Self‐Care Interventions for Preventing Cardiovascular Diseases After Hypertensive Pregnancy Disorders: A Systematic Review and Meta‐Analysis
Thuy D. T. Mai, Sho Katsuragawa, Annie McDougall, Phi‐Yen Nguyen, Lorena Romero, Joshua Vogel, Maureen Makama

TL;DR
This study reviews whether self-care practices can help prevent heart disease in women who had high blood pressure during pregnancy.
Contribution
The paper provides a systematic review and meta-analysis of self-care interventions for preventing cardiovascular diseases in women with a history of hypertensive pregnancy disorders.
Findings
Self-care interventions may reduce systolic and diastolic blood pressure in women with previous hypertensive disorders of pregnancy.
Self-care interventions likely decrease the risk of postpartum hypertension readmission.
There is insufficient evidence to support the effectiveness of self-care interventions in preventing cardiovascular events and chronic hypertension.
Abstract
Women with previous hypertensive disorders of pregnancy (HDP) have an increased risk of developing cardiovascular diseases (CVDs) later in life. Self‐care interventions are known to promote health and well‐being, such as self‐measured blood pressure or mindfulness interventions. We evaluated whether self‐care interventions reduced the incidence of cardiovascular events, chronic hypertension, and the risk of CVDs in women with previous HDP. MEDLINE, Embase, CINAHL, PsycINFO, and the Cochrane Library were systematically searched on 08 January 2025 without date or language restrictions. Randomised and non‐randomised controlled trials. Meta‐analysis was performed using random‐effects models. We included 16 studies involving 2200 women. Fourteen studies from twelve randomised trials, one was a non‐randomised trial, and one was a quasi‐experimental study. Data from nine trials involving…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
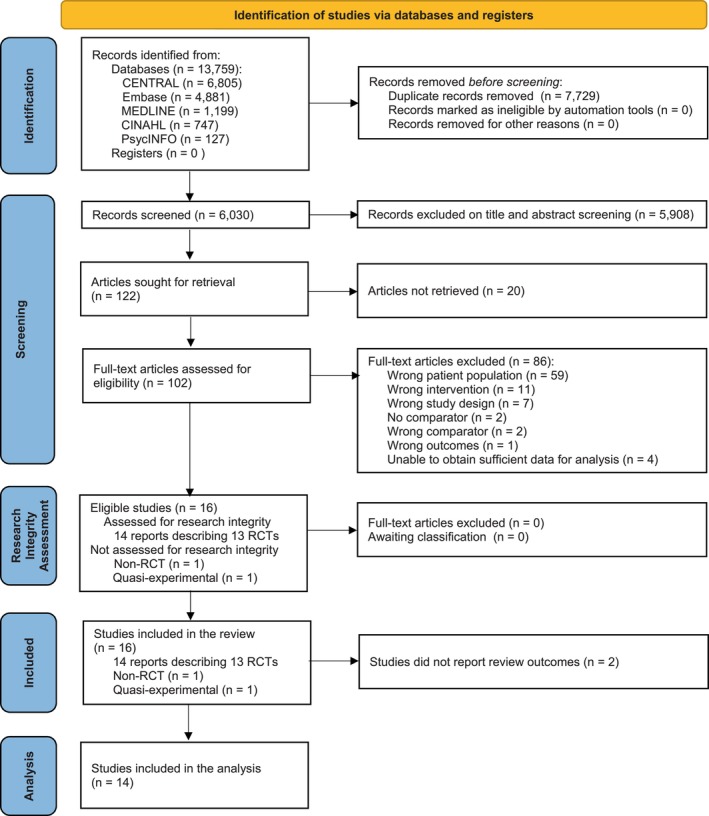 FIGURE 1
FIGURE 1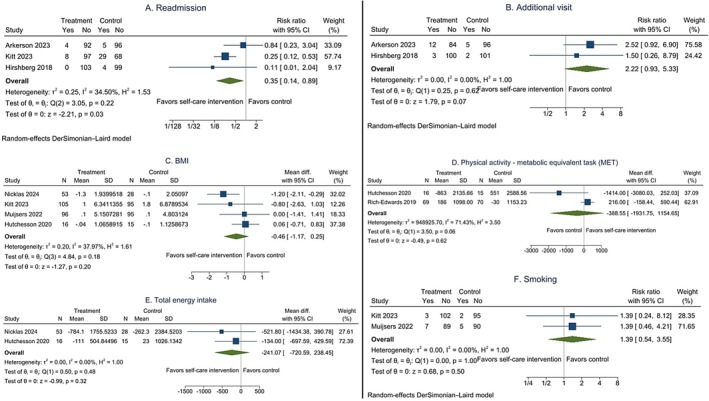 FIGURE 2
FIGURE 2| Author Year | Study design | Country | Intervention vs. Control | Postpartum period at enrolment | Intervention duration | Sample size | Review outcomes |
|---|---|---|---|---|---|---|---|
| Arkerson 2023 | RCT | USA | HBPM vs. IBPM | Soon after discharge | 16 days | 197 | Additional visits, medication |
| Cairns 2018 | RCT | England | HBPM vs. Usual care | Soon after discharge | 6 months | 82 | BP, medication, Psychological status |
| Ekawati 2019 | Non‐RCT | Indonesia | Lifestyle change vs. Not specified | On the 2nd day | 7 days | 60 | No outcomes of interest |
| Hauspurg 2023 | RCT | USA | HBPM vs. HBPM+ Lifestyle change vs. Usual care | 6 weeks to 6 months | 12 months | 129 | BP, BMI, medication, Hypertension, PA, Retention, Self‐efficacy |
| Hirshberg 2018 | RCT | USA | HBPM vs. IBPM | 4 to 6 days | 2 weeks | 206 | Additional visits, medication |
| Hoppe 2020 | Non‐RCT | USA | HBPM vs. Standard care | Soon after discharge | 6 weeks | 428 | Additional visits, medication |
| Hutchesson 2020 | RCT | Australia | Lifestyle change vs. Usual care | Within 4 years | 3 months | 31 | BP, BMI, Dietary intake, Lipid levels, PA, Psychological status |
| Kitt 2021 | RCT | England | HBPM vs. Usual care | Soon after discharge | 6 months | 61 | BP |
| Kitt 2023 | RCT | England | HBPM vs. Standard care | 1 to 6 days | 9 months | 200 | BP, BMI, medication, Readmission, PA, Smoking, Breastfeeding |
| Lewey 2022 | RCT | USA | PA vs. No intervention | 1 to 4 months | 3 months | 127 | BP, PA |
| Muijsers 2022 | RCT | Netherlands, Germany | HBPM vs. Usual care | At least 1 year | 12 months | 191 | BP, BMI, medication, Chest pain, Diabetes, Hypertension, Smoking |
| Nicklas 2024 | RCT | USA | Lifestyle change vs. Usual care | 1 to 3 months | 6 weeks | 58 | BP, BMI, Dietary intake, Lipid levels, PA, Psychological status |
| Parfenova 2021 | RCT | Canada | Lifestyle change vs. Usual care | 1 to 18 months | 1 month | 98 | No outcomes of interest |
| Rich‐Edwards 2019 | RCT | USA | Lifestyle change vs. Usual care | Within 5 years | 9 months | 139 | PA, Self‐efficacy |
| Riemer 2021 | RCT | Germany | Lifestyle change vs. Usual care | 6 weeks | 6 months | 29 | BP |
| Wang 2024 | RCT | USA | Neonatal sleep vs. Usual care | 6 weeks | 4 months | 104 | BP, medication, Hypertension |
| Outcomes | № of participants (studies) | Certainty of the evidence (GRADE) | Relative effect (95% CI) | Anticipated absolute effects with no intervention, usual or standard care | |
|---|---|---|---|---|---|
| Risk | Risk difference | ||||
| Postpartum hypertension readmission assessed with: Incidence follow‐up: range 2 weeks to 9 months |
605 (3 RCTs) |
⨁⨁⨁◯ Moderate |
RR 0.35 (0.14 to 0.89) | 126 per 1000 |
82 fewer per 1000 (109 fewer to 14 fewer) |
| Additional emergency department or office visit for hypertension not resulting in readmission assessed with: Incidence follow‐up: mean 15 days |
403 (2 RCTs) |
⨁⨁◯◯ Low |
RR 2.22 (0.93 to 5.33) | 34 per 1000 |
42 more per 1000 (2 fewer to 149 more) |
| Use of anti‐hypertensive medications assessed with: Incidence follow‐up: range 2 weeks to 12 months |
1063 (7 RCTs) |
⨁◯◯◯ Very low |
RR 1.20 (0.82 to 1.75) | 79 per 1000 |
16 more per 1000 (14 fewer to 59 more) |
| Systolic blood pressure (SBP) assessed with: mmHg follow‐up: range 3 months to 12 months |
952 (9 RCTs) |
⨁⨁◯◯ Low | — | — |
MD 3.24 mmHg lower (5.42 lower to 1.06 lower) |
| Diastolic blood pressure (DBP) assessed with: mmHg follow‐up: range 3 months to 12 months |
952 (9 RCTs) |
⨁⨁◯◯ Low | — | — |
MD 3.07 mmHg lower (4.88 lower to 1.25 lower) |
| Body mass index (BMI) assessed with: kg/m2 follow‐up: range 3 months to 12 months |
503 (4 RCTs) |
⨁◯◯◯ Very low | — | — |
MD 0.46 kg/m2 lower (1.17 lower to 0.25 higher) |
| Smoking assessed with: Incidence follow‐up: range 9 months to 12 months |
393 (2 RCTs) |
⨁◯◯◯ Very low |
RR 1.39 (0.54 to 3.55) | 36 per 1000 |
14 more per 1000 (17 fewer to 93 more) |
| Physical activity assessed with: MET mins/week follow‐up: range 3 months to 9 months |
175 (2 RCTs) |
⨁◯◯◯ Very low | — | — |
MD 388.55 MET mins/week lower (1931.75 lower to 1154.65 higher) |
| Total energy intake assessed with: Kcal/day |
112 (2 RCTs) |
⨁◯◯◯ Very low | — | — |
MD 241.07 Kcal/day lower (720.59 lower to 238.45 higher) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPregnancy and preeclampsia studies · Cardiovascular Issues in Pregnancy · Birth, Development, and Health
Introduction
1
Hypertensive disorders of pregnancy (HDP) refer to a group of conditions, including chronic (preexisting) hypertension, preeclampsia/eclampsia, and gestational hypertension [1]. Globally HDP affects 18.1 million women yearly [2], and its burden is greatest in low‐ and middle‐income countries (LMICs), accounting for 95% of HDP maternal deaths worldwide [3]. Women who experienced HDP are at a two‐to four‐fold higher risk of developing cardiovascular diseases (CVDs) in later life, including hypertension (relative risk (RR) 3.46; 95% confidence interval (CI) 2.67, 4.49) or heart failure (RR 2.53; 95% CI 1.28, 5.00) [4]. These elevated risks may persist for at least a decade [5, 6, 7], and even after they have developed, CVDs can be a silent or asymptomatic condition for many years [8, 9, 10]. CVDs encompass heart and blood vessel disorders, such as coronary heart disease, rheumatic heart disease, and deep vein thrombosis [11]. CVDs are among the leading causes of death globally, at least 75% of which occur in LMICs, accounting for 9.2 million female deaths in 2019 [12, 13, 14].
Women with a history of HDP may benefit from interventions aimed at reducing CVD risk factors. In recent years, the World Health Organisation (WHO) has promoted self‐care interventions as a promising approach to enhance people's health and well‐being [15]. Self‐care interventions can include tools to support and actions to improve individuals' ability to care for themselves [16]. Self‐care interventions encompass various approaches, including health literacy, regular physical activity, understanding and practices to mitigate risks, awareness and taking action against dangers [17].
For chronic disease prevention and management, self‐care interventions usually relate to behavioural change, equipping people with the knowledge and skills needed to be responsible and actively self‐maintain, self‐monitor, and self‐manage their illness [18]. One commonly proposed mechanism suggests that self‐care actions have a cardioprotective effect, such as minimising inflammation or avoiding risky pharmacological treatment [19], serving as complementary interventions alongside primary treatments for underlying conditions. For example, maintaining a high‐fibre diet helps improve cholesterol levels and endothelial function to decrease inflammation, a risk factor for CVDs [20, 21].
Early prevention strategies with self‐care actions, including practices, lifestyle choices, and habits, might be effective in mitigating the risk of developing CVDs in women with previous HDP. Although there are existing reviews on different interventions to reduce CVD risks in this population, such as lifestyle interventions or home blood pressure (BP) monitoring [22, 23, 24, 25, 26], no reviews have specifically evaluated all components of self‐care interventions together. Furthermore, evidence is absent on the effectiveness of recommended self‐care interventions for women with a history of HDP [27]; it is crucial to identify whether self‐care interventions are effective in preventing CVD risks and outcomes for this high‐risk population. This study aimed to systematically evaluate the evidence on the effects of self‐care interventions on the incidence of cardiovascular events chronic hypertension and risk factors of CVDs in women with a history of HDP.
Methods
2
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines (Appendix S1) [28]. The protocol was prospectively registered with PROSPERO (CRD42023473686) (Appendix S9).
Eligibility Criteria
2.1
Primary randomised and non‐randomised trials (including cross‐over trials, cluster randomised and quasi‐experimental trials) administering self‐care interventions to women with a history of HDP were eligible. There were no limits based on duration since the last pregnancy. To ensure a homogeneous study population and better isolate the impact of self‐care interventions, studies including women with preexisting CVDs (such as stroke, renal failure, or cardiac disease) before the index pregnancy were excluded. Caregivers (family members or partners) carrying out self‐care for women with HDP were excluded. We defined a self‐care intervention as any non‐pharmacological strategy, tool, or resource designed to encourage or support self‐care. The intervention could be single or combined with other self‐care interventions to increase the coverage and quality of healthcare services and/or enhance well‐being, health, and care experiences. Eligible comparisons were no intervention, usual or standard care. Trials were not eligible if their primary interest was in another population, such as gestational diabetes or high BMI, even though they reported on women with previous HDP. There were no restrictions on the language or date of publication.
Information Sources and Search Strategy
2.2
Studies were retrieved from MEDLINE, Embase, CINAHL, PsycINFO, and the Cochrane Library on 09 November 2023, and updated on 08 January 2025 using a pre‐defined search strategy developed in consultation with an information specialist (LR) (Appendix S2). Each electronic database was searched using adapted free text and index terms for the two main concepts: (a) hypertensive disorders of pregnancy and (b) self‐care interventions. Additionally, we manually reviewed the reference lists of included studies to identify any other relevant studies.
Study Selection and Research Integrity Assessment
2.3
Citations were collated using EndNote X9 [29], and screening was conducted using Covidence [30]. After removing duplicates, two reviewers (TM and SK) independently assessed the titles and abstracts, followed by the full text of the remaining citations to determine eligibility. Any disagreements were resolved through discussion and consultation with a third reviewer (MM or AM). Google Translate was used for articles published in languages other than English.
We contacted authors as required to obtain further information for (a) research integrity assessment (RIA), (b) data extraction and analysis, such as missing values needed for meta‐analysis, and (c) clarification of data. Studies for which authors did not respond after two attempts to contact them via email to obtain sufficient data for analysis were recorded as no response. All eligible studies underwent RIA using a published RIA tool [31] by two independent reviewers (TM and SK).
Data Extraction and Quality Assessment
2.4
Two reviewers (TM and SK) independently extracted data from eligible studies using Covidence [30]. Details extracted included study characteristics, design, sample size, duration of study enrolment, participant characteristics, duration and type of self‐care intervention, and the primary and secondary outcomes reported. Review outcomes were selected based on the recommended core outcome set of CVD [32, 33, 34] and commonly used outcomes from reviews on interventions for people with HDP [22, 25, 26]. The primary outcomes were (1) the incidence of any cardiovascular, event (such as stroke, myocardial infarction, or heart failure) and (2) chronic hypertension. Risk factors and additional secondary outcomes are BMI, diabetes, BP, lipid levels, physical activity, dietary intake, breastfeeding, psychological issues, smoking, caffeine use, alcohol use, illicit drug use status, social harms autonomy, and antihypertensive medication requirement (Appendix S3). Studies were not excluded based on review outcomes. We extracted all studies' characteristics, including those that did not report review outcomes. Any discrepancies were resolved through discussion.
The quality of identified randomised controlled trials (RCTs) was assessed using the revised Cochrane risk‐of‐bias tool for randomised trials (RoB 2) [35], and for non‐randomised trials (non‐RCTs), the risk‐of‐bias in non‐randomised studies of interventions (ROBINS‐I) tool [36]. Two reviewers independently assessed each study (TM and SK), and any disagreements were resolved by a third reviewer (MM or AM). Risk‐of‐bias plots were presented using Robvis [37]. Two reviewers (TM and SK) independently assessed the certainty of evidence using Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) [38] in GRADEpro [39]. Disagreements were resolved through discussion or consultation with a third reviewer (MM or AM).
Data Synthesis
2.5
Studies' characteristics were reported descriptively. Data analysis was carried out using STATA SE 18 [40]. For outcomes reported by at least 2 studies, a meta‐analysis was conducted [41]. Results from non‐RCTs were not included in a meta‐analysis. Findings from non‐RCTs and outcomes reported by < 2 trials are presented narratively. Statistical heterogeneity was assessed with a random‐effects model due to the potential sources of variations in intervention effects and sampling error across trials [41]. Heterogeneity was considered substantial if I^2^ > 50% [41]. Meta‐analyses were presented as RR (for binomial variables) or mean difference (MD) from baseline (for continuous variables), their 95% CI, and I^2^ values. Publication bias assessment via funnel plots or statistical tests was not completed as no outcomes were reported by 10 or more studies [38]. Descriptions of dealing with missing data, the unit of analysis issues, sensitivity analyses, sub‐group analyses, investigation of heterogeneity, and post hoc analyses are detailed in Appendix S4.
Results
3
Study Selection
3.1
The search identified 13 759 records. After removing duplicates, 6030 unique records were eligible for title and abstract screening. Of the 122 articles sought for full‐text retrieval, 102 studies were available in full text, with 20 unable to be sourced. There were 16 studies included in this review (14 studies describing 13 RCTs [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55], one non‐RCT [56], and one quasi‐experimental study [57]). Two studies did not report review outcomes, leaving 14 included in the analysis (Figure 1 and Appendix S5). No studies were excluded from the analysis based on RIA (Appendix S6).
PRISMA flow chart of included studies. The research integrity tool was designed to assess RCTs only; therefore, non‐RCTs did not undergo research integrity assessment.
Study Characteristics
3.2
The review included 16 studies involving 2200 participants and reporting self‐care interventions for women with previous HDP [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 56, 57]. One study [53] was a secondary analysis of another trial [50]. All studies were published between 2018 and 2024 and were conducted in eight countries – the United States (n = 8) [44, 45, 48, 49, 51, 52, 55, 56], England (n = 3) [50, 53, 54], Australia (n = 1) [43], Canada (n = 1) [47], and Germany (n = 1) [46], the Netherlands and Germany (n = 1) [42], and a lower‐middle‐income country Indonesia (n = 1) (Table 1) [57].
The components of self‐care interventions included home‐based BP monitoring (n = 8) [42, 48, 49, 50, 51, 53, 54, 56]; lifestyle change (n = 6) [43, 46, 47, 52, 55, 57]; physical exercise (n = 1) [45]; neonatal sleep (n = 1) [44]. Control groups received usual care (n = 10) [42, 43, 44, 46, 47, 49, 50, 52, 53, 55]; standard care (n = 2), in‐office BP (n = 2) [48, 51], no intervention (n = 1) [45], and not specified (n = 1) [57]. The time of enrolment into the study ranged from post‐delivery to 5 years postpartum. Most studies implemented self‐care interventions during the first 6a months postpartum (n = 12) [44, 45, 46, 47, 48, 49, 50, 51, 53, 55, 56, 57]. The most commonly reported outcomes were systolic and diastolic BP (n = 10) [42, 44, 45, 46, 49, 50, 53, 54, 55, 58] and the use of antihypertensives (n = 7) (Table 1) [42, 44, 48, 49, 50, 51, 54]. Descriptions of self‐care intervention in each study arm, the number of participants at baseline, and attrition are detailed in Appendix S6.
Risk of Bias of Included Studies
3.3
Twelve studies from eleven RCTs had a high risk of bias primarily due to missing outcome data [43, 44, 46, 47, 49, 50, 51, 52, 53, 55], and bias in the measurement of the outcome [47, 48, 51, 52]. One RCT had some concerns [45], and one RCT had a low risk of bias (Appendix S7, Figure S1) [54]. One non‐RCT had a critical risk of bias primarily due to the risk of confounding [57], and the other had a serious risk of bias due to confounding and outcome measurements (Appendix S7, Figure S2) [56].
Synthesis of Results
3.4
Results from twelve studies reported eleven RCTs [42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55] were included in the meta‐analyses. One study had two intervention arms; hence, the data were combined and considered as a single intervention arm [49]. Seven studies did not report the SDs for change in outcome measures [42, 44, 45, 46, 50, 52, 54], and were calculated from the reported baseline and final SD values.
Primary Outcomes – Cardiovascular Events and Chronic Hypertension
3.5
Chest Pain
3.5.1
One trial involving 198 women found no association between self‐care interventions and the risk of chest pain (RR 0.67; 95% CI 0.30, 1.48; p = 0.31) [42].
Stage 1 or Greater Hypertension or on Antihypertensive Medications (130/80 mmHg or Higher)
3.5.2
One trial involving 76 women reported no association between self‐care interventions and the incidence of the composite outcome stage 1 or greater hypertension or antihypertensive medications (RR 0.76, 95% CI 0.50, 1.16) [44]. Similarly, another trial involving 129 women reported no association (RR 1.26, 95% CI 0.91, 1.75) [49].
Stage 2 Hypertension and/or on Antihypertensive Medications (140/90 mmHg or Higher)
3.5.3
One trial involving 129 women reported no association between self‐care interventions and the incidence of the composite outcome stage 2 hypertension and/or on antihypertensive medication (RR 1.20; 95% CI 0.58, 2.48; p = 0.61) [49].
Secondary Outcomes
3.6
Data from 9 trials involving 952 women showed that compared to women in the control group, women receiving self‐care interventions may have lower systolic (MD from baseline −3.24; 95% CI −5.42, −1.06 mmHg; low‐certainty evidence) and diastolic BP (MD from baseline −3.07; 95% CI −4.88, −1.25 mmHg; low‐certainty evidence) (Figure 2, Table 2). In the post hoc sensitivity analyses, the overall effect sizes from the leave‐one‐out meta‐analyses are consistent, indicating that self‐care interventions may have lowered systolic and diastolic BP (Figure S5).
The effects of self‐care interventions on the mean difference from baseline of systolic blood pressure (A) and diastolic blood pressure (B), and the subgroup analysis by duration for systolic blood pressure (C) and diastolic blood pressure (D).
The effect of self‐care interventions on the risk of using antihypertensive medications is uncertain (RR 1.20; 95% CI 0.82, 1.75; 7 trials; 1063 women; very low‐certainty evidence) (Figure S3, Table 2). A non‐RCT reported no association between self‐care interventions and the risk of using anti‐hypertensive medications (adjusted RR 1.03; 95% CI 0.74, 1.44; p = 0.87) [56].
Self‐care interventions likely decrease the risk of postpartum hypertension readmission (RR 0.35; 95% CI 0.14, 0.89; 3 trials; 605 women; moderate‐certainty evidence) (Figure S4, Table 2). One non‐RCT (428 women) found that self‐care interventions reduced the risk of postpartum hypertension readmission (adjusted RR 0.12; 95% CI 0.01, 0.96; p = 0.045) and did not reduce the risk of hypertension‐related emergency or triage room visits (adjusted RR 0.81, 95% CI 0.36, 1.80; p = 0.81) [56].
Self‐care interventions may make no difference to the risk of additional emergency department or office visits for hypertension not resulting in readmission (RR 2.22; 95% CI 0.93, 5.33; 2 trials, 403 women; low‐certainty evidence) (Figure S4, Table 2).
We are uncertain whether self‐care interventions were associated with a decrease in body mass index (MD −0.46; 95% CI −1.17, 0.25 kg/m^2^; 4 trials; 503 women; very low‐certainty evidence), an increase in physical activity—the metabolic equivalent task (MET) (MD −528.67; 95% CI −502.53, 1559.87 MET mins/week; 2 trials; 170 women; very low‐certainty evidence), a decrease in total energy intake (MD −241.07; 95% CI −720.59, 238.45 Kcal/day; 2 trials; 112 women; very low‐certainty evidence), and a reduction in the risk of smoking (RR 1.39; 95% CI 0.5, 3.55; 2 trials; 393 women; very low‐certainty evidence) (Figure S4, Table 2).
Sub‐Group Analysis by Duration
3.7
There was strong evidence for no sub‐group effect (p = 0.12) on systolic BP and (p = 0.21) on diastolic BP, indicating that intervention duration did not modify the self‐care intervention effects compared to no intervention, usual care, or standard care. Nonetheless, the number of trials and participants who contributed data to the sub‐group short‐term was less than to the sub‐group medium‐term (4 trials vs. 5 trials), suggesting that these meta‐analyses could not detect subgroup differences (Figure 2).
A narrative summary of other secondary outcomes and detailed information on sensitivity analyses are described in Appendix S8.
Discussion
4
Main Findings
4.1
This review is the first to evaluate the effectiveness of self‐care interventions for reducing CVD risks and CVD outcomes in women with a history of HDP. Few of the sixteen studies involving 2200 women that met our eligibility criteria reported the same outcomes. For primary outcomes, there were insufficient studies to pool results for cardiovascular events and chronic hypertension. For secondary outcomes, we are uncertain whether self‐care interventions were associated with a reduction in the risks of using anti‐hypertensive medications, smoking, a decrease in BMI and total energy intake, and an increase in physical activity due to very low certainty of evidence. Additionally, self‐care interventions may make no difference to the risk of additional emergency department or office visits for hypertension not resulting in readmission due to low certainty of evidence. However, some self‐care interventions likely decrease the risk of postpartum hypertension readmission (moderate‐certainty evidence) and appear to be associated with a decrease in BP (low‐certainty evidence) compared to no intervention, usual, or standard care. Sensitivity analyses that replaced correlation values in studies with missing SD for change and leave‐one‐out meta‐analyses showed similar results to the primary analyses. Subgroup analyses showed that intervention duration did not modify the effect of self‐care interventions on BP compared to no intervention, usual care, or standard care. While the findings suggest some promise, further high‐quality studies with multiple and longer follow‐up periods are needed, and agreed‐upon core outcomes are reported.
Strengths and Limitations
4.2
This review has several strengths. It is the first meta‐analysis to evaluate the effectiveness of self‐care interventions for reducing the risk of CVDs in women with previous HDP. We assessed all RCTs for integrity and only included studies conducted with appropriate ethical standards to ensure quality, ethics, and benefits to research and society. We also assessed the certainty of the evidence for all pooled results, which was not done in the existing meta‐analysis [26], providing stronger evidence for the practice and research implications of the findings of our review.
There are some limitations in our review. Firstly, there is unexplained heterogeneity across review outcomes; however, exploring these was limited because few studies reported the same outcomes. There were too few studies for subgroup analyses of primary outcomes. Subgroup analyses by the duration of intervention were conducted for secondary outcomes; however, there was insufficient data for meta‐analysis by type of HDP experienced during pregnancy, postpartum period at enrolment, by type of interventions, by single or combined interventions, by reproductive age, and by settings. This unexplained heterogeneity and the high risk of bias complicated the interpretation of the findings of our review [59]. Secondly, studies included in this review mostly did not report on cardiovascular events—our primary outcome and—did not research various research settings, restricting the generalisability of our review's findings. Thirdly, all RCTs except one trial included in the meta‐analysis were judged to be at high risk of bias, limiting the certainty of evidence of this review. However, masking and self‐reported measures are commonly unavoidable, given the nature of self‐care interventions.
Interpretation
4.3
Existing literature highlights the need for longer‐term follow‐up and management to prevent CVDs in women with previous HDP. A 2024 rapid review of two studies involving 589 women with previous HDP in the United States and Canada reported that text‐based BP monitoring and antihypertensive therapy interventions up to 10 days were not associated with a reduction in BP, hospital readmission for hypertension, and persistence of hypertension [60]. The absence of long‐term follow‐up was considered to contribute to the lack of association [60]. Similarly, a 2021 integrative review of 194 women with previous HDP from two studies in the Netherlands reported little or no association between physical activity interventions and CVD risk reduction [61]. According to the authors, the trial durations (4 and 12 weeks) might have been too short to detect any change [61]. Both reviews highlighted a gap in the current literature on longer‐term follow‐up. Additionally, there is a persistent risk of developing CVDs for decades after the first occurrence of HDP [5, 6, 7], however, most women with a history of HDP might still have a low chance of absolute risk in a CVD risk assessment in the first 10 years [62]. In our review, pooled results from 2 RCTs that followed up with their participants in 6 and 12 months showed no clear benefit of self‐care intervention for lowering the incidence of the composite outcome of stage 1 or greater hypertension or on antihypertensive medications.
The current clinical recommendations are based on limited evidence for women with a history of HDP. The International Federation of Gynaecology and Obstetrics recommended that women with a history of HDP should adopt lifestyle modifications, including appropriate exercise and a heart‐healthy diet, to reduce CVD risks [62, 63]. However, except for one case–control and one cohort study on women with a history of HDP [64, 65], the evidence supporting their recommendations was not specific to this population. For example, recommendations for using a heart‐healthy diet to reduce the 10‐year Framingham Risk Score and exercise to lower CVD risks were based on meta‐analyses of adult men and women [66, 67]. Additionally, a 2019 review of international guidelines reported a lack of consensus in recommendations for frequency and length of follow‐up and an absence of referenced evidence on whether recommended interventions were effective for this population [27]. This lack of evidence and emphasis on consistent and long‐term management recommendations might explain why only one trial in our review followed participants for up to four years [50, 53]. Besides, findings from our review showed low to very low certainty of evidence despite the included trials incorporating recommended self‐care interventions in women with previous HDP. Furthermore, there were insufficient studies to explore the effectiveness of the types, single or combined interventions, timing, and settings of self‐care interventions, suggesting a significant knowledge gap in the prevention of CVDs in this high‐risk population.
Further trials and utilisation of the core outcome set of CVDs are needed. The American Heart Association—AHA (2017) emphasises that self‐care should not be overlooked in the effort to minimise CVD risks and outcomes [68]. Self‐care interventions could focus on the proposed mechanism of the underlying association between HDP and CVD risks, such as reducing inflammation [19]. One potential intervention that has not been explored in included trials is breastfeeding, which can lower CVD risks, as reported in a 2022 meta‐analysis in parous women [69]. Breastfeeding interventions can be implemented immediately after delivery, and women are only required to adhere to breastfeeding for up to 12 months postpartum compared to a lifelong commitment to maintaining a healthy lifestyle. This intervention may be particularly beneficial because women with a history of HDP often stop breastfeeding earlier than those without (−6.26, 95% CI −10.00, −2.51 weeks) in the first year postpartum [70]. Another potential intervention is to use biomarkers such as the calcitonin gene‐related peptide and adrenomedullin as an element in self‐care interventions [71, 72]. These biomarkers can identify individuals at an increased risk for developing CVDs [72], offering an alternative to the need for a long‐term follow‐up intervention. Furthermore, while the core outcome set of CVDs has been identified [32, 33, 34], it was not utilised in many of the included studies in this review. Using the core outcome set could improve the pooling of review outcomes and potentially improve heterogeneity.
It is essential to implement appropriate strategies to assess the effectiveness of self‐care interventions in this population. Effective interventions are critical in LMICs, where the burden of HDPs is highest. The incidence of HDP is highest in Africa, with a rate of 335 per 100 000 reproductive‐aged women in 2019, followed by Southeast Asia, with 136.8 per 100 000 and the Middle East, 121.4 per 100000 [73]. Nonetheless, studies included in this review were primarily conducted in high‐income countries, indicating a need for trials in LMICs. According to the WHO, self‐care interventions can be effective in diverse settings [16], and they could become even more essential in places with limited access to healthcare due to unavailability, inaccessibility, poor quality, and discrimination. For women, regardless of their postpartum period, maintaining self‐care practices can be challenging due to the demands of motherhood, efficacy, financial limitations, and adherence to social and cultural practices [74, 75]. Hence, future research should tailor self‐care interventions to the challenges and preferences of women with a history of HDP. For instance, a qualitative study reported that postpartum women preferred flexible, low‐intensity lifestyle intervention programs integrated into existing routine healthcare services [76]. Integrating self‐care interventions into the healthcare continuum allows healthcare professionals to provide early, continuous screening and consultation about the increased CVD risks [77, 78, 79], especially when self‐care interventions for this population are needed for further evaluation. Furthermore, this approach enables researchers to systematically collect data on women with previous HDP over time due to a persistent risk of developing CVDs [5, 6, 7]. Therefore, it is necessary for policymakers and public health practitioners to provide appropriate strategies to assess the viability of self‐care interventions, especially in LMICs.
Conclusion
5
This review investigated the effectiveness of self‐care interventions for the prevention of CVDs in women with previous HDP. Due to limited data on review outcomes, varying degrees of heterogeneity, and low to very low certainty of evidence, there is currently insufficient evidence for a recommendation of self‐care interventions for reducing the incidences of cardiovascular events, chronic hypertension, and reducing risk factors of CVDs in women with a history of HDP; although there was evidence that some self‐care interventions may lower blood pressure and likely decrease the risk of postpartum hypertension readmission. Larger trials with multiple and longer‐term follow‐ups, utilising the core outcome set of CVDs, may lead to different conclusions.
Author Contributions
T.D.T.M., A.M. and M.M. are responsible for conceptualisation and methodology. T.D.T.M. and S.K. are responsible for formal analysis and data curation. A.M., J.V. and M.M. are responsible for supervision. P.‐Y.N. and L.R. are responsible for software. T.D.T.M. wrote the original draft of the manuscript. All authors were responsible for the review and editing of the manuscript.
Ethics Statement
Ethical approval was not required as the study analysed publicly available data.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. A. Magee , M. A. Brown , D. R. Hall , et al., “The 2021 International Society for the Study of Hypertension in Pregnancy Classification, Diagnosis & Management Recommendations for International Practice,” Pregnancy Hypertens 27 (2022): 148–169.35066406 10.1016/j.preghy.2021.09.008 · doi ↗ · pubmed ↗
- 2W. Wang , X. Xie , T. Yuan , et al., “Epidemiological Trends of Maternal Hypertensive Disorders of Pregnancy at the Global, Regional, and National Levels: A Population‐Based Study,” BMC Pregnancy and Childbirth 21, no. 1 (2021): 364.33964896 10.1186/s 12884-021-03809-2PMC 8106862 · doi ↗ · pubmed ↗
- 3L. Say , D. Chou , A. Gemmill , et al., “Global Causes of Maternal Death: A WHO Systematic Analysis,” Lancet Global Health 2, no. 6 (2014): e 323–e 333.25103301 10.1016/S 2214-109X(14)70227-X · doi ↗ · pubmed ↗
- 4J. Sukmanee and T. Liabsuetrakul , “Risk of Future Cardiovascular Diseases in Different Years Postpartum After Hypertensive Disorders of Pregnancy: A Systematic Review and Meta‐Analysis,” Medicine (Baltimore) 101, no. 30 (2022): e 29646.35905265 10.1097/MD.0000000000029646 PMC 9333537 · doi ↗ · pubmed ↗
- 5W. Ying , J. M. Catov , and P. Ouyang , “Hypertensive Disorders of Pregnancy and Future Maternal Cardiovascular Risk,” Journal of the American Heart Association 7, no. 17 (2018): e 009382.30371154 10.1161/JAHA.118.009382 PMC 6201430 · doi ↗ · pubmed ↗
- 6P. Wu , R. Haththotuwa , C. S. Kwok , et al., “Preeclampsia and Future Cardiovascular Health,” Circulation. Cardiovascular Quality and Outcomes 10, no. 2 (2017): e 003497, 10.1161/circoutcomes.116.003497.28228456 · doi ↗ · pubmed ↗
- 7L. Bellamy , J. P. Casas , A. D. Hingorani , and D. J. Williams , “Pre‐Eclampsia and Risk of Cardiovascular Disease and Cancer in Later Life: Systematic Review and Meta‐Analysis,” BMJ 335, no. 7627 (2007): 974.17975258 10.1136/bmj.39335.385301.BEPMC 2072042 · doi ↗ · pubmed ↗
- 8N. M. Breetveld , C. Ghossein‐Doha , S. M. J. van Kuijk , et al., “Prevalence of Asymptomatic Heart Failure in Formerly Pre‐Eclamptic Women: A Cohort Study,” Ultrasound in Obstetrics & Gynecology 49, no. 1 (2017): 134–142.27404208 10.1002/uog.16014 · doi ↗ · pubmed ↗