Migration of atrial septal occluder device to the thoracic aorta: case report
Felipe Carrasco Ferreira Dionisio, Pedro Henrique Amaral Ângelo da Silva, Bruno Lima Moreira, Augusto Kreling Medeiros, Felipe Carrasco Ferreira Dionisio, Pedro Henrique Amaral Ângelo da Silva, Bruno Lima Moreira, Augusto Kreling Medeiros

TL;DR
A rare case of a heart defect closure device migrating to the aorta is reported, highlighting the need for careful management and imaging in such complications.
Contribution
This paper presents a rare clinical case of Amplatzer™ device migration and emphasizes the importance of imaging in managing late complications.
Findings
Device migration occurred 6 months after implantation in an asymptomatic patient.
The case was managed with percutaneous removal followed by open surgery.
Imaging played a crucial role in determining the treatment plan.
Abstract
Atrial septal defect (ASD) is a common cardiac defect with significant implications if left untreated. Although open heart surgery is the traditional approach, transcatheter closure devices, such as the Amplatzer™ Septal Occluder Device, have gained prominence due to advantages like shorter hospital stays and reduced costs. Among potential complications, device migration is a rare complication, with an incidence of 0.5 to 1.1%. We report a rare case of migration of an Amplatzer™ device in an asymptomatic patient, diagnosed 6 months after its implantation. After detecting the issue, the medical team opted for percutaneous device removal followed by open surgery to correct the ASD. In conclusion, managing Amplatzer™ device embolization requires careful consideration of the patient’s circumstances and device anatomy. This case highlights the importance of correlating clinical and imaging…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
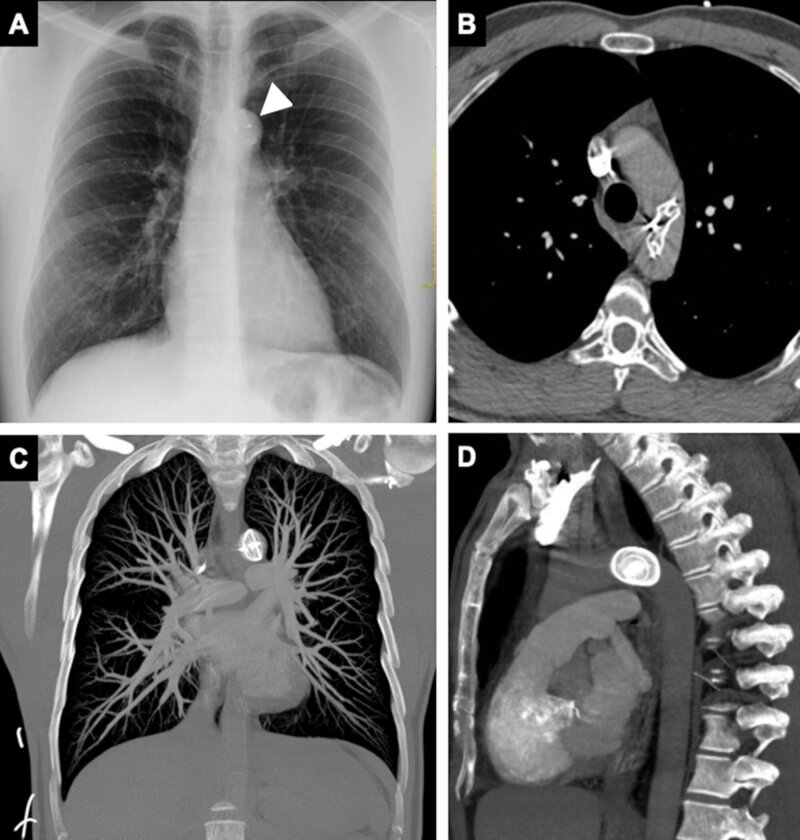 Figure 1
Figure 1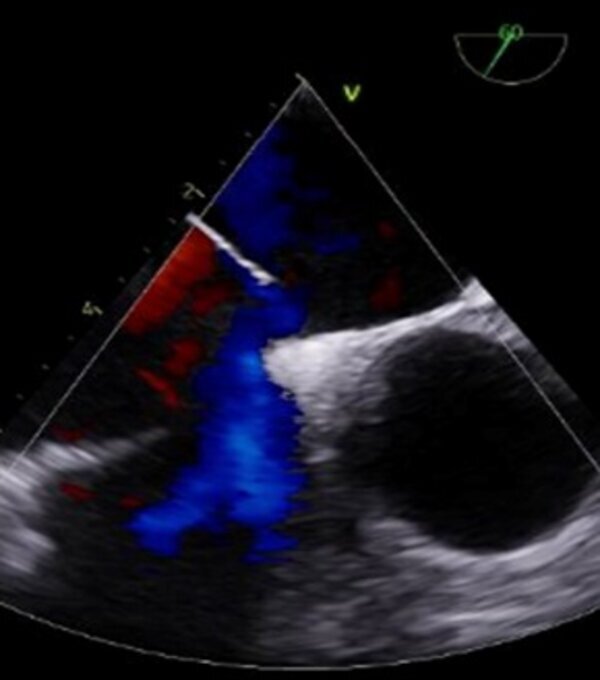 Figure 2
Figure 2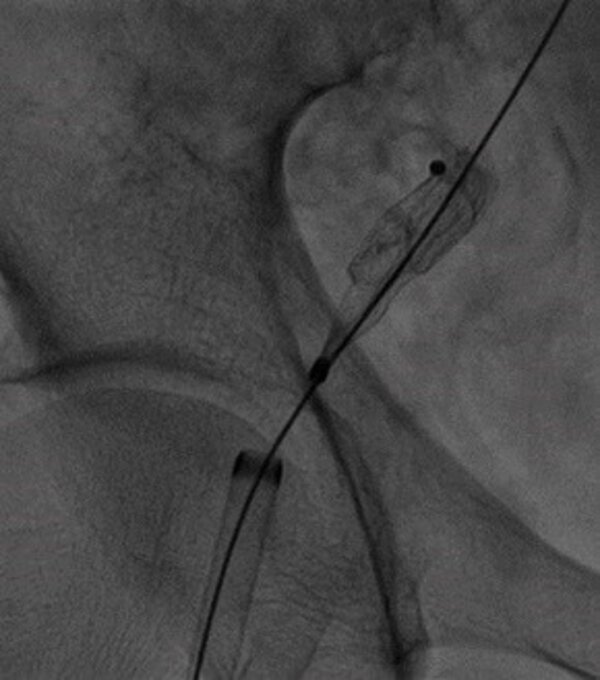 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Airway Management and Intubation Techniques · Congenital Heart Disease Studies
INTRODUCTION
Atrial septal defect (ASD) is one of the most common congenital cardiac defects. Some cases are identified early in childhood, while others remain undetected until adulthood, becoming hemodynamically significant over time. If left uncorrected, they can cause right ventricular overload, leading to heart failure, increased pulmonary vascular resistance, emboli, and atrial arrhythmia.^1,2^
While open surgery is a well-established method for repairing septal defects, improvements in devices for transcatheter closure have made this technique increasingly common. Studies suggest that these devices offer comparable efficacy to open surgery, with shorter hospital stays and reduced costs.^3^
In this context, Amplatzer™ septal occluder devices are widely used for minimally invasive closure. However, they are not entirely free from complications, among which migration is a rare event, with incidence ranging from 0.5 to 1.1% of cases.^4^
In this article, we report a rare case of migration of an Amplatzer™ device to the proximal thoracic descending aorta that was detected in the sixth month following implantation during a routine Doppler ultrasonography in an asymptomatic patient. This case report illustrates a rare complication during the postoperative period after placement of an atrial septal occlusion device and discusses the corresponding imaging findings and the treatment options available.
The protocol was approved by the Ethics Committee at our institution (CAAE – 75966923.4.0000.5483 and decision number 6.614.692).
CASE DESCRIPTION
An asymptomatic 42-year-old man presented at our service with a referral letter recommended urgent admission having undergone an echocardiogram at an external provider for 6-month follow-up of percutaneous placement of an Amplatzer™ cardiac device to correct an ostium secundum ASD. It had not been possible to locate the device in its expected topography during the examination, suggesting the possibility of migration/embolization. The patient’s reports suggested that the examinations performed immediately postoperatively and for control at 3 months after the procedure had been normal.
During the physical examination at admission, the patient was free from acute discomfort, blood pressure was 173 / 80 mmHg, there was no fever or signs of cyanosis (oxygen saturation of 96% in room air), heart rate and rhythm were normal, and there was no evidence of heart murmur.
He was admitted to hospital by the cardiology team. A chest X-ray revealed dense material with a circular shape in the region of the proximal descending thoracic aorta, compatible with the cardiac device fitted previously (Figure 1A). No devices were identified in the cardiac projection.
(A) Chest X-ray (front view) showing the anomalous position of the septal occluder device in the proximal descending thoracic aorta projection (arrowhead); (B-D) Computed tomography with iodinated contrast confirmed the position of the device in the proximal descending thoracic aorta and ruled out complications, such as pulmonary thromboembolism or aortic thrombosis.
A subsequent angiotomography confirmed the Amplatzer™ device in an anomalous position in the proximal descending thoracic aorta and helped to rule out other complications, such as thromboembolism or formation of thrombi adjacent to the device (Figure 1B-D). Once the device had been precisely located, the patient underwent transesophageal Doppler ultrasonography, which showed that the interatrial communication with left-right shunt was still present (Figure 2). After analysis of the images and discussion of the case, the interventional cardiology team decided to attempt percutaneous removal of the device, via the right iliofemoral arterial axis (Figure 3) after puncture of the right femoral artery by the Seldinger technique. Aortography was used to locate the prosthesis and a 12F radiopaque sheath was inserted, followed by a snare catheter, which was advanced up to the proximal descending thoracic aorta, with capture and displacement of the migrated device. The device was found anchored in the femoral artery, requiring a longitudinal incision in this artery to enable removal of the device under direct visualization. After removal of the device, angiotomography was performed again, with no further significant findings, ruling out potential complications related to embolization of the Amplatzer™ device, such as thrombi or other vascular injuries (lesions). Approximately 2 weeks later, the patient underwent atrial septoplasty via a median sternotomy, with closure of the ASD using bovine pericardium, with no postoperative complications.
Transesophageal echocardiogram revealed persistence of an ostium secundum interatrial communication with a diameter of 7.5 mm, causing left-right shunt.
Fluoroscopic image of percutaneous removal of the device via the right iliofemoral arterial axis.
DISCUSSION
Modern cardiac devices have both temporary and permanent applications and are used to treat a range of cardiac conditions. These devices include those for ASD occlusion.^1,5^ Several different studies have demonstrated that the percutaneous technique for ASD correction is as safe and effective as open surgery, with similar results. Advantages of percutaneous occlusion include no need for extracorporeal circulation, reduced postoperative discomfort, and shorter hospital stay.^3^
In 1997, Kurt Amplatz developed a self-expandable device made from nitinol wires (a nickel and titanium alloy) comprising two circular discs connected by a short central waist. This device became known as the Amplatzer™ septal occluder and was approved by the Food and Drug Administration (FDA) in 2001.^6^
In addition to its use for closure of ASDs, the Amplatzer™ device is also used to treat other types of heart defects, such as patent foramen ovale and ventricular septal defect. A range of different models and sizes are available, enabling choice of the most appropriate device tailored to each patient, considering the size and location of the defect.
The overall rate of complications after the percutaneous ASD closure procedure varies from 6.1% to 11.1%. The most common complications are embolization and malpositioning.^2^
A device that becomes displaced can migrate to several different areas, including the following: main pulmonary artery, left ventricle, left atrium, thoracic ascending aorta, aortic arch, or thoracic descending aorta. In the majority of cases, the device migrates to the main pulmonary artery, as shown by a study by Chessa et al.,^7^ in which migration to this artery occurred in 89% of cases analyzed.^7^ Migration is most often detected during the first 24 hours after the procedure, underscoring the importance of conducting Doppler ultrasonography immediately or during the first few hours after fitting the device.^2,8^ In this scenario, Doppler ultrasonography plays a crucial role after placement of an Amplatzer™ device, enabling determination of its exact position and detection of residual shunts. In contrast, cases of embolization to the aortic arch or to the thoracic descending aorta in the late postoperative period are extremely rare.^2^ In specific situations, primarily later cases, computed tomography is a valuable tool for evaluating devices, especially in relation to embolizations. It enables the precise location of the Amplatzer™ and its anatomic relationships to be determined, making it essential for management and choice of removal technique. Moreover, computed tomography facilitates assessment of device migration or protrusion into anatomic structures that might not be visualized with confidence using transthoracic echocardiogram.
With regard to management of cases of Amplatzer™ device embolization, studies indicate that percutaneous removal is a well-established option when embolization occurs soon after fitting the device. However, in late embolization cases, in which there is a high probability of endothelization of the prosthesis, removal by open surgery may be safer, because of the increased risk of injury to the vascular wall.^4^ Taking into account the risk-benefit balance in asymptomatic patients, conservative management may be considered (observation, without immediate removal of the device).^4,8^ In our case, the patient was asymptomatic and, after analysis of the images, ruling out complications adjacent to the device, such as formation of thrombi or endothelization, the medical team chose percutaneous removal of the device, using the right femoral artery.
In summary, management of Amplatzer™ device embolization must consider several factors, including the time of migration, the probability of endothelization, the clinical condition of the patient, and the anatomy of the device. Assessment with different imaging methods and their correlation plays a fundamental role in choice of the best management approach. In our case, correlation of clinical findings with the imaging exams was crucial, since it enabled us to start with the less invasive treatment, with intraoperative confirmation that the migrated device was free from vascular adhesion and percutaneous removal of the device via the right iliofemoral arterial axis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brida M Chessa M Celermajer D et al Atrial septal defect in adulthood: a new paradigm for congenital heart disease Eur Heart J 202243282660267110.1093/eurheartj/ehab 64634535989 · doi ↗ · pubmed ↗
- 2Kim HH Yi GJ Song SW Late migration of amplatzer septal occluder device to the descending thoracic aorta Korean J Thorac Cardiovasc Surg 2017501474910.5090/kjtcs.2017.50.1.4728180104 PMC 5295484 · doi ↗ · pubmed ↗
- 3Ooi YK Kelleman M Ehrlich A et al Transcatheter versus surgical closure of atrial septal defects in children: a value comparison JACC Cardiovasc Interv 201691798610.1016/j.jcin.2015.09.02826762915 · doi ↗ · pubmed ↗
- 4Silvestre JMS Silvestre GS Sardinha WE et al Complicação após tratamento percutâneo de comunicação interatrial: migração de dispositivo Amplatzer® para bifurcação aórtica: relato de caso J Vasc Bras 201514327127410.1590/1677-5449-0010 · doi ↗
- 5Moore J Hegde S El-Said H et al Transcatheter device closure of atrial septal defects: a safety review JACC Cardiovasc Interv 20136543344210.1016/j.jcin.2013.02.00523702008 · doi ↗ · pubmed ↗
- 6Shrivastava S Shrivastava S Allu SVV Schmidt P Transcatheter closure of atrial septal defect: a review of currently used devices Cureus 2023156 e 4013210.7759/cureus.4013237425612 PMC 10329454 · doi ↗ · pubmed ↗
- 7Chessa M Carminati M Butera G et al Early and late complications associated with transcatheter occlusion of secundum atrial septal defect J Am Coll Cardiol 20023961061106510.1016/S 0735-1097(02)01711-411897451 · doi ↗ · pubmed ↗
- 8Maleux G Rega F Heye S Troost E Budts W Asymptomatic migration of a first-generation AMPLATZER vascular plug into the abdominal aorta: conservative management may be an option J Vasc Interv Radiol 201122456957010.1016/j.jvir.2010.11.03321316986 · doi ↗ · pubmed ↗