspots, with larger number of beds and residents, and with for-profit ownership had higher inter-LTCH connectivity with other LTCH (Fig. 1; Figure S1-4). No differences in the degree of inter-LTCH connectivity were observed by proportion of private beds (Figure S5).
Table 1. Characteristics of long-term care homes by outbreak status in greater Toronto area, OntarioOutbreak^2^ (N = 106)No outbreak (N = 73)Degree of connectivity (median (interquartile range, IQR)) * Baseline* ^1^ 11 (7–15)9 (5–16) * Study period* 6 (3–8)5 (3–7) * Number of missing* 1119Number of total beds (median (IQR))161 (128–205)134 (93–160) Proportion of private beds (median (IQR), %)28 (9–59)45 (9–60) Number of residents (median (IQR))169.9 (75.8)130.6 (57.7)For-profit status (N (%)) * Yes* 53 (50%)43 (59%) * No* 53 (50%)30 (41%)Hotspot status^3^ (N (%)) * Yes* 77 (73%)36 (49%) * No* 29 (27%)37 (51%)Number of cases among residents during study period (median (IQR))40 (4–66)/Time to first case since 2020-02-26 in days (median (IQR))47 (33–69)/^1^Baseline period is from 2019-01-01 to 2020-02-25; Study period is from 2020-02-26 to 2020-08-31^2^An outbreak is defined as at least one SARS-CoV-2 case diagnosed among the residents^3^Hotspot: a LTCH was categorized as being located in a hotspot if the cumulative rate of SARS-CoV-2 diagnoses in the dissemination area (a small geographic unit with around 400–700 people) surrounding the LTCH during the study period was > 300 per 100,000 population
Fig. 1. Network connection across long-term care homes (LTCH) in Greater Toronto Area, Ontario by outbreak status. Each node represents a LTCH. The bigger the node, the higher degree of connectivity (panel A) and number of total beds (panel B) that LTCH had between 2020-02-26 and 2020-08-31. An outbreak is defined as at least one SARS-CoV-2 case diagnosed among the residents
In the unadjusted analysis of our primary outcome, a one-unit increase in inter-LTCH connectivity was associated with an increased odds of a SARS-CoV-2 outbreak (adjusted odds ratio [aOR]=1.11, 90% CrI: 1.03-1.20). The magnitude of association reduced after adjusting for facility-level and neighbourhood-level factors (aOR=1.08, 90% CrI: 1.00-1.17). Analyses of secondary outcomes demonstrated that increased inter-LTCH connectivity was associated with earlier SARS-CoV-2 outbreaks (adjusted hazard ratio [aHR]=1.05, 90%CrI: 1.02-1.09). However, we did not observe a statistically significant association between the degree of connectivity and the outbreak size (adjusted rate ratio [aRR] = 1.04, 90%CrI: 0.96-1.13).
Location of the home in a neighbourhood hotspot was also associated with greater odds of an outbreak (aOR=2.00, 90%CrI: 1.14-3.58) and with the hazard of an earlier first SARS-CoV-2 case (HR = 1.66, 90%CrI: 1.14-2.42). A higher proportion of private beds was associated with a lower odd of an outbreak (aOR=0.28, 90%CrI: 0.08-0.95), a lower hazard for earlier first SARS-CoV-2 cases (aHR=0.47, 90%CrI: 0.24-0.94), and a smaller outbreak size (aRR=0.19, 90%CrI: 0.05-0.80. We did not observe an association of number of total beds and for-profit ownership on all of the three outcomes examined.
Discussion
Using connectivity information derived from the mobile-device data, we quantified the strength of association between inter-LTCH connectivity and risk, timing, and size an outbreak of SARS-CoV-2 during the first wave of the COVID-19 epidemic. We found that for each additional facility to which an LTCH was connected, there was an 8 percent-point increase in the odds of an outbreak and a 5 percentage-point higher risk of an earlier outbreak. However, there was no evidence of an association between inter-LTHCH connectivity and outbreak size. Facility-level attributes including proportion of private beds and the incidence of SARS-CoV-2 cases in surrounding communities were also strongly associated with the probability and timing of an outbreak in the LTCH.
Our study suggests that inter-LTCH connectivity increased the risk of an outbreak and earlier timing of an outbreak with an exponential augmentation. For example, connections with 10 additional facilities meant 2.2-fold higher odds of an outbreak. However, connectivity was not associated with the size of an outbreak. Taken together, this association of the first two outcomes suggests that connectivity may represent an important risk factor for the introduction of a pathogen; nevertheless, it becomes less important once nosocomial transmission within a facility takes hold (size of the outbreak). This interpretation aligns with epidemic theory that staff who worked in multiple facilities posed a higher risk of case importation into these facilities [43]. Empirical studies using mobile-device data to measure connectivity in the United States and Canada also found that cross-facility staff movements accounted for approximately 50% of the cases in LTCH [36] and reduced mobility between facilities was associated with lower risk of SARS-CoV-2 in LTCH [37]. Moreover, case studies that explicitly measured staff movement in the United Kingdom provided further evidence of staff-to-resident transmission and elevated risk of infection among staff working at multiple facilities [44]. Therefore, these empirical associations (and which were conceptualized as risk factors), alongside epidemic theory, suggest that efforts to reduce connectivity could be an important early strategy but alone would be insufficient to reduce nosocomial transmission risks.
Our findings on other facility-level and area-level factors beyond connectivity align with previous literature on the importance of the facility and community characteristics. These studies demonstrated the important role of lower staff-to-resident ratio, outbreaks in surrounding community, for-profit status, and other architectural structure (e.g., proportion of private beds) factors on risks of SARS-CoV-2 outbreaks in congregated living settings [23, 36, 40, 45, 46]. This is expected because more cases in surrounding community can increase the risk of case importation, and lacking space for distancing and isolation increases the risk of transmission among residents. Low staff-to-resident ratio not only decreases the quality of care, but also increases the likelihood of staff not taking sick leave, and therefore increasing the risk of transmission [47]. We also found a protective association between the proportion of private beds and the timing of an outbreak which has not yet been discussed elsewhere. A possible explanation could be that LTCH with higher proportion of private beds were newer (better design) and had higher quality of care [48]. These findings provide further evidence to support structural strategies within LTCH to reduce transmission risks for SARS-CoV-2, and other respiratory viruses [23, 27, 45].
Our study should be interpreted considering certain limitations. First, we used mobile device connectivity as proxy to staff movement. While our visit definition aimed to increase the accuracy, some detected movements may still have been from non-LTCH staff (e.g., extended stay by delivery services, individuals waiting for a bus within 50 meters of a facility’s latitude-longitude coordinates). Additionally, the quality of the data highly depends on the extent of measurement error and the degree of completeness of the data. This may induce bias if there exists systematic error (e.g., mobile device sensor quality, device signal not captured) and missingness of staff mobile connectivity not at random (e.g., geolocation failure, invalid geocoordinate) [49]. For example, if missingness among LTCH with an outbreak was higher than those without an outbreak, then it might bias the effect of connectivity towards the null, and vice versa. However, mobile data is one of the most feasible sources of mobility information for large-scale studies on movement, compared to methods that need to distribute specific devices such as portable sensors. Second, the availability and quality of time-series network connection data (i.e., data collected at regular time intervals) were limited. Therefore, we only used overall degree of connectivity as measures of the inter-LTCH movement, instead of also looking into the impact of other network connectivity measures (e.g., the strength of connection, which also takes into account of the total number of visits between linked facility [36]) and the changing connectivity across time. Using the overall degree of connectivity as a “static” variable means that it is possible that part of the measure may have been influenced by our outcome of interest; thus, our findings surrounding association should be interpreted with caution. For example, our study is not designed to compare the associations before and after implementation of policies to limit staff working in multiplefacilities. More nuanced and time-varying measures of network connection would help generate more precise estimates of the association, especially for the time-to-event analysis. Same as the connectivity measure, we used overall number of cases reported at each LTCH during the study period as a proxy for the outbreak size, which may also affect casual interpretation of our results. Moreover, we did not study the mixing pattern of the connections between LTCH due to the quality of the data. For example, staff working at a facility with an outbreak may be more likely to have another job at the other facility, or the linkages were random, or those who moved between facilities were more likely to be personal supporting staff who had direct contact with residents [50]. This information can help estimate the causal relationship between the staff movement and the outbreaks in LTCH. Future efforts should be paid to overcome these data limitations. Finally, the association between connectivity and COVID-19 outbreaks may be obscured by the fact that more precautions due to general public health measures, as well as the changes to staffing policies, were undertaken during the study period.
This study also has several strengths. First, we used mobile data to measure the mobility of LTCH workers. This type of data provides valid and nearly real-time population movement information at a large scale that can hardly be achieved by traditional surveys [51, 52]. Moreover, this study adopted a Bayesian approach to deal with the missing data, which incorporated the uncertainty directly into the model and provided more robust and realistic estimates.
These findings have two key implications. First, if most of the connectivity between facilities is due to movement of staff who work in multiple facilities, then our findings suggest that implementing a “work only in one-site” strategy (staff cohorting) could help reduce risks of an outbreak but may not reduce the size of an outbreak. The latter is critical given trade-offs that have been identified and include low staffing levels associated with higher rates of SARS-CoV-2 in LTCH [4], staff burnout [24], lower care quality and pressure (e.g., higher rates of antipsychotic use) on LTCH residents [25, 53], etc. A pandemic response strategy that carefully separates strategies to reduce “importation” risks and “nosocomial” risks, therefore, can balance these trade-offs. For example, structural strategies to reduce nosocomial transmission risks, such as ensuring training of LTCH staff and strict protocols of infection control, increasing staff-residence ratio and adequate staff sick pay, and improving living environment of the residents [17, 23, 27], are particularly important because it is the nosocomial risks and outbreak size that shape the burden of morbidity and mortality. Second, our findings on the importance of location (in a hotspot) highlight the critical role that reducing transmission in the community could have on reducing importation risks in facilities [45].
Conclusion
To prevent and manage outbreaks of SARS-CoV-2 and other respiratory viruses in long-term care homes, policies should focus on limiting staff movement between facilities to reduce virus importation. Simultaneously, addressing widespread staffing shortages is critical to ensure care quality without compromising infection control. Structural strategies, such as improving infection prevention protocols and facility infrastructure, are essential to minimize nosocomial transmission and enhance outbreak preparedness in these congregate living settings.
Supplementary Information
Supplementary Material 1.
Supplementary Material 2.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Amy T, Hsu NL, Samir K, Sinha J, Dunning M, Dhuper ZK, Heidi Sveistrup. Understanding the impact of COVID-19 on residents of canada’s long-term care homes– ongoing challenges and policy responses. Int Long-Term Care Policy Netw. 2020. https://ltccovid.org/wp-content/uploads/2020/06/LT Ccovid-country-reports_Canada_June-4-2020.pdf. Accessed 16 Dec 2024.
- 2Clarke J. Impacts of the COVID-19 pandemic in nursing and residential care facilities in Canada. Ontario: Statistics Canada. 2021;10. https://www 150.statcan.gc.ca/n 1/pub/45-28-0001/2021001/article/00025-eng.htm. Accessed 25 Sept 2024.
- 3Long-Term Care Homes Program - A review of the plan to create 15,000 new Long-Term care beds in Ontario. Toronto: Financial Accountability Office of Ontario. 2019. https://fao-on.org/en/report/ontario-long-term-care-program/. Accessed 25 Sept 2024.
- 4Estabrooks CASS, Flood CM, Keefe J, Armstrong P, Donner G, Boscart V, Ducharme F, Silvius JWM. Restoring trust: COVID-19 and the future of Long-Term care. In: Canada R So, editor. Ottawa. 2020. https://rsc-src.ca/en/events/covid-19-policy-briefing/long-term-care/restoring-trust-covid-19-and-future-long-term-care. Accessed 25 Sept 2024.
- 5COVID-19 Visiting Policy. November 23, 2020 ed. ON, Canada. https://fco.ngo/files/COVID-19-Visiting-Policy-NOV-23.pdf. Accessed 4 Oct 2024.
- 6Newswire B. How do Canada’s provinces compare on restricting movement of care workers during COVID-19? BC Care Provider Assiciation; 2020 [updated May 29, 2020. Available from: https://bccare.ca/2020/05/how-do-canadas-provinces-compare-on-restricting-movement-of-care-workers-during-covid-19/
- 7Low L-F, CS, Taylor W, Breuer E, Yu JJ. COVID-19 and the Long-Term care system in Australia. LT Ccovid, Care Policy and Evaluation Centre, London School of Economics and Political Science. https://ltccovid.org/country-page-australia/. Accessed 4 Oct 2024.
- 8Addressing the Staffing Emergency. in Long-Term care in Canada. The Canadian Association for Long Term Care. https://www.ourcommons.ca/Content/Committee/441/HUMA/Brief/BR 11698352/br-external/Canadian Association For Long Term Care-e.pdf. Accessed 5 Oct 2024.