A Propensity-Matched Cohort Study Assessing Neuropathy in Patients With Leukocytoclastic Vasculitis
Kritin K Verma, Sezim Minbaeva, Orson T Robertson, Ryan Koch, Daniel P Friedmann, Denise C Robson, Jonathan Aldrete, Michelle Tarbox

TL;DR
This study found that patients with leukocytoclastic vasculitis have a higher risk of developing neuropathy compared to a matched control group.
Contribution
The study provides the first propensity-matched evidence of an increased risk of neuropathy in patients with leukocytoclastic vasculitis.
Findings
5.4% of LCV patients had neuropathy compared to 4.6% of controls, with a relative risk of 1.209.
The association was statistically significant (95% CI: 1.009-1.448, p = 0.0396).
LCV may contribute to neuropathy through vasculitic damage to nerve blood supply.
Abstract
Objective The objective of this study was to examine the potential relationship between leukocytoclastic vasculitis (LCV), a small-vessel vasculitis, and neuropathy. While LCV primarily affects the skin, its systemic involvement, including the development of neuropathy, has been increasingly recognized. This study aimed to assess whether LCV patients have a higher risk of developing neuropathy compared to a demographically matched control group. Materials and methods This retrospective cohort study utilized data from the TriNetX database (TriNetX, LLC, Cambridge, Massachusetts, USA). A total of 4,519 patients diagnosed with LCV were matched with 4,519 control patients based on demographic factors such as age, sex, and race to ensure comparable baseline characteristics between groups. Neuropathy in both groups was identified using the ICD-10-CM diagnostic code G62.9. Statistical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
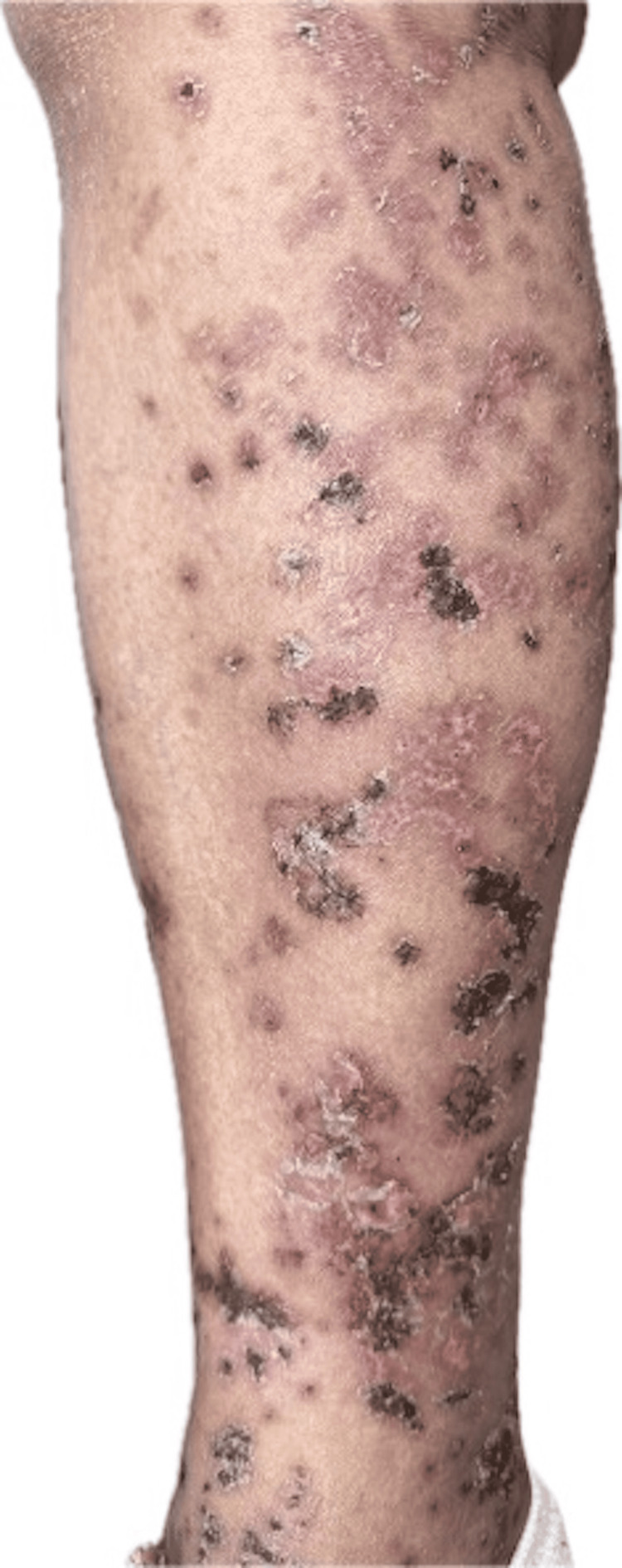 Figure 1
Figure 1| Characteristic | Cases (%) | Controls (%) | RR (95% CI)* | P-value* |
| Total Participants | 4,519 (100%) | 4,519 (100%) | - | 1.00 |
| Average age ± SD | 43.3 ± 22.9 | 43.3 ± 22.9 | - | 0.995 |
| Female | 2,304 (51.0%) | 2,298 (50.9%) | - | 0.003 |
| Male | 2,088 (46.2%) | 2,093 (46.3%) | - | 0.916 |
| Race | ||||
| White | 3,071 (68.0%) | 3,077 (68.1%) | - | 0.892 |
| Alaska Native | 23 (0.5%) | 19 (0.4%) | - | 0.536 |
| Native Hawaiian | 23 (0.5%) | 22 (0.5%) | - | 0.881 |
| Black | 332 (7.3%) | 334 (7.4%) | - | 0.936 |
| Asian | 157 (3.5%) | 153 (3.4%) | - | 0.817 |
| Ethnicity | ||||
| Non-Hispanic | 3,214 (71.1%) | 3,216 (71.2%) | - | 0.963 |
| Hispanic | 603 (13.3%) | 602 (13.3%) | - | 0.975 |
| Polyneuropathy, unspecified (ICD-10-CM Code: G62.9) | 243 (5.4%) | 206 (4.6%) | 1.209 (1.009-1.448) | 0.0396** |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Systemic Lupus Erythematosus Research · Atherosclerosis and Cardiovascular Diseases
Introduction
Leukocytoclastic vasculitis (LCV) is a type of small-vessel vasculitis that most classically results from an Arthus-type III hypersensitivity reaction, in which antigens complexed to IgG or IgM deposit in the walls of small blood vessels [1]. These immune complexes activate the complement system, leading to neutrophil infiltration and subsequent inflammation and damage to the vessel walls [2,3]. Clinically, LCV typically presents as palpable purpura and may rarely demonstrate urticarial lesions [1]. Histopathological examination is crucial for diagnosis and is marked by the presence of neutrophil infiltrate, often accompanied by fibrinoid necrosis of the vessel walls [1,3]. While mostly affecting the skin, systemic involvement, including neuropathy, is becoming more widely recognized [4,5]. In recent years, there has been an increasing awareness of the broader clinical implications of LCV, particularly its association with various neurological disorders [6], including peripheral neuropathy and central nervous system involvement [4,5]. Literature suggests that neuropathy in LCV may present in various forms, from sensory disturbances (e.g., paresthesia) to motor impairment, with some cases progressing from sensory to motor disturbances, highlighting the diverse manifestations of this condition [7,8]. This suggests that LCV is not only a dermatological concern but also potentially a multi-system disorder, making it critical to explore its broader impact. This study employs the TriNetX database (TriNetX, LLC, Cambridge, Massachusetts, USA), leveraging its large-scale real-world data, to investigate the relationship between LCV diagnosis and neuropathy [9,10]. Further research is needed to better understand this relationship, understand its underlying mechanisms, and develop targeted therapies that can address both the vascular and neurological components of the disease [5,9,11].
Materials and methods
Study design
This was a multi-institutional study conducted using retrospective, de-identified patient data from the TriNetX Research Network, which aggregates electronic medical records from multiple healthcare organizations across the United States. We conducted a retrospective cohort study using the TriNetX database to identify cases of LCV (Figure 1). The study was conducted in February 2025, during which we identified 4,519 instances of LCV using the ICD-10-CM codes D69.0 (LCV) and L95.8 (cutaneous LCV), analyzing the past 20 years of data [12]. To minimize potential confounding factors, we employed propensity score matching to select control subjects. The controls were matched by age, sex, and race using optimized algorithms available within the TriNetX platform [3].
Leukocytoclastic vasculitis visualized on the anteromedial aspect of the right lower leg.Image source: Original photograph contributed by Michelle Tarbox and Denise Robson (co-authors of this manuscript).
Inclusion and exclusion criteria
Inclusion criteria for this study were individuals with a diagnosis of LCV identified by ICD-10-CM codes D69.0 and L95.8. Exclusion criteria involved removing individuals who did not meet the matching criteria (age, sex, and race) or those without sufficient data within the TriNetX database to conduct a complete analysis [3].
Data collection
Data was collected from the TriNetX database, which includes a wide range of demographic information as well as diagnostic codes [3]. Neuropathy cases were identified through the ICD-10-CM code G62.9 (polyneuropathy, unspecified). This code was specifically chosen because other forms of neuropathy, such as diabetic or alcoholic neuropathy, would not fit into the category of LCV-induced neuropathy. We focused on collecting demographic data and the prevalence of neuropathy in patients with LCV compared to the control group.
Race and ethnicity data within the TriNetX platform are collected and recorded by participating healthcare organizations during routine clinical care. This information is typically self-reported by patients at the time of registration or intake and entered into electronic health records by clinical or administrative personnel. The data is de-identified and aggregated for research use within the TriNetX platform.
Statistical analysis
Demographic data and the prevalence of neuropathy were analyzed using Wald's method. We calculated risk ratios (RRs) and 95% confidence intervals (CIs) to assess the association between LCV and the development of neuropathy. Logistic regression analysis was used in congruence with Wald's method. Statistical significance was determined using a threshold of p < 0.05.
Results
The final cohort of 4,519 LCV patients and 4,519 matched controls was well-balanced in terms of sex (51% female in both groups) and age (mean 43.3 ± 22.9 years), with a similar racial distribution (68% White individuals in both groups). This careful matching strengthens the validity of the comparison by minimizing demographic confounding. The key observation was that neuropathy occurred in 5.4% (243/4,519) of LCV patients versus 4.6% (206/4,519) of controls, resulting in a relative risk (RR) of 1.209 (95% CI: 1.009-1.448; p = 0.0396) (Table 1).
**Table 1: Propensity-matched cohort analysis of demographics and neuropathy in patients with leukocytoclastic vasculitis from the TriNetX database.*After propensity score matching, Statistically significant values between cases and controls, defined at p < 0.05 using Wald's statistical testCI: confidence interval; CM: clinical modification; ICD: International Classification of Diseases; RR: risk ratio; SD: standard deviation
The RR of 1.209 indicates a 20.9% increased risk of neuropathy in LCV patients compared to controls. The 95% confidence interval (1.009-1.448) is particularly important because it excludes 1.0 at the lower bound, reinforcing that the risk elevation is not due to chance.
The p-value (0.0396) confirms statistical significance while suggesting that replication in larger cohorts could help strengthen these findings, but clinical relevance depends on context. Neuropathy, even at a modestly increased risk, can have meaningful consequences, such as chronic pain, sensory deficits, or mobility issues, particularly in patients already managing systemic inflammation from LCV. Since LCV is a vasculitic disorder, microvascular damage could contribute to nerve ischemia, potentially explaining the observed association.
The findings suggest that LCV patients may benefit from periodic neurological assessments, especially if they exhibit other risk factors (e.g., diabetes, alcohol use, or nutritional deficiencies that independently predispose to neuropathy).
The study’s matched design reduces confounding, but unmeasured variables (e.g., comorbidities, disease severity, or treatment differences) could influence the results. Future research could explore whether neuropathy in LCV patients follows a distinct pattern or whether tighter inflammatory control mitigates risk.
Discussion
The findings indicate a significant association between LCV and the development of peripheral neuropathy. This aligns with prior studies that have shown LCV, although classically presenting with skin manifestations, may extend past cutaneous symptoms to encompass neurological complications [5,11]. Neuropathy in LCV is thought to originate from ischemic damage produced by vasculitis inflammation of the vasa nervorum, the vessels which supply the peripheral nerve circulation [13,14]. Mononeuritis multiplex and polyneuropathy have been reported as severe symptoms of systemic vasculitis, with the latter uniquely presenting following recurrent tuberculosis infection [4,7,15].
Several mechanisms may underlie the connection between LCV and neuropathy [14]. Immune complex deposition in small arteries can cause inflammation, luminal narrowing, and ischemia in peripheral nerves and their blood supply [13,14]. Inflammatory responses are further intensified by the release of pro-inflammatory cytokines and other mediators, which may cause nerve damage and worsen vascular damage [13]. Although LCV is often linked to the skin and commonly manifests as palpable purpura [15], systemic involvement is not uncommon and may include abdominal pain, hematuria, and signs of peripheral nerve involvement [4].
The diagnosis of LCV-associated neuropathy can be difficult and may necessitate a combination of clinical examination, electromyography, nerve conduction investigations, and, in some cases, biopsy of affected tissues [4,6,8]. Skin biopsy may be especially beneficial to rule out medium and/or large vessel vasculitis [13].
LCV-associated neuropathy is often treated with immunomodulatory treatments to reduce the underlying vascular inflammation. Corticosteroids are frequently utilized as first-line treatment, and long-term maintenance may necessitate "corticosteroid-sparing" agents. In some patients, intravenous immunoglobulins or plasma exchange may help with acute exacerbations.
Limitations of this study include the reliance on ICD-10 codes for case identification, which may have resulted in some misclassification [16], as LCV diagnoses may have been categorized into broader categories or overlooked entirely due to coexisting conditions [6]. Furthermore, although varying degrees of neuropathy have been observed throughout the literature, the analysis makes no distinction between the types or degrees of neuropathy, which may affect the strength of the observed association [11]. Despite propensity-score matching, residual confounding from characteristics such as comorbid autoimmune diseases, medication use, or other unmeasured variables remains a possibility [15,17,18]. The TriNetX database, although reflective of real-world clinical practice, may not capture all relevant clinical details, and its use of broad diagnostic criteria may limit the accuracy and generalizability of the findings [6,10]. These limitations highlight the need for further research to refine diagnostic criteria and explore the mechanisms of neuropathy in LCV [6].
Conclusions
Although diagnosing LCV-associated neuropathy can be challenging, the study highlights the need for careful monitoring of neurological symptoms in patients with LCV. This study found a weak but statistically significant link between LCV and neuropathy, reinforcing the need for clinical awareness. Future research should concentrate on investigating this relationship whilst accounting for additional variables (e.g, comorbidities known to cause peripheral neuropathy).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hypersensitivity vasculitis 2024 https://emedicine.medscape.com/article/1083719-overview
- 2Leukocytoclastic vasculitis: a cutaneous expression of immune complex disease Arch Dermatol Mackel SE Jordon RE 2963011181982621114610.1001/archderm.118.5.296 · doi ↗ · pubmed ↗
- 3Etiologies and prognostic factors of leukocytoclastic vasculitis with skin involvement: a retrospective study in 112 patients Medicine (Baltimore) Bouiller K Audia S Devilliers H 095201610.1097/MD.0000000000004238 PMC 495682527428231 · doi ↗ · pubmed ↗
- 4Leukocytoclastic vasculitis associated with multifocal sensory neuropathy responsive to intravenous immunoglobulins: a case report Sarcoidosis Vasc Diffuse Lung Dis Ferranti M Cama E Cacciavillani M Schiavon F Felicetti M Briani C Alaibac M 038202110.36141/svdld.v 38i 3.10883 PMC 855257434744418 · doi ↗ · pubmed ↗
- 5A case of tuberculosis-related leukocytoclastic vasculitis presenting with peripheral neuropathy Cureus Rafiei N Khanlou N Khosa S Moheb N Mishra SK 010201810.7759/cureus.3703 PMC 637224930788192 · doi ↗ · pubmed ↗
- 6Diagnosis and management of leukocytoclastic vasculitis Intern Emerg Med Fraticelli P Benfaremo D Gabrielli A 8318411620213371328210.1007/s 11739-021-02688-x PMC 8195763 · doi ↗ · pubmed ↗
- 7Sensory mononeuritis multiplex: a rare sequela of leukocytoclastic vasculitis J Am Acad Dermatol Chohan TS Odedra S Salim A 0852021
- 8Leucocytoclastic vasculitic neuropathy diagnosed by biopsy of normal appearing skin J Neurol Neurosurg Psychiatry Yamanaka Y Hiraga A Arai K 7067077720061661404410.1136/jnnp.2005.077321 PMC 2117470 · doi ↗ · pubmed ↗