Nutraceutical Supplementation Effects on Subjective Fatigue Symptoms in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Systematic Review
Emanuella M Brito, Leonardo Bonifanti, Rajvi Patel, Jailene Jimenez, Jacqueline Junco, Irina R Rozenfeld, Violetta Renesca, Amanpreet K Cheema

TL;DR
This paper reviews the effects of nutritional supplements on fatigue symptoms in ME/CFS patients, finding some supplements may help but with limitations in study quality.
Contribution
A systematic review of clinical trials on nutraceuticals for ME/CFS, highlighting gaps in standardized outcome measures.
Findings
Supplements like NADH, CoQ10, wasabi, and probiotics showed potential symptom improvement in ME/CFS.
Many trials lacked standardized NIH/NINDS outcome measures, limiting comparability and generalization.
Nutritional interventions are commonly used but evidence remains scarce and inconsistent.
Abstract
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a debilitating condition marked by severe, long-lasting fatigue and exhaustion that does not improve with rest. ME/CFS is reported in individuals of all ages and various racial, socioeconomic, and ethnic groups. This condition lacks standard treatment. Nutritional supplements and dietary interventions are often used to manage symptoms, but the efficacy of these interventions remains scarce in the current literature. This systematic review aims to evaluate and summarize recent evidence on nutrient supplementation and diet-based interventions in patients with ME/CFS sourced from clinical trial registries and article databases. Registries improve the quality, integrity, and transparency of clinical trials by providing a standardized platform for reporting study design and results and, thus, reducing the biases related to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
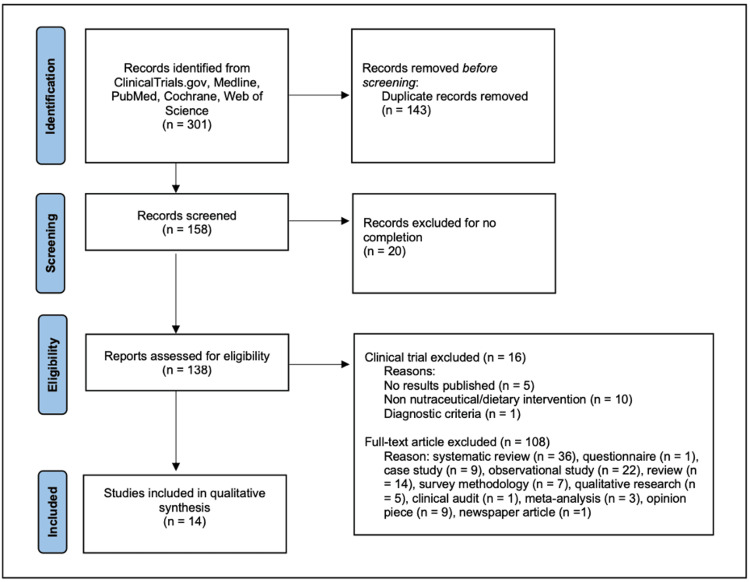 Figure 1
Figure 1| References | Year | Country | Study design | Treatment intervention | Treatment duration (weeks) | Reported side effects | Final number of participants | Age (years) mean (SD) | Sex, female % | |||
| Control | Tx | Control | Tx | Control | Tx | |||||||
| Barletta et al. [ | 2023 | Italy | RCT | CoQ10 + alpha-lipoic acid | 8 | No reported adverse effects | 58 | 116 | 50.3 | 51.7 | 51.1 | 48.9 |
| Cash and Kaufman [ | 2022 | USA | OPT, POC | Anhydrous enol-oxaloacetate (AEO) | 6 | Dyspepsia 2/23 500 mg BID, 2/24 1,000 mg BID and insomnia 1/26 500 mg BID | N/A | 76 | N/A | 47 | N/A | 77.6 |
| Castro-Marrero et al. [ | 2016 | Spain | RCT, POC | CoQ10 + NADH | 8 | No reported adverse effects | 34 | 39 | 49.1 (8.4) | 49.3 (7.1) | 100 | 100 |
| Castro-Marrero et al. [ | 2021 | Spain | RCT, POC | CoQ10 + NADH | 12 | Epigastralgia, dizziness | 72 | 72 | 46.8 (6.5) | 45.4 (7.8) | 100 | 100 |
| Castro-Marrero et al. [ | 2021 | Spain | RCT, POC | Melatonin + zinc | 16 | No reported adverse effects | 24 | 26 | 53.7 (9.6) | 51.0 (10.2) | 100 | 100 |
| Castro-Marrero et al. [ | 2022 | Spain | OPT | CoQ10 + selenium | 8 | No reported adverse effects | N/A | 27 | N/A | 47.3 (1.5) | N/A | 100 |
| Comhaire [ | 2018 | Belgium | OPT, POC | Sodium DCA | 4 | Generalized moderate tremor in one pt, which disappeared immediately after decreased DCA dose | N/A | 22 | N/A | 43.3 | N/A | 63.3 |
| Friedberg and Choi [ | 2022 | USA | RCT | Hydrogen water | 4 | Headache, heartburn, loose stools, pain, and brain fog | 11 | 11 | 53.6 (7.3) | 40.3 (10.7) | 81.8 | 75 |
| Kan et al. [ | 2021 | China | RCT |
| 8 | No reported adverse effects | 58 | 117 (59 high dose; 58 low dose) | 50.7 (7.6) | 50.5 (7.0) high dose; 51.5 (7.5) low dose | 50 | 52.5% high dose, 53.4% low dose |
| Ostojic et al. [ | 2016 | Serbia | RCT, CO | Guanidinoacetic acid | 12 | No reported adverse effects | N/A | 14 | N/A | 39.3 (8.8) | N/A | 100 |
| Oka et al. [ | 2022 | Japan | OPT | 6-Methylsulfinylhexyl isothiocyanate | 12 | No reported adverse effects | N/A | 15 | N/A | 37.5 | N/A | 80 |
| Teitelbaum et al. [ | 2012 | USA | OPT | D-Ribose | 3 | Nausea, insomnia | N/A | 203 | N/A | 51 | N/A | 91.6 |
| Teitelbaum et al. [ | 2020 | USA | OPT | Porcine serum polypeptide | 5 | Mild gas and bloating, loose stool, nausea, fatigue, insomnia, feeling irritable and fidgety | N/A | 43 | N/A | 58 | N/A | 83.7 |
| Venturini et al. [ | 2019 | Italy | OPT | Probiotics* | 8 | Symptom flare-up in one patient, although inflammatory markers did not increase | N/A | 9 | N/A | NR | N/A | NR |
| Reference (date) | Treatment intervention | Primary/secondary outcome measures | Results |
| Barletta et al. (2022) [ | CoQ10 + alpha-lipoic acid | FSS | Significantly lower (p < 0.0001) |
| SSS | Significantly lower (p < 0.0001) | ||
| VAS for pain, sleep, and fatigue | Significantly lower for pain, sleep, and fatigue (p < 0.0001) | ||
| WPI | Significantly lower (p < 0.0001) | ||
| FAS | Significantly lower (p < 0.0001) | ||
| Cash and Kaufman (2022) [ | Anhydrous enol-oxaloacetate (AEO) | CFQ-11 | Physical fatigue: significantly lower for 500 mg BID (p < 0.005), 1,000 mg BID (p < 0.005), and 1,000 mg TID (p < 0.01) |
| Castro-Marrero et al. (2016) [ | CoQ10 + NADH | Max HR | Significantly lower (p = 0.022) |
| FIS-40 | Fatigue: significantly lower (p = 0.03) | ||
| MPQ | Pain: NS | ||
| PSQI | Sleep: NS | ||
| Castro-Marrero et al. (2021) [ | CoQ10 + NADH | FIS-40 | Fatigue: significantly lower (p < 0.001) |
| SF-36 | HRQoL: significantly higher (p < 0.05) | ||
| Sleep duration: significantly higher (p = 0.018) | |||
| Habitual sleep efficiency: significantly higher (p = 0.038) | |||
| Castro-Marrero et al. (2021) [ | Melatonin + zinc | FIS-40 | Fatigue: significantly lower (p < 0.05) |
| SF-36 | Sleep: NS | ||
| HADS | Anxiety: NS | ||
| Urinary melatonin metabolite | Significantly higher (p < 0.0001) | ||
| Castro-Marrero et al. (2022) [ | CoQ10 + selenium | FIS-40 | Fatigue: significantly lower (p = 0.021) |
| SF-36 | HRQoL: significantly higher (p = 0.002) | ||
| PSQI | Sleep: NS | ||
| TAC | Significantly higher (p < 0.0001) | ||
| Lipid peroxidase | Significantly lower (p < 0.0001) | ||
| Inflammatory cytokines | NS | ||
| Comhaire (2018) [ | Sodium dichloroacetate | FSS | Fatigue: significantly lower (p = 0.0001) |
| Friedberg and Choi (2022) [ | Hydrogen water | FSS | Fatigue: significantly lower (p = 0.04) |
| SF-36 | Sleep: NS | ||
| DASS-21 | NS | ||
| Kan et al. (2021) [ |
| CFQ-11 | Fatigue: significantly lower (p = 0.001) |
| WHOQoL | HRQoL: significantly higher (p < 0.01) | ||
| SLQQ | Sexual life quality: significantly higher (p < 0.01) | ||
| Blood ammonia | Significantly lower (p < 0.05 low dose; p < 0.01) | ||
| Lactic acid | Significantly lower (p < 0.05 low dose; p < 0.01) | ||
| Ostojic et al. (2016) [ | Guanidinoacetic acid | MFI | Fatigue: NS |
| VAS for pain | Pain: NS | ||
| Muscular creatine levels | Significantly higher (p < 0.01) | ||
| Muscular strength and aerobic power | Significantly higher (p < 0.05) | ||
| Oka et al. (2022) [ | 6-Methylsulfinylhexyl isothiocyanate | PS | Significantly higher (p = 0.015) |
| CFQ-11 | Physical and mental fatigue (CFQ-11): NS | ||
| PSQI | Sleep: NS | ||
| PPT | Pain: significantly lower for headache frequency (p = 0.001) & myalgia (p = 0.019) | ||
| TMT-A | TMT-A time: significantly lower (p = 0.007) | ||
| Right occipital PPT: significantly higher (p = 0.01) | |||
| NRS | NRS scores: significantly lower for brain fog (p = 0.011), difficulty finding words (p = 0.015), photophobia (p = 0.008) | ||
| Orthostatic intolerance | Orthostatic intolerance: NS | ||
| POMS2 | Significantly higher for vigor (p = 0.045) | ||
| HADS | NS for anxiety & depression | ||
| SF-36 | HRQoL: significantly higher for general health perception (p = 0.036) & vitality (p = 0.039) | ||
| Teitelbaum et al. (2012) [ | D-Ribose | 7-point hedonic scale for fatigue symptoms | Fatigue symptoms: significantly lower (p < 0.0001) |
| Teitelbaum et al. (2020) [ | Porcine serum polypeptide | VAS for fatigue symptoms & pain | Significantly lower for fatigue symptoms (p < 0.001) & pain (p < 0.013) |
| FIQR | Significantly lower (p < 0.001) | ||
| Antibody levels | Significantly higher for IgGa (p = 0.008) & IgG1a (p < 0.001) | ||
| Venturini et al. (2019) [ | Probiotics* | UC | 2.3x fold increase |
| DHEA-S concentration | 1.4x fold increase | ||
| CAL | 2.5-1x fold increase | ||
| CRP concentration | 30% reduction | ||
| SF-36 & CFQ-11 | SF-36 & CFQ-11 combination: significant improvement of mental component (p = 0.043) | ||
| BDI-I & BDI-II | NS |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibromyalgia and Chronic Fatigue Syndrome Research · Biochemical effects in animals · Exercise and Physiological Responses
Introduction and background
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a profoundly debilitating disease characterized by long-lasting fatigue and exhaustion that does not improve with rest. Currently, about 17-24 million people suffer from ME/CFS, with women having a two times greater risk of being affected than men [1].
The disease can be difficult to diagnose, as it often relies on the exclusion of other acute and chronic pathologies due to the condition’s varied symptomatology. Besides chronic fatigue, patients commonly experience sleep abnormalities, cardiovascular complications, endocrine imbalance, respiratory issues, cognitive dysfunction, pain, and post-exertional malaise (PEM), defined as a worsening of symptoms after physical and/or mental exertion [2,3]. Many ME/CFS patients are housebound or even bedridden for long periods of time, severely impacting their quality of life (QoL) [3]. The complex, multisymptom nature of ME/CFS, coupled with a lack of understanding of its pathophysiology, has hindered the development of clear treatments. The incidence of ME/CFS has been attributed to infectious illness, exposure to environmental toxins, viral infections, and stress [4]. However, no specific etiology has been determined [5]. Preclinical and human mechanistic studies have suggested dysfunctions in multiple organ systems influencing the myriad symptoms experienced by patients [4,5]. Biomarker, metabolomics, and genomic studies have highlighted abnormal functioning of various biochemical processes involving the metabolism of key nutrients [3,6-8].
Mitochondrial dysfunction is a recurring feature seen in ME/CFS that contributes to impaired energy production and symptoms of fatigue and PEM [9-11]. Nutraceuticals such as coenzyme Q10 (CoQ10) have been studied for their potential to improve mitochondrial dysfunction. In addition, oxidative and nitrosative stress pathways are implicated in the pathophysiology of ME/CFS, with increased levels of inflammatory cytokines exacerbating cellular damage. Several nutraceuticals have been studied to mitigate these inflammatory and oxidative stress effects [12]. Disruption of the gut mucosal barrier and subsequent bacterial translocation may further amplify immune and oxidative stress. Interventions such as probiotics and glutamine have been shown to restore gut integrity and reduce inflammation [9,13]. Moreover, integrative medicine approaches have demonstrated potential in ameliorating the debilitating physical and cognitive symptoms of ME/CFS [3,8,14-16]. Given the central role of mitochondrial and oxidative dysfunction in ME/CFS, nutraceuticals represent a promising therapeutic avenue. However, no systematic evaluation of nutrition/nutraceutical-focused registered studies in ME/CFS has yet been conducted.
This paper evaluates and discusses the most recent evidence regarding nutrient supplementation and diet-based interventions for patients with ME/CFS, using literature databases including Medline, PubMed, Cochrane, and Web of Science and, most importantly, clinical registries such as ClinicalTrials.gov. ClinicalTrials.gov, a registry of clinical trials run by the United States National Library of Medicine at the National Institutes of Health (NIH), provides information on the effectiveness of treatments while avoiding the information biases often linked with systematic reviews.
This article was previously presented as a meeting abstract at the 2023 Undergraduate Student Symposium (USS) at Nova Southeastern University Alvin Sherman Library, Research, and Information Technology Center.
Review
Methods
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [17]. A systematic search was conducted to locate interventional studies with patients with ME/CFS. Studies that were included targeted nutrient supplementation and diet-based interventions.
The search process included the following steps: (i) A systematic search was conducted across ClinicalTrials.gov, Medline, PubMed, Cochrane, and Web of Science. The search was restricted to publication dates between 2010 and 2023. (ii) To identify relevant clinical trials pertaining to ME/CFS, ClinicalTrials.gov was searched with the “All Studies” status selected to include both completed and ongoing trials. The terms “ME/CFS”, “Chronic Fatigue Syndrome”, or “Myalgic Encephalomyelitis” for disease or condition were used. (iii) To limit the studies for interventions focused on nutritional supplementation or diet modification, the disease or condition was searched with the combination of the words “Nutrition”, “Nutraceutical”, and “Diet”. (iv) Medline, PubMed, Cochrane, and Web of Science were searched with advanced search builder showing (("benign myalgic encephalomyelitis" OR "chronic fatigue" OR "chronic fatigue and immune dysfunction syndrome" OR "encephalomyelitis, myalgic" OR "fatigue syndrome" OR "fatigue syndrome, chronic" OR "myalgic encephalomyelitis" OR "syndrome of chronic fatigue" OR "syndrome, chronic fatigue" OR "systemic exertion intolerance disease" OR "chronic fatigue syndrome") AND ("nutraceuticals" OR "nutriceutical" OR "nutriceuticals" OR "nutraceutical" OR "supplementation")). We screened full-text articles written in English and conducted on humans.
Eligibility Criteria
Studies were selected if they contained at least one nutraceutical or dietary intervention search term and at least one ME/CFS search term. They also had to satisfy the following inclusion criteria: (i) interventional studies published after 2010, (ii) study conducted on human participants aged 18 years or older, (iii) full text available in English, (iv) reporting of original research only, (v) diagnosis of ME/CFS follows Centers for Disease Control and Prevention (CDC) diagnosis criteria, and (vi) studies use nutraceuticals and/or diet intervention to target ME/CFS symptoms. Excluded studies included observational studies, narrative reviews, studies with multimodal interventions, and case reports, as well as studies not focused on ME/CFS as a primary diagnosis and studies including participants under 18 years of age or with comorbid conditions that confound ME/CFS symptomatology. Unpublished and ongoing clinical trials were also excluded.
Data Extraction
Relevant data were extracted from each of the studies. This includes the (i) study design, (ii) treatment intervention, (iii) treatment duration, (iv) country, (vi) number of participants, (vii) participants’ age, (viii) participants’ sex, (ix) adverse effects, (x) primary outcomes, and (xi) secondary outcomes.
Quality and Certainty Assessment
Quality and bias were assessed using the Delphi list for randomized controlled trials (RCTs). The Delphi list has been extensively evaluated and validated [18]. The Quality Assessment for Diverse Studies (QuADS) tool was used to assess open-label non-randomized studies. The QuADS tool is a modification of the QATSDD tool, which has shown substantial reliability for use in systematic review papers with multimethod health service research [19]. EMB, LB, and RP individually conducted the assessment, and no studies were excluded based on the results.
Results
A total of 301 studies were retrieved from ClinicalTrials.gov, Medline, PubMed, Cochrane, and Web of Science. Duplicate studies were removed, yielding a total of 158 studies worldwide. Incomplete studies were removed, including three with unknown status, four withdrawn, eight recruiting, three actives but not recruiting, and two not recruiting yet, leaving 138 articles to be assessed for eligibility. Among the studies, 30 were completed clinical trials, of which five had no results published, 10 were not a supplemental or dietary intervention for ME/CFS, and one did not follow the ME/CFS diagnostic criteria by the CDC. Data from the 14 remaining studies were included in the systematic review. This selection process followed PRISMA guidelines summarized in Figure 1 [17]. Article screening was conducted independently by EMB and RJ, with a third reviewer, LB, breaking ties. Each individual reviewer reviewed all articles blindly.
PRISMA flow diagram for study selectionPRISMA criteria described in reference [17].PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study Overview and Characteristics
The overview and characteristics of studies included in this review are presented in Table 1. A meta-analysis was not conducted due to substantial heterogeneity in study design, nutraceutical interventions, outcome measures, and follow-up durations. The included studies varied widely in the type, dosage, and duration of nutraceutical or dietary interventions, as well as in how outcomes were assessed, using different self-reported scales. All included studies were intervention-based. Following article selection, they were further classified based on study type. Seven were RCTs [20-26], three of which were proof-of-concept (POC) studies [21-23]. RCTs are designed to rigorously evaluate efficacy through random assignment to treatment arms, while POC studies are preliminary investigations assessing feasibility, biological activity, or early signals of efficacy. Among the RCTs, one followed a cross-over (CO) design [26], while the remaining five used a parallel design. In the CO design, participants received both the intervention and the control treatment in sequential periods, serving as their own controls and potentially reducing variability. In contrast, in a parallel design, each participant is assigned to only one treatment arm for the entire study duration. Seven of the studies were open-labelled pilot trials (OPTs) [27-33], two of which were also POC studies [30,31]. OPTs are exploratory studies without blinding, primarily assessing feasibility, safety, or preliminary outcomes. Fatigue was the primary outcome in 12 out of 14 studies [20,22-32]. Fatigue was measured using various self-reported questionnaires, including the Fatigue Impact Scale (FIS-40), the Chalder Fatigue Scale (CFQ-11), the Multidimensional Fatigue Inventory (MFI), a seven-point hedonic scale, the Visual Analog Scale (VAS), and the Fatigue Severity Scale (FSS) [20-33].
Participant Characteristics
There was a total of 1,046 participants across the 14 studies analyzed in this systematic review who completed their respective clinical interventions. Initially enrolled patients who failed to complete their studies were excluded due to failure to satisfy inclusion criteria, declining to participate, stopping the intervention due to adverse side effects, requesting to leave, or failing to follow up. The proportion of males to females was 19.6% versus 80.4%, respectively. All participants were above 18 years of age, with the average age being 48.4 years.
Interventions on Primary Outcomes
Fatigue was the primary outcome in all studies except two [21,23]. Of the studies that assessed fatigue as the primary outcome, 10 out of 12 reported significant improvements in fatigue levels post-treatment [20,22-31]. While these findings suggest a potential therapeutic benefit, the clinical significance is more difficult to determine due to variability in the fatigue measurement tools used, which included the FIS-40 and FSS. For instance, one study using a combination of CoQ10 and nicotinamide adenine dinucleotide (NADH) demonstrated significantly lower FIS-40 scores [22], and another study using CoQ10 with alpha-lipoic acid also showed decreased fatigue levels on the FSS [20]. Both interventions yielded changes that may be clinically meaningful; however, the lack of standardization in fatigue assessment tools limits the ability to directly compare effect sizes or determine uniform clinical relevance across studies. Treatment with melatonin and zinc supplementation in another study also reported significantly lower FIS-40 scores [23]. CoQ10 plus selenium supplementation was shown to significantly decrease fatigue levels post-intervention [27]. Another study supplementing with hydrogen water found a small but significant difference in perceptive fatigue symptoms using the FSS [24]. A combination treatment of Ginkgo and Cistanche showed significantly lower levels of perceptive fatigue in both of its treatment groups, with improvement in fatigue being proportional to the treatment dosage [25]. Another open-label trial using anhydrous enol-oxaloacetate (AEO) also decreased patients’ levels of fatigue in its three subgroups, using different dosages and intake frequencies [30]. Treatment with sodium dichloroacetate (DCA) also resulted in significantly lower fatigue levels [31]. Two studies reported no significant difference in fatigue levels after intervention [26,32]. Although treatment with wasabi showed no significant improvements in fatigue levels, it did result in improvements in performance status [32]. In one study, patients receiving D-ribose reported significant improvements in energy, sleep, mental clarity, and overall well-being [28]. Treatment with porcine peptide serum in another study also resulted in significant improvements in energy, well-being, sleep, cognition, anxiety, gastrointestinal health, and pain [29].
One study’s primary endpoint was to assess the efficiency of supplementing with CoQ10 and NADH on maximum heart rate (HR) during a cycle ergometer test [21]. The study reported that participants in the active group had a significant reduction in maximum HR [21]. Another study’s outcome was to assess the safety and efficacy of supplementing with probiotics in ME/CFS patients, reporting significant improvements in mental fatigue levels as well as a decrease in inflammatory cytokines post-treatment [33]. While these findings suggest promise for several interventions, the variability in outcome measures limits the ability to compare effect sizes or determine generalizable clinical efficacy across studies.
Interventions on Secondary Outcomes
Several secondary endpoints were assessed in the studies, including physical function, psychological outcomes, biochemical markers, and QoL domains (Table 2). In the domain of physical function, supplementation with guanidinoacetic acid (GAA) significantly increased muscular creatine levels, muscular strength, and aerobic power, though no significant changes in pain were observed [26]. Treatment with porcine serum polypeptide resulted in a significant reduction in Revised Fibromyalgia Impact Questionnaire (FIQR) scores, indicating improved functional status [29].
Regarding psychological and clinical outcomes, CoQ10 and alpha-lipoic acid supplementation improved sleep and pain, as well as scores on the widespread pain index (WPI) and the modified fibromyalgia assessment status [20]. Of the two studies using CoQ10 and NADH, one reported improved fatigue with no change in pain or sleep, while the other reported significant improvement in sleep and health-related QoL (HRQoL) [21,22]. Melatonin and zinc supplementation led to increased melatonin metabolite excretion but did not improve sleep or anxiety, and hydrogen water treatment showed no significant changes in secondary outcomes [23,24]. Wasabi (6-methylsulfinylhexyl isothiocyanate (6-MSITC)) improved self-reported vigor and reduced symptoms such as brain fog, photophobia, and word-finding difficulty [32].
Biochemical outcomes were assessed in several trials. CoQ10 and selenium supplementation increased total antioxidant capacity (TAC) and reduced lipid peroxidase levels, although it had no impact on inflammatory cytokines [27]. Probiotic supplementation resulted in biomarker changes including increased urinary free cortisol (UC), fecal calprotectin (CAL), and dehydroepiandrosterone sulfate (DHEA-S) and decreased C-reactive protein (CRP) [33].
In terms of QoL, Ginkgo and Cistanche significantly improved both general health-related and sexual QoL, along with reductions in blood ammonia and lactic acid levels [25]. Wasabi supplementation was also associated with improved vitality-related HRQoL, and CoQ10 with selenium increased HRQoL even in the absence of changes to sleep quality [27,32]. The D-ribose study did not report any secondary endpoints [28].
Quality Assessment
Quality assessment scores for each study can be found in Supplemental materials 1 and 2. Six of the studies in this review were determined to be of high quality based on the Delphi list (Delphi score > 7) [21-26] while only one study assessed using the QuADS criteria met the threshold for good quality (QuADS score = 32) [27]. Lower-quality studies commonly failed to implement randomization and blinding of participants and assessors, which are key methodological steps that help reduce selection and measurement bias. Item nine of the Delphi list, which assesses the intention-to-treat (ITT) statement, was the least addressed item among the RTCs included in this review. The absence of ITT analysis may overestimate treatment effects by excluding non-compliant participants. For the OPTs, items six and 10 from the QuADS criteria were the least addressed. These items assessed the rationale behind the data collection tools used and the justification for the analytic method selected, respectively. The absence of clear theoretical justification for these aspects reduces both the interpretability and reproducibility of study findings. These methodological gaps are important to consider when evaluating the reliability and validity of reported outcomes. Trials that lack blinding are more prone to expectation biases, and those without robust analytical rationale may yield spurious or non-generalizable associations. Future research in this area would benefit from the routine use of ITT protocols and the adoption of validated, theory-driven outcome measures to enhance methodological rigor and cross-study comparability.
Discussion
ME/CFS is a debilitating medical condition with no established standard of care [5]. Consequently, many patients resort to either clinician- or self-recommended dietary and nutritional supplements to alleviate symptoms [1,5]. This retrospective systematic review reviewed data from 14 trials reporting improvements in self-reported or administered measures of disease severity and other symptoms of illness.
The heterogeneity of the instruments used in these studies presents a challenge, however, to conduct a comparison of the effectiveness of treatments. The U.S. NIH’s National Institute of Neurological Disorders and Stroke (NINDS) collaborated with the CDC in 2018 to identify and define common data elements (CDEs) for ME/CFS to reduce this prevalent issue in translational research [34,35]. However, none of the studies included in this review employed the recommended CDEs, which limits comparability across trials and contributes to inconsistency in reported outcomes. This methodological shortcoming compromises the ability to synthesize evidence and draw generalizable conclusions. In addition, clinical trial registries, such as the National Library of Medicine ClinicalTrials.gov registry, provide valuable information on the effectiveness of the treatments while avoiding information biases often associated with systematic reviews. Although the requirements for registering studies are designed to standardize the information within a study record including the type of study, intervention, trial phase, funding source, outcomes, and data types to be reported, the Food and Drug Administration Amendments Act (FDAAA 801) mandates the registration of only studies that meet the definition of an "applicable clinical trial" (ACT) onto ClinicalTrials.gov [36,37]. None of the studies included in this review reported their results on ClinicalTrials.gov or have utilized the core instruments recommended by the CDEs. The absence of trial registration introduces risks of publication bias, selective outcome reporting, and overestimated effect sizes, which can weaken the transparency and reproducibility of findings. This study retrieved applicable results from separate journals and databases, including PubMed, Cochrane, Medline, and Web of Science, to complete this review. Not only is this process of scientific evaluation cumbersome, but it is also impractical for a patient population with a significant disease burden to make an informed decision.
This review highlights the already reported sex differences in ME/CFS affliction, with 80.4% of the aggregated study population being female, potentially attributed to underlying neuroendocrine adaptations. However, only three studies reported race or ethnicity, and all participants in those studies identified as Caucasian [22,23,27]. This lack of diversity restricts the generalizability of findings and overlooks possible race or ethnicity-specific manifestations of ME/CFS. Moreover, many of the studies included in this review were conducted outside of the United States and originated from a single institution, underscoring the need for more diverse studies to confirm replicability and ensure population representation. Studies across multiple therapeutic areas have recognized this general lack of racial/ethnic diversity in research studies, potentially due to identified fiscal and sociopsychological barriers faced by underserved communities. The lack of representation hinders the profiling of the crucial phenotypic traits of illnesses that may be race/ethnicity-specific, leading to worse public health outcomes in these communities.
All participants in this review were diagnosed with ME/CFS using the CDC diagnostic criteria from 1994 and the 2015 National Academy of Medicine criteria [38]. More specific diagnostic criteria such as the Canadian Consensus Criteria (CCC) and International Consensus Criteria (ICC) should be considered in future research to minimize diagnostic overlap with other conditions [2,39]. Furthermore, several studies failed to implement key methodological practices such as blinding of participants and assessors or the use of ITT analysis. These flaws may introduce bias, reduce internal validity, and compromise the reliability of treatment effects observed in unblinded or non-randomized trials.
Despite these limitations, the studies discussed represent the core body of available evidence on this topic across databases such as ClinicalTrials.gov, PubMed, Medline, Cochrane, and Web of Science. The focus of this review was studies utilizing supplements/nutrients/diet as the sole intervention, although it is worth noting that one trial explored the effects of a mitochondria-support nutrient formula coadministered with a low-dose stimulant [40,41]. This combination had synergistic effects, optimizing cellular energy production and alertness while improving tolerability and reducing reliance on stimulants. However, this was not representative of the broader evidence base reviewed and falls outside the review’s inclusion criteria. Therefore, recommendations regarding combination therapy with supplements and medications remain speculative and should be interpreted with caution, requiring the need for future studies.
Finally, further investigations employing the CDEs for ME/CFS are needed not only to standardize measured outcomes but also to enhance reproducibility, reduce bias, and enable direct comparison across trials. Incorporating CDEs, such as uniform fatigue scales, cognitive testing protocols, and biological markers, could provide more structured and interpretable data. High-quality, rigorously designed RCTs with transparent reporting and diverse populations are essential to strengthen the evidence on the role of nutraceuticals in ME/CFS and guide future clinical recommendations.
Conclusions
This review identified current studies showing that supplementation with CoQ10, NADH, selenium, melatonin, AEO, alpha-lipoic acid, DCA, and zinc may be beneficial in improving subjective fatigue symptoms in patients with ME/CFS. Additionally, supplements such as Ginkgo, Cistanche, wasabi, and probiotics have the potential to alleviate symptoms related to cognitive and memory impairment, while GAA may positively affect muscular strength. CoQ10, selenium, and probiotics have also demonstrated anti-inflammatory effects. While these findings are encouraging, they must be interpreted with caution, given the considerable methodological limitations present in many of the included studies. The frequent absence of blinding, lack of ITT analysis, limited racial/ethnic representation, and heterogeneity in outcome measures significantly compromise internal validity and generalizability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): where will the drugs come from?Pharmacol Res Toogood PL Clauw DJ Phadke S Hoffman D 10546516520213352975010.1016/j.phrs.2021.105465 · doi ↗ · pubmed ↗
- 2Myalgic encephalomyelitis/chronic fatigue syndrome J Chronic Fatigue Syndr Carruthers BM Jain AK De Meirleir KL 7115112003
- 3The chronic fatigue syndrome: a comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group Ann Intern Med Fukuda K Straus SE Hickie I Sharpe MC Dobbins JG Komaroff A 9539591211994797872210.7326/0003-4819-121-12-199412150-00009 · doi ↗ · pubmed ↗
- 4Long COVID and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS)-a systemic review and comparison of clinical presentation and symptomatology Medicina (Kaunas) Wong TL Weitzer DJ 4185720213392578410.3390/medicina 57050418 PMC 8145228 · doi ↗ · pubmed ↗
- 5Myalgic encephalomyelitis/chronic fatigue syndrome: a comprehensive review Diagnostics (Basel) Cortes Rivera M Mastronardi C Silva-Aldana CT Arcos-Burgos M Lidbury BA 91920193139472510.3390/diagnostics 9030091 PMC 6787585 · doi ↗ · pubmed ↗
- 6Metabolic features of chronic fatigue syndrome Proc Natl Acad Sci U S A Naviaux RK Naviaux JC Li K 080113201610.1073/pnas.1607571113 PMC 502746427573827 · doi ↗ · pubmed ↗
- 7Insights into myalgic encephalomyelitis/chronic fatigue syndrome phenotypes through comprehensive metabolomics Sci Rep Nagy-Szakal D Barupal DK Lee B 10056820182996880510.1038/s 41598-018-28477-9PMC 6030047 · doi ↗ · pubmed ↗
- 8Comprehensive circulatory metabolomics in ME/CFS reveals disrupted metabolism of acyl lipids and steroids Metabolites Germain A Barupal DK Levine SM Hanson MR 341020203194754510.3390/metabo 10010034 PMC 7023305 · doi ↗ · pubmed ↗