Synchronous Diagnosis of Ductal Carcinoma In Situ and Mucoepidermoid Carcinoma of the Parotid Gland: A Rare Case of Dual Primary Malignancy
Hesa A Salaibeekh, Hesa Alkaabi

TL;DR
A rare case is presented where a patient had two different cancers, ductal carcinoma in situ and mucoepidermoid carcinoma, diagnosed at the same time.
Contribution
This paper reports a unique case of dual primary malignancies occurring synchronously in a single patient.
Findings
A 76-year-old woman was diagnosed with both ductal carcinoma in situ and low-grade mucoepidermoid carcinoma.
The case highlights the rare coexistence of two distinct malignancies in the same patient.
Possible causes include coincidental tumor development, treatment effects, inherited predisposition, or hormonal influences.
Abstract
The coexistence of two histologically and anatomically distinct malignancies, ductal carcinoma in situ (DCIS) and mucoepidermoid carcinoma (MEC), in the same patient is a clinically rare phenomenon. MECs of the salivary glands, most often arising in the parotid, can display a range of histological grades and clinical courses. We report the case of a 76-year-old woman with a prior diagnosis of hormone receptor-positive DCIS who developed low-grade MEC of the parotid gland nearly a decade later. Possible etiologic factors discussed include coincidental tumor development, prior treatment effects, inherited predisposition, and hormonal influences. A focused literature-based discussion supports the analysis of this unique case.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
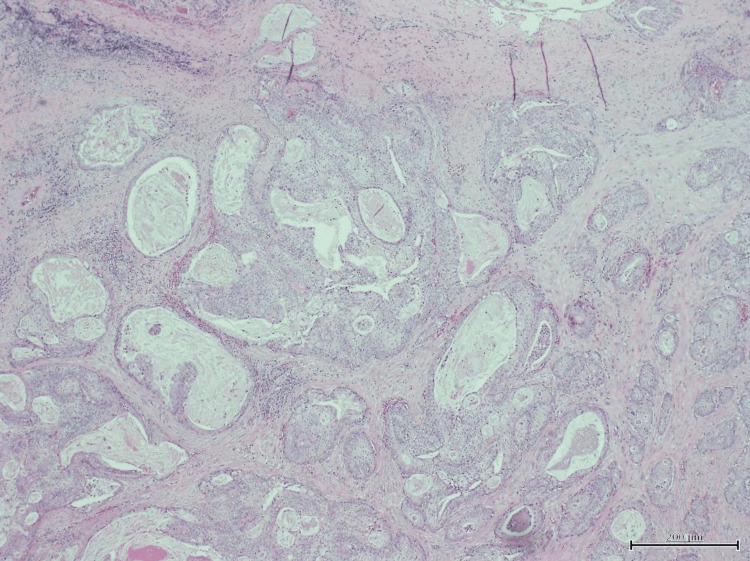 Figure 1
Figure 1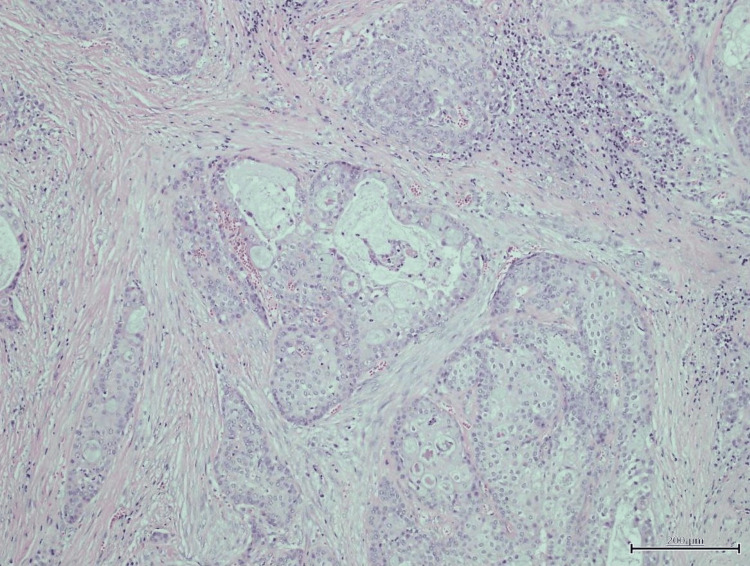 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Tumors Diagnosis and Treatment · Multiple and Secondary Primary Cancers · Neuroendocrine Tumor Research Advances
Introduction
The synchronous occurrence of two distinct primary malignancies, ductal carcinoma in situ (DCIS) of the breast and mucoepidermoid carcinoma (MEC) of the salivary gland, is a clinically rare phenomenon. This report describes a unique case involving a 76-year-old woman with a prior diagnosis of hormone receptor-positive DCIS who developed low-grade MEC of the parotid gland nearly a decade later.
DCIS is a non-invasive neoplastic proliferation of epithelial cells within the breast ducts, often asymptomatic and detected via routine screening mammography [1]. With the rising use of mammographic screening, the incidence of DCIS has increased significantly, and it now comprises up to 25% of newly diagnosed breast neoplasms in the Western world [2,3]. Management commonly includes breast-conserving surgery, radiotherapy, and adjuvant endocrine therapy for hormone receptor-positive tumors [4]. Long-term survival for DCIS exceeds 95%, and while recurrence can occur, distant metastases are rare in the absence of invasion [5].
MEC is the most frequently encountered malignant salivary gland neoplasm, accounting for roughly one-third of all cases, and arises primarily within the parotid gland [3,6]. It consists of mucin-producing, intermediate, and squamous epithelial cells and demonstrates diverse histopathological grades, which predict prognosis [7]. Low-grade MECs typically have favorable outcomes following surgical resection, while high-grade tumors may behave aggressively [6,8].
The occurrence of multiple primary malignancies, although uncommon, has been documented in cancer registries. Studies report that up to 10% of cancer survivors may develop a second primary cancer, particularly in the elderly population, where cumulative mutational burden, immune senescence, and longer post-treatment survival contribute to risk [9,10]. However, the co-presentation of breast DCIS and salivary MEC (tumors with disparate etiologies and anatomic origins) has not been reported in large series and thus warrants further exploration.
Case presentation
A 76-year-old Bahraini woman was diagnosed in 2014 with right breast DCIS after presenting with a palpable mass. Histopathological analysis confirmed grade 2 DCIS with HER2 overexpression (3+) and estrogen receptor (ER) and progesterone receptor (PR) positivity. Initial staging classified the disease as T1N1M0. She underwent breast-conserving surgery with negative margins and sentinel lymph node biopsy, followed by four cycles of adjuvant chemotherapy with epirubicin and cyclophosphamide (EC), and five years of letrozole. She did not receive radiotherapy due to favorable surgical margins and absence of invasive disease. Her surveillance mammograms remained unremarkable through April 2022.
In September 2023, she presented with a progressively enlarging, painless swelling in the left periorbital and preauricular region. Initial clinical suspicion was sialadenitis, and she received multiple empirical antibiotic courses without clinical improvement. Examination revealed a firm, mobile mass overlying the left parotid gland, without facial nerve involvement. There were no systemic signs such as fever, weight loss, or night sweats.
Neck ultrasonography demonstrated a heterogeneous, hypoechoic lesion within the superficial lobe of the left parotid gland. Fine-needle aspiration cytology revealed clusters of mucin-secreting and intermediate cells, with immunohistochemical positivity for CK7 and CK5/6, and strong mucicarmine staining. MRI confirmed a well-demarcated 2.2 cm lesion localized to the superficial parotid with no lymphadenopathy or perineural spread.
A superficial parotidectomy was performed with preservation of the facial nerve. Histopathological examination confirmed low-grade mucoepidermoid carcinoma, with negative margins and no lymphovascular invasion (Figures 1, 2). The patient’s recovery was uneventful, and she remains on oncologic follow-up.
Hematoxylin and eosin (H&E) stain, low-power view at 10x magnification showing infiltration by nests of tumor cells, some containing intraluminal secretions, within a fibroinflammatory stroma
Hematoxylin and eosin (H&E) stain, high-power view at 40x magnification showing infiltrative tumor cells composed of mucous cells, intermediate cells, and squamous cells, surrounded by desmoplastic stroma
Discussion
The concurrence of DCIS and MEC, two malignancies without overlapping histological lineage or anatomical continuity, prompts a multifaceted discussion. DCIS arises from ductal epithelial cells of the breast and is largely confined to the ductal system, while MEC originates in the salivary gland ductal reserve cells and demonstrates mucous and epidermoid differentiation [3,6].
The most plausible explanation is a coincidental occurrence of two primary malignancies. The incidence of multiple primaries in cancer survivors ranges between 4-10%, especially in patients over 70 years, as shown in Surveillance, Epidemiology, and End Results (SEER) data [9,11]. Dual cancers with no embryologic, hormonal, or treatment-related links are often reported in the literature as sporadic findings [10].
A secondary consideration is radiation exposure. Ionizing radiation has been conclusively linked to salivary gland carcinogenesis, particularly after therapeutic or environmental exposure during childhood [12]. Nevertheless, our patient did not receive radiotherapy to the breast or any region close to the head and neck. In modern radiotherapy protocols for breast cancer, scatter doses to distant tissues such as the parotid are negligible [13]. Thus, radiation-induced MEC is implausible in this case.
Genetic predisposition to multiple cancers must also be considered. Syndromes such as Li-Fraumeni (TP53 mutations), Cowden syndrome (PTEN mutations), and hereditary breast and ovarian cancer syndrome (BRCA1/2 mutations) have all been implicated in predisposition to multiple tumors [14,15]. However, MEC is not commonly associated with these syndromes, and our patient’s personal and family history was not indicative of a hereditary cancer syndrome. Additionally, MECs frequently harbor MAML2 fusions, which are not implicated in breast carcinogenesis [16].
Hormonal influences could also be hypothesized, given the hormone receptor positivity in DCIS and the patient’s exposure to systemic endocrine therapy. However, while androgen receptor expression has been noted in some salivary gland malignancies such as salivary duct carcinoma, there is scant evidence of ER or PR playing a role in MEC pathogenesis [17]. Williams et al. found that hormone receptors are variably expressed across salivary gland carcinomas, but MECs rarely express ER or PR in a functionally relevant manner [17]. Therefore, any hormonal link is weak and unsubstantiated.
Finally, the case highlights the clinical importance of maintaining diagnostic breadth in cancer survivors. Misattributing new symptoms to benign processes, such as infection or recurrence, can delay diagnosis. As in this patient, early biopsy and imaging of new lesions are essential to distinguish between recurrence, metastasis, or new primary tumors.
Conclusions
This report presents an unusual case of sequential DCIS and MEC in the absence of radiation exposure or hereditary cancer syndrome. While coincidence remains the most likely explanation, the case underscores the importance of comprehensive diagnostic evaluation in cancer survivors presenting with new symptoms. Ongoing advances in molecular oncology may eventually elucidate subtle links between disparate tumor types, but current evidence supports independent tumorigenesis in this case.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence of and treatment for ductal carcinoma in situ of the breast JAMA Ernster VL Barclay J Kerlikowske K Grady D Henderson C 91391827519968598618 · pubmed ↗
- 2Ductal carcinoma in situ of the breast: a systematic review of incidence, treatment, and outcomes J Natl Cancer Inst Virnig BA Tuttle TM Shamliyan T Kane RL 17017810220102007168510.1093/jnci/djp 482 · doi ↗ · pubmed ↗
- 3An update on grading of salivary gland carcinomas Head Neck Pathol Seethala RR 6977320092059699410.1007/s 12105-009-0102-9PMC 2807532 · doi ↗ · pubmed ↗
- 4Long-term outcomes of invasive ipsilateral breast tumor recurrences after lumpectomy in NSABP B-17 and B-24 randomized clinical trials for DCISJ Natl Cancer Inst Wapnir IL Dignam JJ Fisher B 47848810320112139861910.1093/jnci/djr 027PMC 3107729 · doi ↗ · pubmed ↗
- 5Breast cancer mortality after a diagnosis of ductal carcinoma in situ JAMA Oncol Narod SA Iqbal J Giannakeas V Sopik V Sun P 888896120152629167310.1001/jamaoncol.2015.2510 · doi ↗ · pubmed ↗
- 6Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria Cancer Goode RK Auclair PL Ellis GL 12171224821998952901110.1002/(sici)1097-0142(19980401)82:7<1217::aid-cncr 2>3.0.co;2-c · doi ↗ · pubmed ↗
- 7Salivary mucoepidermoid carcinoma: revisited Adv Anat Pathol Luna MA 2933071320061707529510.1097/01.pap.0000213058.74509.d 3 · doi ↗ · pubmed ↗
- 8Mucoepidermoid carcinoma: a clinicopathologic study of 80 patients with special reference to histological grading Am J Surg Pathol Brandwein MS Ivanov K Wallace DI 8358452520011142045410.1097/00000478-200107000-00001 · doi ↗ · pubmed ↗