Enhancing Safety Culture for Formal Caregivers in Long-Term Care: A Rapid Review
Mathias Haeger, Sandra Garay, Kristin Krieger, Simon Eggert

TL;DR
This paper reviews strategies to improve safety culture for caregivers in long-term care, highlighting the need for better interventions and measurement tools.
Contribution
The study provides a rapid review of recent strategies and factors influencing safety culture in long-term care settings.
Findings
Few intervention studies exist, and findings remain heterogeneous.
Critical incident reporting systems and staff training are emphasized as beneficial.
No gold standard measurement instrument for safety culture was identified.
Abstract
Aim: This study explores the latest intervention strategies, contributing factors, and measurement instruments aimed at enhancing safety culture in long-term care settings. Background: A positive safety culture is associated with increased patient safety. While strategies to enhance safety culture are well documented in medical and clinical settings, evidence from the long-term care sector remains limited. Furthermore, the literature is heterogeneous regarding contributing factors and measurement approaches. Strengthening the understanding of how to enhance safety culture in long-term care could raise safety awareness among formal caregivers working with this highly vulnerable population of older adults. Methods: A rapid integrative review was conducted to update our previous work on interventions. Relevant empirical and theoretical studies were retrieved from eight databases. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
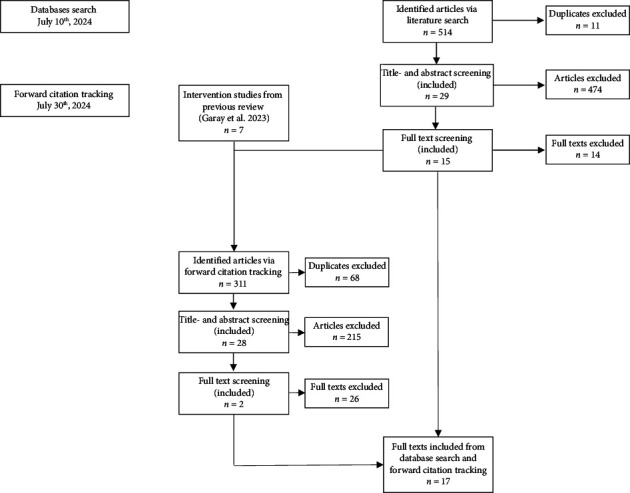 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational Health and Safety Research · Risk and Safety Analysis · Patient Safety and Medication Errors
1. Introduction
Healthcare is facing a global challenge in ensuring patient safety [1]. This concern, however, has not received the same level of attention in long-term care. The increasing life expectancy and demographic changes are adding to the burden on the care system. The complexity of care for older adults, including psychological and physiological disorders and extensive medications, requires appropriate qualifications to avoid adverse events [2]. A study revealed that nurse leaders identified a lack of knowledge in providing care as an important reason for safety concerns [3]. Safety and high-quality care are crucial for care-dependent people, formal caregivers, and relatives. Formal caregivers in in-home care or nursing homes can influence safety and the quality of care through a positive organizational culture [4, 5]. The construct of organizational culture includes safety culture [5], which is often defined as shared beliefs, values, competencies, and behaviors within a team targeting a reduction of safety-related problems [6–8]. In addition, a difference also lies between the terms “culture” and “climate,” as Churruca and colleagues (2023) explain: “Culture” is the deeper underlying construct of “climate” as its surface-level manifestation [4]. In previous publications, our group has referred to this perspective and defined safety climate as a kind of measurable snapshot of the underlying safety culture [7, 9]. However, it is impossible to separate both clearly. Thus, we focus on safety culture and imply the safety climate measurement.
Improving safety culture in long-term care settings holds the potential for significant positive outcomes. Previous studies have shown that an enhanced safety culture is associated with fewer adverse events [10, 11]. Moreover, higher scores in safety culture predict better quality performance indicators (i.e., reduced deficiency citations for healthcare and fewer substantiated complaints) in nursing homes [12]. An initial safety culture assessment in an organization plays an essential role in its further development, as it informs about the status quo of safety culture and provides the opportunity to shift the staff's attention towards it [13, 14]. There are numerous validated instruments to evaluate the safety culture in long-term care facilities. However, they are not readily applicable across countries. Known instruments are, for example, the Canadian Patient Safety Culture Survey (Can-PSCS) Tool [15], the Manchester Patient Safety Framework or “Culture is Key” [16], the Nursing Home Survey of Patient Safety Culture (NHSOPSC) [17], and the Survey on Resident Safety in Nursing Homes (NRS) [18]. A collection of instruments to assess safety culture in long-term care settings could be useful for researchers and nurse managers. Choosing the most appropriate instrument from a collection of possible instruments (e.g., regarding setting, objective, and length) could serve as a starting point to evaluate the facilities' safety culture. Based on the assessment result, this creates the opportunity to decide which areas of safety culture to target. It should also be noted that simply conducting a safety culture survey could already impact it [14, 19].
Literature indicates that, for example, interventions to reduce stress and professional burnout, the implementation of a registry or reporting system of incidents/adverse events, staff training, or the collegial exchange of experiences might be beneficial for improving the safety culture in long-term care facilities [7, 20]. A recent review highlighted various published approaches (n = 57 strategies) to support management and staff in strengthening patient safety culture [21]. The authors divided these strategies into two categories: recommendations (i.e., focusing on teamwork, communication, and leadership) and actions (i.e., active participation and commitment to safety practices). This demonstrates that many factors could be considered in the context of safety culture interventions, which play into the fact that safety culture is a complex construct.
Much new research emerged on the topic, since the conclusions of our latest work were based on the literature search from 2020. At the same time, long-term care providers depend on the latest evidence to implement and sustain a positive safety culture in their organizations. Because of that, we undertook this update of previous work on safety culture interventions for nursing professionals in long-term care and an extension of our work regarding the measurement and contributing factors of safety culture. We therefore aimed to collect up-to-date evidence on methods linked to safety culture in the long-term care setting. The research was guided by the primary research question:
-
- Which studies published since May 2020 describe interventions aimed to enhance safety culture in long-term care on a team or facility level?
The secondary research questions addressed factors associated with safety culture in long-term care:
- 2. Have there been new instruments for assessing the safety climate on the team or facility level in long-term care since May 2020?
-
- What implications exist for reporting systems from intervention studies on safety culture in long-term care published since May 2020?
-
- Which factors have a measurable or subjective reported impact on safety culture in long-term care at the team or facility level, according to the intervention studies published since May 2020?
2. Methods
2.1. Design
This rapid review adopted an integrative approach to examine the context, including diverse study designs [22–24]. The five-stage integrative review method was followed: problem identification, literature search, data evaluation, data analysis, and presentation [25]. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for the search strategy and the reporting of results, including precise research questions, a systematic search, screening and selection based on defined inclusion/exclusion criteria, data extraction, and synthesis as well as analysis of evidence [26]. Since this is an update of a previous study, we included studies published between 2020 and 2024. This review was preregistered in PROSPERO with the following ID: CRD42024570096.
2.2. Search Strategy
We included studies from PubMed (MEDLINE database) and EBSCO (including databases APA PsycArticles, APA PsycINFO, CINAHL, ERIC, PSYNDEX Literature with PSYNDEX Tests, and SocINDEX). Additional literature was identified by forward citation tracking of eligible studies and intervention studies from our previous work [7]. We focused on three areas of interest combined with an AND-operator: (I) the population (ambulatory care OR outpatient care OR agencies, home care OR long-term care OR nursing homes) as MeSH-term or title/abstract search, (II) interventions/concepts (training^∗^ OR education OR program^∗^ OR method^∗^), and (III) the context ((patient AND safe^∗^) OR (safe^∗^ AND culture) OR (risk AND manage^∗^) OR (safe^∗^ AND manage^∗^) OR (error AND manage^∗^) OR (safe^∗^ AND climate) OR (safe^∗^ AND measure^∗^) OR (medi^∗^ AND error) OR (nurs^∗^ AND error) OR (adverse AND event)) as title/abstract search. A more detailed example of our search strategy, including the syntax, is available on the PROSPERO registry. For all studies, the following inclusion and exclusion criteria were applied (Table 1).
2.3. Review Process
All studies were transferred from the databases to the tool Covidence for the title, abstract, and full-text screening. The first 50 studies in the title and abstract screening were used as exercises and discussed within the research team after an independent review (SG, KK, and MH). In the process, each study was screened and later extracted independently by two researchers (SG and MH). A third reviewer (KK) checked each conflict.
2.4. Data Extraction
The tool Covidence was also used for data extraction, including exporting to Microsoft Excel. Extracted data included the study objective and design, country, methods, population/setting, measurements/tools, a description of concepts/interventions, and results.
2.5. Assessment of Methodology/Risk of Bias (RoB)
Two reviewers (KK and MH) independently judged the RoB in relevant results, and disagreements were discussed until a consensus was reached. Characteristics of interest were, for example, randomization, confounding, or missing outcome data. Since we included different study designs, we used the appropriate assessment tools: RoB-2 tool for randomized controlled trials [27], ROBIS for reviews [28], AXIS for cross-sectional studies [29], and the JBI checklist for qualitative studies [30].
2.6. Data Analysis and Synthesis
The extracted data and the RoB assessment were reported descriptively with a narrative presentation of the overall results structured by the research questions.
3. Results
3.1. Descriptive Results
A total of 825 studies were identified via database search and citation tracking. We excluded 79 duplicates, 689 studies in the title and abstract screening, and 40 more in the full-text screening. Finally, 17 studies were eligible regarding our research questions (Figure 1). All studies included were conducted in nursing homes or residential care facilities. No study from in-home care agencies or semiresidential facilities was included. Some studies showed overlaps regarding our research questions; thus, we found one intervention study, seven studies that mentioned new or updated instruments, four studies that discussed implications on Critical Incident Reporting Systems (CIRS), and ten studies that described contributing factors to safety culture. Table 2 presents the characteristics of the included studies.
3.2. RoB Assessment
Most studies in this review were cross-sectional trials (n = 10). The RoB estimations in the AXIS tool ranged from 11 to 19 positive out of 20 possible answers, with a mean value of 16. In detail, more than half of the included studies did not justify their sample size [35, 37, 38, 41, 43, 45], did not address or categorize nonresponders [32, 34, 35, 37, 38, 41, 43, 46], and offered no information on nonresponders [32, 35, 37, 38, 41, 43, 46]. In six studies, the selection process was not likely to select participants that were representative of the target population [34, 35, 38, 41, 43, 46]. The qualitative studies (n = 3), assessed using the JBI, showed a mean of 8 out of 10 possible positive answers. Two studies did not address the role of the researcher in the process (own cultural and theoretical orientation) and the representation of participants and their voices [31, 47]. The reviews (n = 3) were assessed with ROBIS. Two showed a low RoB [33, 40], and one review did not adequately address the potential RoB from the study identification and selection process and thus was rated with an overall high RoB [39]. The RCT was rated at a high RoB, since one domain (measurement of the outcome) showed a high RoB [44].
3.3. Implications to Enhance Safety Culture
3.3.1. Interventions to Enhance Safety Culture
We identified one intervention study that implemented a training package on safety culture in French nursing homes [44]. The package included a strategy to report and analyze adverse events associated with care, including clear definitions, examples, reporting tools, and a steering group responsible for analyzing and defining an action plan. Nursing homes were provided with methodological support given in four different sessions to raise awareness of taking ownership of the project, raise awareness among nursing home staff to report events, train the steering group on how to structure their work, analyze adverse events, and observe how the steering group handled critical adverse events. The intervention showed only for the seventh dimension (“Feedback and communication about incidents”) of the NHSOPSC a significant improvement from pre to post [44].
3.3.2. Instruments to Assess Safety Culture
Seven studies were identified which reported or used instruments to measure safety culture in nursing homes: The CLC Employee Survey of Attitudes about Resident Safety (CESARS) [36–38], the Korean Patient Safety Culture Scale for long-term care facilities [34], the Adverse Event Reporting Obstacle Scale (AEROS) [32], the Occupational Health and Safety Council Safety Climate Questionnaire [39], and the Modified Stanford Patient Safety Culture Survey Instrument (MSI) [33]. All instruments reported acceptable validity and reliability. These instruments are new, since others (i.e., NHSOPSC) were already known from our previous review [7] and a report on safety culture [9]. In these previous studies, we identified the NHSOPSC, Culture is Key, Can-PSCS, Safety Attitudes Questionnaire (SAQ), and the NRS. All these instruments examine safety culture in residential or in-home care and therefore show some overlaps; however, we cannot indicate which instrument is most suitable.
3.3.3. Implications for the Implementation of Critical Incident Reporting Systems
We included four studies that used or described a critical incident reporting system and mentioned facilitators or barriers. It should be noted that there is currently no standard system to report adverse events or incidents in long-term care settings [40]. Scott et al. gave an overview of existing systems, captured types of incidents commonly reported, and highlighted that more standardized systems might improve cross-organizational learning. The authors also argued that digital reporting systems should be favored, as they reduce the workload of paper systems (i.e., data entry and evaluation) [40]. Another study described a facilitating effect of patient safety culture on reporting attitudes to adverse events [46]. Moreover, their results indicate that individual characteristics such as reporting awareness, education level, and working experience significantly influenced the staff's reporting attitude. Wang et al. concluded that nurse managers should simplify the reporting procedures to enable staff with a lower educational level to report incidents. Finally, the authors from one study noted that a lesson learned from incident management was to emphasize processing reported incidents at the organizational level transparently and to initiate solutions openly with the team to avoid the reoccurrence of safety incidents [42]. The authors assumed that not addressing lessons learned for the organization could lead to isolating learnings to only the individual employee rather than an opportunity for the whole organization to improve safety practices.
Three studies describe barriers to the implementation of a reporting system [35, 42, 46]. One study mentioned a high workload as a possible barrier to adverse event reporting. Especially when nurses lack time to complete their tasks in direct care, an additional duty, such as filling out a reporting for, may be neglected [46]. The authors also described hierarchical reporting and working conditions as a barrier since, for example, nurse assistants typically relay information orally to the head nurse and do not use a reporting system on their own [46]. Another study referred to nurses' negative emotions such as shame and guilt, a loss of confidence after experiencing conflicts or repercussions, and a lack of support from peers after reporting incidents [42]. Moreover, an examination of professionals' views on safety culture and incident reporting systems showed that the staff felt that the organization was neither learning from the system nor providing enough feedback [35]. The authors also assumed that there might be a reporting difference depending on the kind of incidents, i.e., falls that happened in the absence of a nurse might be easier to report since professionals are not usually held responsible for them.
3.3.4. Contributors to Safety Culture
In sum, 10 studies reported factors that contributed to safety culture. The identified factors can be grouped into organizational, care process–related, or staff-related aspects. At the organizational level, the included studies identified the implementation of training in safety culture practices (“risk management approach”) as well as an already initiated quality approach and a steering group that demonstrated leadership [44], organizational readiness to change at different levels (i.e., coworkers, supervisors, and senior managers) [36], or the facility scale (i.e., larger facilities), ownership (i.e. state-owned), and whether it was an integrated care institution which provided medical and aged care services as opposed to only aged care services [32] as aspects with a positive influence on safety culture. However, there were heterogeneous results regarding facility scale since another study showed that larger facilities and being attached to a hospital resulted in perceptions of a lower safety culture [43]. Regarding contributors to safety culture on the care process level, one study highlighted the division of roles according to expertise, smooth information sharing, open communication, as well as an active participation in the development of care-related rules and respectful relationships between professions as beneficial for safety culture [47]. Another study pointed out that good reporting management of adverse events might improve safety culture [32]. Besides that, the authors described the reported frequency of concerns regarding patient safety, the occurrence of actual adverse events in the departments, and a punitive atmosphere as further influencing aspects [32]. Finally, there are staff-related aspects that might improve safety culture. With this, two studies showed that the length of service (work experience) [37] as well as staff turnover of registered nurses and certified nurse assistants [45], had a negative effect on the perception of safety culture. To navigate that, Quach et al. (2021) suggested pairing experienced workers with newer ones to narrow potential knowledge gaps and increase collaboration. In addition, huddles, team meetings, and organizational initiatives could facilitate recognizing and leveraging experienced workers' accumulated safety knowledge [37]. Higher reporting attitudes and reporting awareness of adverse events were associated with a higher perception of safety culture [46]. Furthermore, two studies linked a positive safety culture to leadership behavior [31, 41]. In detail, Seljemo et al. reported that transformational leadership, defined by idealized influence, inspirational motivation, intellectual stimulation, and individualized consideration, was linked to a better safety culture. Engle et al. described leadership support, communication, and responsiveness as core influential factors in the staff's perceived safety culture. The authors stated that in facilities with a higher safety culture, staff had the sense that people in positions above them in the hierarchy were open to conversations, were approachable, and were physically present to have face-to-face conversations; moreover, they found their nurse managers and senior managers to be supportive and approachable [31]. On an individual staff-related level, skill utilization and job demands (i.e., work pace and emotional workload) influenced safety culture [41].
4. Discussion
This review updates previous work, focusing on interventions to improve safety culture in long-term care. Between 2020 and 2024, we identified 17 studies, including only one intervention study. Other aspects of interest were instruments for measuring safety culture, implications for implementing CIRS, and factors that might influence safety culture in long-term care settings. Even if the findings on new intervention studies are marginal, this integrative review provides a beneficial overview for the development of future intervention studies and research projects.
The intervention study implemented a training package to improve the reporting and analysis of care-related adverse events and safety culture in nursing homes. It was shown that the 7^th^ dimension of the NHSOPSC, namely, “feedback and communication about incidents,” improved in the facilities [44]. It seems appropriate, as some training content (i.e., raising awareness, available tools, and empowering some professionals to analyze events and provide feedback) was also related to this area. Such intervention content is partly in line with previous studies that, for example, intended to facilitate the collegial exchange of experiences and learnings and create an environment of reporting and learning from mistakes [7]. Overall, however, the approaches and results of intervention studies are too heterogeneous to allow targeted comparisons and to identify the most effective interventions. Thus, as previous studies stated [20, 48], further intervention research is still required.
To give further recommendations on intervention designs, we also examined existing measurement instruments for safety culture, CIRS (due to their proximity to safety culture), and factors influencing safety culture. Some of the instruments, several of which have been validated in different languages, were already known from our previous work. The current research adds the CESARS, the Korean Patient Safety Culture Scale for long-term care facilities, the AEROS, the Occupational Health and Safety Council Safety Climate Questionnaire, and the MSI. These instruments were identified in response to our second research question and serve to broaden the overview of available tools. However, it must be noted that this overview may not be exhaustive, as the search strategies of both reviews were not specifically tailored to identify measurement instruments. Therefore, the intention here is to offer guidance on potentially useful instruments for assessing safety culture in long-term care settings. Although all included instruments were described as validated, no single one has been established as a “gold standard” or received official recommendation, unlike in the hospital setting, where, for example, the European Commission has issued guidance [49]. One recommended instrument is the Hospital Survey of Patient Safety Culture (HSOPSC) [50], which has also been adapted for nursing homes and has recently been validated in a short version [51]. This short version focuses on four key dimensions of safety culture: (i) safety improvement actions, (ii) teamwork, (iii) information flow, and (iv) management support. Other instruments may emphasize similar or distinct areas, such as responses to mistakes and errors. In practice, the decision in favor or against a particular instrument therefore depends on which dimensions of safety culture should be addressed and evaluated in the context of the intervention. The results of an initial safety culture survey can help identify areas with room for improvement before an intervention is implemented. Follow-up assessments can then indicate whether the steps taken had an impact on the previously identified dimension. In addition to selecting a suitable instrument, incorporating patient safety quality indicators, such as falls, pressure ulcers, or use of physical restraints, may enhance evaluation efforts [33]. These indicators allow to reveal changes in the quality of care as a proxy for improvements in safety culture. Combined feedback from measurement tools and quality indicators can presumably improve the effectiveness of interventions in safety culture.
In addition to the instruments described above, CIRS can contribute to safety culture by recording and evaluating safety-related incidents. Four of the included studies examined correlations between the use of reporting systems and safety culture [35, 40, 42, 46]. It was shown that safety culture is related to the reporting attitude of adverse events [46], that organizational learning processes can be improved [42], and that the data from reported incidents allow conclusions to be drawn about safety culture [35]. The link between reporting systems and safety culture can be used to learn specifically from incidents by reviewing and discussing them with the team. A standardized system used in different facilities could also be valuable for cross-organizational learning [40]. Regarding data evaluation and feedback processes, a digital system would be preferable to an analog one (i.e., paper and pencil) [40]. In addition, it could be helpful to use reporting and learning systems or appropriate training as an intervention approach to improve safety culture, as was intended in the intervention study mentioned above [44]. However, reporting systems not only affect an organization's safety culture but their outcomes also depend on the preexisting safety culture on site: WHO describes that incident reporting and learning systems can only be meaningfully advanced based on a cultural change toward a positive safety culture [1].
Besides reporting systems or measurement instruments, which in themselves can already positively influence safety culture [19], other factors can be intervention content. Therefore, it is essential to note that safety culture is a complex construct that is part of the organizational culture [5, 52]. Thus, it could be recommended that interventions address several factors rather than a single one. These factors can, for example, affect the organization, the care process, and the staff. We differentiated the included studies into these areas, whereby some overlaps also become clear: For example, the “organizational readiness to change” [36] can not only address single professionals but can also be understood as overarching for the entire organization. Furthermore, open communication, better information sharing, or good incident reporting management [32, 47] are process-related factors that could also be addressed through personal training of nursing managers [31, 41]. Therefore, adapting a process should be linked to staff training about the implementation. Such overlaps on individual and organizational levels show that factors influencing the safety culture often cannot be clearly separated, which suggests intervention approaches connecting the different levels. This is in line with a recent study that pointed out that a combination of different methods (i.e., communication, teamwork, and active leadership) might be beneficial for strengthening safety culture in the healthcare sector [21].
4.1. Limitations
Our study has some limitations that should be discussed. The included RCT was rated at a high RoB, and therefore, the significant effects regarding the 7^th^ dimension of the NHSOPSC should be considered carefully. This is comparable to our previous study, in which all included studies showed an overall critical RoB [7]. Therefore, the effect of the contents or strategies of all intervention studies included in our last reviews must be considered cautiously and should only be used as an indication for further studies. The overall RoB from the other included studies was, in sum, moderate, with a small RoB in five studies [33, 36, 40, 42, 45]. However, other limitations must be considered even if the risk is lower in the nonintervention studies. We have limited the search period for our secondary research questions to restrict the literature included. Nevertheless, this point limits the informative value: Studies on measurement instruments and reporting systems may be missing, or important factors influencing the safety culture may not be taken into account. Furthermore, we excluded short-term care, palliative care, psychiatric care, the care of younger people, and care of people with disabilities, which limits the significance of our results in the long-term care of older adults. Finally, we also excluded the clinical care setting, as, in our view, the results cannot thoroughly be transferred between the settings, especially as other studies indicate setting-related differences in the perception of safety culture [35].
4.2. Implications for Nursing Management
To effectively enhance safety culture in long-term care settings, nursing management should adopt a multifaceted strategy that integrates organizational development and staff support. A strong safety culture requires conscious and sustained leadership efforts to create an environment in which safety is understood as a shared responsibility, not a source of blame. Nurse leaders play a central role in fostering open communication and psychological safety, encouraging staff engagement in incident reporting and ensuring that lessons learned are reflected upon at the team level without fear of negative consequences. Regular training that promotes team-based reflection, simplified reporting procedures accessible across education levels, and emotional support after adverse events are key elements of such an approach. In addition, nurse managers should make use of validated safety culture measurement instruments to identify areas for improvement and monitor progress over time. Suggestions for appropriate instruments can be found in the results section and previous publications. Importantly, efforts to strengthen safety culture should be understood as long-term processes that ultimately support high-quality care.
5. Conclusion
Taking the current findings together with those of our previous review, several key conclusions can be drawn. First, intervention studies targeting safety culture in long-term care remain scarce, particularly in residential and home care settings. Since our last review, we identified only one additional intervention study in these areas. Second, the content and approaches of existing interventions remain highly heterogeneous. This diversity is understandable, given the multitude of factors that appear to influence safety culture, and the current lack of evidence regarding which of these factors are most critical. Nevertheless, each of the studies reviewed offers valuable insights into the nature, and collectively, they lay the groundwork for the development of targeted interventions. In this context, our reviews provide a foundation for informed intervention planning, including practical guidance on strategies, contributing factors, measurement instruments, and the role of reporting systems. For instance, the findings can help identify which dimensions of safety culture require improvement (based on measurement data) and guide the selection of appropriate intervention strategies to address relevant influencing factors. Since safety culture is a complex construct influenced by multiple overlapping factors, interventions are likely to be effective when they target several layers of safety culture simultaneously. In addition, the relationship between safety culture and reporting systems deserves further exploration, not least, because reporting systems themselves may serve as intervention tools. This potential has been highlighted in previous research [40] and warrants closer investigation. Finally, intervention planning must also carefully consider how to measure outcomes, given the absence of a gold standard for assessing safety culture. In our view, future research should prioritize two aims: (1) identifying the factors with the greatest influence on safety culture and (2) designing specific, evidence-based interventions targeting these factors. It is important to recognize, however, that developing a strong safety culture is a long-term process that requires sustained efforts and time.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization-WHO Global Patient Safety Action Plan 2021–2030: Towards Eliminating Avoidable Harm in Health Care 20211 st World Health Organization
- 2Ewers M. Lehmann Y. Jacobs K. Kuhlmey A. GreßS. Klauber J. Schwinger A. Hochschulisch Qualifizierte Pflegende in Der Langzeitversorgung?! University-Qualified Nurses in Long-Term Care?! Pflege-Report 2019: Mehr Personal in Der Langzeitpflege - Aber Woher? 2020 Berlin, Heidelberg Springer Berlin Heidelberg https://link.springer.com/10.1007/978-3-662-58935-9
- 3Eggert S. Sulmann D. Teubner C. Sicherheitskultur in Der Ambulanten Pflege ZQP-analyse 2020 Berlin https://www.zqp.de/wp-content/uploads/ZQP-Analyse-Sicherheitskultur Ambulant.pdf
- 4Churruca K. Falkland E. Saba M. Ellis L. A. Braithwaite J. An Integrative Review of Research Evaluating Organisational Culture in Residential Aged Care Facilities BMC Health Services Research 2023231 p. 85710.1186/s 12913-023-09857-y PMC 1042437637580765 · doi ↗ · pubmed ↗
- 5Pfaff H. Hammer A. Ernstmann N. Kowalski C. Ommen O. Sicherheitskultur: Definition, Modelle Und Gestaltung. Safety Culture: Definition, Models, and Design Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen 2009103849349710.1016/j.zefq.2009.08.0072-s 2.0-7224909107419998775 · doi ↗ · pubmed ↗
- 6Cooper Ph DM. D. Towards a Model of Safety Culture Safety Science 200036211113610.1016/s 0925-7535(00)00035-72-s 2.0-0034158686 · doi ↗
- 7Garay S. Haeger M. Kühnlein L. Sulmann D. Suhr R. Interventions to Enhance Safety Culture for Nursing Professionals in long-term Care: a Systematic Review International Journal of Nursing Studies Advances 20235 p. 10011910.1016/j.ijnsa.2023.100119 PMC 1108028738746586 · doi ↗ · pubmed ↗
- 8Guldenmund F. W. The Nature of Safety Culture: a Review of Theory and Research Safety Science 2000341–321525710.1016/s 0925-7535(00)00014-x 2-s 2.0-0034028034 · doi ↗