Dyke‐Davidoff‐Masson Syndrome in a Female Adult: A Rare Case of Progressive Hemiparesis, Epilepsy, and Cerebral Hemiatrophy
Quang Dai La, Aiman Baloch, Muhammad Ayub, Sobia Ahmed, Enoch Lue

TL;DR
This paper presents a rare case of Dyke-Davidoff-Masson syndrome in an adult woman, highlighting the importance of early diagnosis for better care.
Contribution
The novelty lies in reporting DDMS in an adult female, a rare occurrence, emphasizing MRI's role in diagnosis.
Findings
DDMS was diagnosed in an adult female with hemiparesis, epilepsy, and cerebral hemiatrophy.
MRI confirmed cerebral hemiatrophy with compensatory skull and sinus hypertrophy.
Early recognition of DDMS can improve symptom management and patient outcomes.
Abstract
Consideration of Dyke‐Davidoff‐Masson syndrome (DDMS) in patients with epilepsy, hemiparesis, and cognitive impairment should be taken into account. MRI plays a key role in diagnosing this rare disorder by recognizing cerebral hemiatrophy with compensatory skull and sinus hypertrophy. Early recognition can assist with symptom management and improve patient care, the prognosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
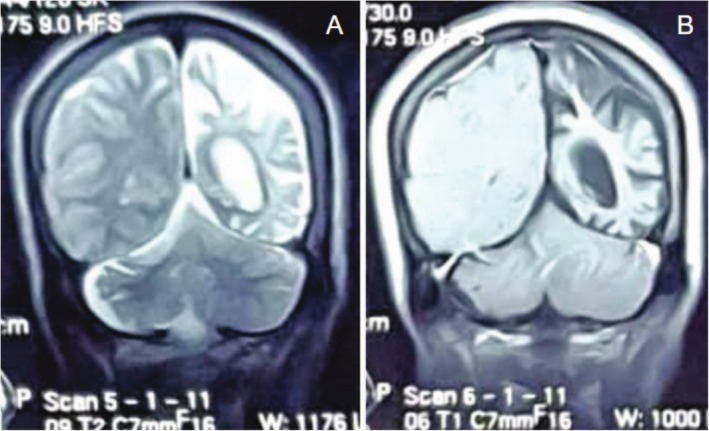 FIGURE 1
FIGURE 1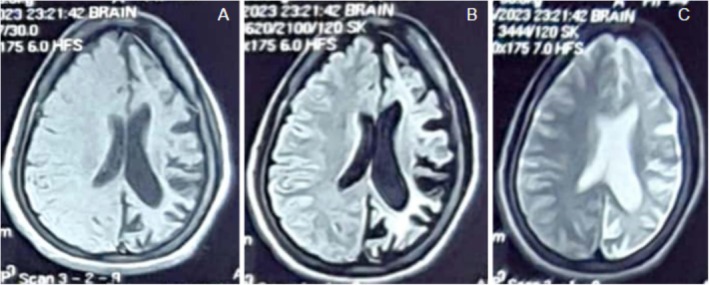 FIGURE 2
FIGURE 2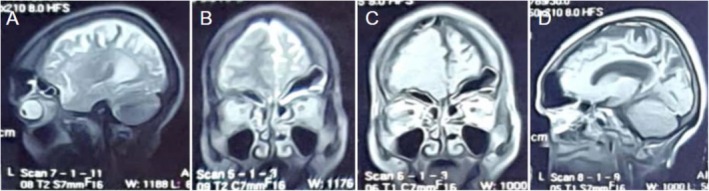 FIGURE 3
FIGURE 3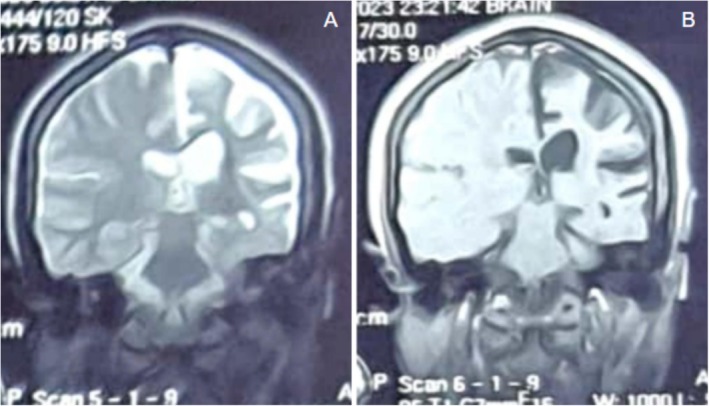 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Head and Neck Surgical Oncology · Bone health and treatments
Introduction
1
Dyke‐Davidoff‐Masson syndrome (DDMS) is an uncommon neurological disorder characterized by cerebral hemiatrophy with compensatory hypertrophy of the skull and sinuses [1]. The syndrome can be congenital or acquired and was first described in 1933 [1]. Congenital DDMS is thought to be caused by prenatal vascular insults such as intrauterine infections, ischemic insults, or congenital malformations [2]. Acquired DDMS, on the other hand, occurs after birth and is produced by ischemic strokes, infection, trauma, or any other underlying cause that produces chronic brain damage [3].
Neurological deficits include seizures, hemiparesis, and cognitive deficits that are often seen with DDMS [3]. Seizures are typically the most common symptom and are often refractory to treatment [4]. Hemiparesis may be progressive and is usually contralateral to the affected hemisphere [5]. The level of intellectual handicap is determined by the extent of the brain affected [6]. Neuroimaging studies are vital to distinguishing DDMS from other causes of cerebral hemiatrophy such as Rasmussen's encephalitis, Sturge–Weber syndrome, or congenital ischemic insults [3].
A 25‐year‐old woman with epilepsy, developing right‐sided hemiparesis, and intellectual impairment is the subject of this case report of DDMS. We review the radiologic and clinical characteristics, emphasizing the importance of MRI in diagnostic evaluation.
Case Presentation
2
A 25‐year‐old woman presented to our clinic with a history of chronic seizures only partially managed by antiepileptic drugs. Over the past few years, the patient has experienced progressive cognitive decline and the insidious onset of right‐sided weakness. No previous neuroimaging history was present.
Upon examination, the patient had hyperreflexia, elevated muscular tone, and right‐sided hemiparesis. Gait analysis showed a spastic pattern, and the right hand and foot had minor contractures. The patient had mild cognitive impairment, with specific deficits in complex problem‐solving and memory.
An MRI of the brain showed ex‐vacuo dilatation of the ipsilateral lateral ventricle and left‐sided cerebral hemiatrophy (Figure 1). There was also dilatation of the frontal and sphenoid sinuses, thickening of the ipsilateral calvaria, and hyperpneumatization of the mastoid air cells (Figure 2). The cerebellum, internal capsule, and right basal ganglia appear intact. Lack of aberrant post‐contrast enhancement ruled out active inflammatory or neoplastic processes.
(A) Coronal T2‐weighted MRI showing left hemicerebral atrophy with ex‐vacuo dilatation of the left lateral ventricle. (B) Coronal T1‐weighted post‐contrast MRI displaying similar findings with no abnormal enhancement.
(A) Hemicerebral atrophy. (B) Ex‐vacuo dilatation of the ipsilateral lateral ventricle. (C) Ipsilateral calvarial thickening. Imaging findings demonstrate varying degrees of cerebral hemiatrophy with associated compensatory hypertrophy of the skull and sinuses.
MRI findings confirmed left‐sided cerebral hemiatrophy with calvarial thickening, hyperpneumatization of ipsilateral mastoid air cells, and compensatory sinus hypertrophy (Figures 3 and 4). Based on these findings, Dyke‐Davidoff‐Masson syndrome was diagnosed. The patient was referred for neurological follow‐up and physiotherapy to manage her motor impairments, and her antiepileptic medication was modified to better control her seizures. To evaluate the course of the condition and improve treatment approaches, long‐term surveillance was suggested.
(A) T1 sagittal MRI showing hypertrophy of the left frontal and ethmoid sinuses with left calvarial thickening. (B) T2 coronal MRI demonstrating left hemicerebral atrophy. (C) T1 post‐contrast coronal MRI. (D) T1 post‐contrast sagittal MRI.
(A) T2 coronal MRI showing hyperpneumatization of left mastoid air cells with slight elevation of the left petrous ridge. (B) T1 post‐contrast coronal MRI demonstrating left lateral ventricle dilation and calvarial thickening.
Differential Diagnosis
3
Another factor to take into account is Sturge–Weber syndrome, which likewise involves unilateral brain involvement. Leptomeningeal angiomatosis and distinctive facial port‐wine stains, which are not present in DDMS, are indicative of this neurocutaneous condition. Furthermore, Sturge–Weber syndrome manifests as increasing calcifications in impacted brain areas that are visible on imaging tests.
Asymmetric cerebral atrophy, which resembles DDMS, can be caused by perinatal ischemia traumas. The typical compensatory bone and sinus enlargement associated with DDMS is typically absent in these patients, though. Another possible differential is hemimegalencephaly, a developmental abnormality marked by an enlarged rather than atrophic hemisphere. On neuroimaging, hemimegalencephaly can be distinguished from DDMS by its cortical thickness and excessive gyration.
In light of these factors, MRI is essential for distinguishing DDMS from other causes of unilateral cerebral atrophy. One characteristic that continues to help in diagnosis is the combination of sinus hypertrophy, compensatory skull thickening, and cerebral hemiatrophy.
Conclusion and Results
4
The patient was referred for neurological follow‐up and physiotherapy. Her antiepileptic medication regimen was adjusted to enhance seizure control. Long‐term surveillance was recommended to monitor disease progression and optimize symptom management. Early intervention in such cases improves mobility and quality of life.
Discussion
5
Dyke‐Davidoff‐Masson syndrome (DDMS) is a rare neurologic disorder first described in 1933 and characterized by cerebral hemiatrophy with secondary skull changes, including calvarial thickening and frontal and mastoid sinus hyperpneumatization [7]. The present case is in accord with classical imaging findings of DDMS, like left‐sided brain atrophy, ipsilateral ventricular dilatation, calvarial thickening, and frontal and mastoid sinus hyperpneumatization [8].
The etiopathogenesis of DDMS is traditionally categorized as acquired or congenital. Congenital types are usually caused by intrauterine vascular insults or brain developmental malformations [9]. Acquired DDMS, by contrast, is usually caused by postnatal brain insult such as trauma, infection, ischemic stroke, or febrile seizures in early life that persist for a prolonged duration [3].
Our patient presented with progressive seizures, right‐sided weakness, and impaired cognition—features characteristic of the most common clinical presentation of DDMS [10]. Seizures in DDMS are generally resistant to standard antiepileptic treatment and may require polytherapy or surgery in severe cases [11]. The motor deficits, particularly hemiparesis with spasticity and contractures in this case, are commonly progressive and have a significant role in producing disability [12].
DDMS diagnosis is radiologically directed. MRI would reveal unilateral cerebral atrophy, ipsilateral ventriculomegaly, and compensatory features such as skull thickening and hyperpneumatization of sinuses [8]. The findings above can distinguish DDMS from disorders that mimic its similar neurological presentation. Rasmussen's encephalitis, for example, can have unilateral atrophy and seizures but in the absence of DDMS's compensatory skull changes [11]. Sturge–Weber syndrome, a differential diagnosis, consists of leptomeningeal angiomatosis and characteristic facial port‐wine stains, both of which were absent in our patient [7].
For our patient, absence of post‐contrast enhancement on MRI further excluded inflammatory and neoplastic etiologies, making the diagnosis of DDMS more likely [3]. Ipsilateral hypertrophy of calvaria and sinus is pathognomonic and typically accompanies cerebral insult of early life [8].
Management of DDMS is multidisciplinary. Seizure is managed with antiepileptic drugs, although surgery such as hemispherectomy can be considered in resistant cases [11]. Physiotherapy also becomes significant in motor rehabilitation, particularly to manage spasticity and prevent fixed deformities due to contractures [12]. Cognitive therapy and follow‐up over a long period of time also play significant roles, particularly in intellectual impairment patients [3].
This case illustrates the importance of early neuroimaging in chronic, drug‐resistant seizures and unilateral motor deficit. Identification of the pathognomonic features of DDMS can guide diagnosis and encourage multidisciplinary intervention, perhaps to improve long‐term prognosis [9].
Author Contributions
Quang La: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, visualization, writing – original draft, writing – review and editing. Aiman Baloch: conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, writing – original draft, writing – review and editing. Muhammad Ayub: data curation, supervision, validation, writing – original draft, writing – review and editing. Sobia Ahmed: supervision, validation, writing – original draft, writing – review and editing. Enoch Lue: writing – original draft, writing – review and editing.
Consent
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Al‐Smair , S. A. Hafez , A. Saadeh , and A. Al‐Ali , “An Adult With Dyke–Davidoff–Masson Syndrome: A Case Report,” Cureus 14, no. 3 (2022): e 23315, 10.7759/cureus.23315.35464553 PMC 9015058 · doi ↗ · pubmed ↗
- 2“Abstracts of ESPR 2013, the European Society of Paediatric Radiology 50th Annual Meeting and 36th Postgraduate Course. June 3–7 2013. Budapest, Hungary,” Pediatric Radiology 43, no. Suppl 3 (2013): S 475–S 656, 10.1007/s 00247-013-2675-4.23613005 PMC 3679720 · doi ↗ · pubmed ↗
- 3U. Pradeep , A. Chiwhane , S. Acharya , P. Kumar , and P. Kasat , “Dyke‐Davidoff‐Masson Syndrome: A Rare Case of Hemiatrophy With Chronic Seizure Disorder,” Radiology Case Reports 20, no. 3 (2024): 1470–1474, 10.1016/j.radcr.2024.11.060.39811048 PMC 11730932 · doi ↗ · pubmed ↗
- 4I. Zawar , A. A. Khan , T. Sultan , and A. W. Rathore , “Dyke‐Davidoff‐Masson Syndrome. An Unusual Cause of Status Epilepticus,” Neurosciences (Riyadh) 20, no. 4 (2015): 385–387, 10.17712/nsj.2015.4.20150481.26492121 PMC 4727633 · doi ↗ · pubmed ↗
- 5P. A. Thakkar and R. H. Dave , “Dyke‐Davidoff‐Masson Syndrome: A Rare Cause of Cerebral Hemiatrophy in Children,” Journal of Pediatric Neurosciences 11, no. 3 (2016): 252–254, 10.4103/1817-1745.193365.27857800 PMC 5108134 · doi ↗ · pubmed ↗
- 6A. Sachdev , S. Acharya , J. H , and S. Huse , “A Rare Case of Dyke‐Davidoff‐Masson Syndrome in an Adolescent Female,” Cureus 16, no. 3 (2024): e 56377, 10.7759/cureus.56377.38633966 PMC 11022166 · doi ↗ · pubmed ↗
- 7P. Singh , K. Saggar , and A. Ahluwalia , “Dyke‐Davidoff‐Masson Syndrome: Classical Imaging Findings,” Journal of Pediatric Neurosciences 5, no. 2 (2010): 124–125, 10.4103/1817-1745.76108.21559157 PMC 3087988 · doi ↗ · pubmed ↗
- 8A. Al Hatmi , T. Almashaikhi , and E. Al Ajmi , “Imaging Features of Dyke‐Davidoff‐Masson Syndrome,” Sultan Qaboos University Medical Journal 23, no. 1 (2023): 122–124, 10.18295/squmj.9.2022.055.36865414 PMC 9974030 · doi ↗ · pubmed ↗