Bidirectional relationship between sleep problems and long COVID: a longitudinal analysis of data from the COVIDENCE UK study
Giulia Vivaldi, Mohammad Talaei, John Blaikley, Callum Jackson, Paul E Pfeffer, Seif O Shaheen, Adrian R Martineau

TL;DR
This study finds that poor sleep before SARS-CoV-2 infection increases the risk of long COVID, and sleep duration changes briefly after infection but returns to normal.
Contribution
The study uses longitudinal data to show a bidirectional relationship between sleep and long COVID, with novel insights into sleep variability's role.
Findings
Poor pre-infection sleep quality is linked to a higher risk of long COVID.
Sleep duration increases slightly in the first month after infection but returns to baseline.
Fluctuations in sleep duration last up to six months in those with long COVID.
Abstract
Studies into the bidirectional relationship between sleep and long COVID have been limited by retrospective pre-infection sleep data and infrequent post-infection follow-up. We therefore used prospectively collected monthly data to evaluate how pre-infection sleep characteristics affect risk of long COVID and to track changes in sleep duration during the year after SARS-CoV-2 infection. COVIDENCE UK is a prospective, population-based UK study of COVID-19 in adults. We included non-hospitalised participants with evidence of SARS-CoV-2 infection and used logistic regression to estimate adjusted ORs for the association between preinfection sleep characteristics and long COVID. We assessed post-infection sleep duration using multilevel mixed models. We collected sleep data from participants using a subset of questions from the Pittsburgh Sleep Quality Index. We defined long COVID as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
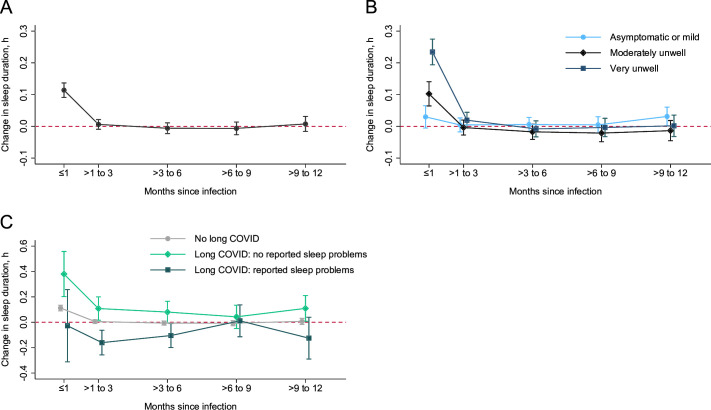 Figure 1
Figure 1| Reports long COVID (n=327) | Does not report long COVID (n=3667) | |
|---|---|---|
|
| ||
| Age, years | 59.0 (49.1–66.7) | 63.4 (55.4–69.3) |
| Sex | ||
| Female | 252 (77.1%) | 2592 (70.7%) |
| Male | 75 (22.9%) | 1075 (29.3%) |
| Ethnicity | ||
| White | 312 (95.4%) | 3541 (96.6%) |
| Black, African, Caribbean or Black British | 3 (0.9%) | 17 (0.5%) |
| South Asian | 4 (1.2%) | 47 (1.3%) |
| Mixed, multiple or other | 8 (2.4%) | 62 (1.7%) |
| IMD decile | 7 (5–9) | 7 (5–9) |
| Highest educational level attained | ||
| Primary or secondary | 48 (14.7%) | 331 (9.0%) |
| Higher or further (A levels) | 53 (16.2%) | 484 (13.2%) |
| College or university | 131 (40.1%) | 1658 (45.2%) |
| Post-graduate | 95 (29.1%) | 1194 (32.6%) |
| Weekly hours of vigorous physical exercise | ||
| 0 | 144 (44.0%) | 1111 (30.3%) |
| 1–3 | 121 (37.0%) | 1689 (46.1%) |
| ≥4 | 62 (19.0%) | 867 (23.6%) |
|
| ||
| Sleep duration, h | 6.7 (1.2) | 7.0 (1.0) |
| Sleep efficiency | 80% (74–88) | 84% (76–90) |
| Sleep quality | ||
| Good | 96 (29.4%) | 1453 (39.6%) |
| Medium | 133 (40.7%) | 1459 (39.8%) |
| Medium–low | 78 (23.9%) | 669 (18.2%) |
| Low | 20 (6.1%) | 86 (2.3%) |
| Medications | ||
| Benzodiazepines | 4 (1.2%) | 11 (0.3%) |
| Non-benzodiazepine hypnotics and sedatives | 6 (1.8%) | 39 (1.1%) |
|
| ||
| BMI, kg/m² | ||
| <25 | 126 (38.5%) | 2001 (54.6%) |
| 25 to <30 | 116 (35.5%) | 1129 (30.8%) |
| ≥30 | 85 (26.0%) | 537 (14.6%) |
| General health | ||
| Excellent | 48 (14.7%) | 1001 (27.3%) |
| Very good | 115 (35.2%) | 1662 (45.3%) |
| Good | 102 (31.2%) | 785 (21.4%) |
| Fair | 50 (15.3%) | 181 (4.9%) |
| Poor | 12 (3.7%) | 38 (1.0%) |
| Asthma or COPD | 69 (21.1%) | 516 (14.1%) |
| Autoimmune disease | 42 (12.8%) | 281 (7.7%) |
| Diabetes | ||
| Pre-diabetes | 13 (4.0%) | 101 (2.8%) |
| Diabetes | 23 (7.0%) | 141 (3.8%) |
| Heart disease | 15 (4.6%) | 101 (2.8%) |
| Hypertension | 72 (22.0%) | 755 (20.6%) |
| Immunosuppression or organ transplantation | 25 (7.6%) | 127 (3.5%) |
| PHQ-4 grade | ||
| Normal | 249 (76.4%) | 3273 (89.3%) |
| Mild | 61 (18.7%) | 311 (8.5%) |
| Moderate | 14 (4.3%) | 53 (1.4%) |
| Severe | 2 (0.6%) | 27 (0.7%) |
|
| ||
| Infection data type | ||
| Swab test | 312 (95.4%) | 3429 (93.5%) |
| Antibody test | 12 (3.7%) | 48 (1.3%) |
| Symptoms only | 3 (0.9%) | 190 (5.2%) |
| Likely SARS-CoV-2 variant | ||
| Pre-Omicron | 172 (52.6%) | 575 (15.7%) |
| Omicron | 155 (47.4%) | 3092 (84.3%) |
| Self-reported infection severity | ||
| Asymptomatic | 22 (6.7%) | 258 (7.0%) |
| Mildly unwell | 63 (19.3%) | 1402 (38.2%) |
| Moderately unwell | 99 (30.3%) | 1215 (33.1%) |
| Very unwell | 143 (43.7%) | 792 (21.6%) |
| Number of acute symptoms | 4 (3–5) | 2 (1–3) |
| Vaccinated at time of infection | 229 (70.0%) | 3443 (93.9%) |
| Follow-up since infection, months | 12.2 (8.5–15.3) | 16.0 (11.3–22.4) |
| Main analysis | Main analysis, adjusted for infection-related variables | Sensitivity 1: test-positive only | Sensitivity 2: higher symptom burden | |||||
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | OR (95% CI) | P value | |
| Sleep quality | ||||||||
| Good | 1 (ref) | 1 (ref) | 1 (ref) | 1 (ref) | ||||
| Medium | 1.36 (1.02 to 1.80) | 0.036 | 1.32 (0.98 to 1.78) | 0.072 | 1.27 (0.94 to 1.73) | 0.123 | 1.37 (0.95 to 1.97) | 0.088 |
| Medium–low | 1.49 (1.06 to 2.09) | 0.023 | 1.49 (1.04 to 2.13) | 0.028 | 1.48 (1.03 to 2.13) | 0.036 | 1.93 (1.29 to 2.90) | 0.001 |
| Low | 1.95 (1.09 to 3.49) | 0.025 | 2.02 (1.07 to 3.80) | 0.030 | 2.00 (1.05 to 3.81) | 0.035 | 2.58 (1.32 to 5.04) | 0.006 |
| | 0.022 | 0.024 | 0.026 | 0.002 | ||||
| Sleep midpoint | 0.99 (0.88 to 1.10) | 0.797 | 1.00 (0.89 to 1.11) | 0.961 | 0.98 (0.87 to 1.10) | 0.698 | 0.99 (0.87 to 1.12) | 0.830 |
| SD of mid-sleep point (10 min) | 0.99 (0.96 to 1.02) | 0.448 | 0.99 (0.96 to 1.02) | 0.432 | 0.99 (0.96 to 1.03) | 0.643 | 0.99 (0.96 to 1.02) | 0.470 |
| SD of sleep efficiency (%) | 1.04 (0.99 to 1.09) | 0.128 | 1.07 (1.02 to 1.12) | 0.010 | 1.07 (1.02 to 1.12) | 0.010 | 1.07 (1.02 to 1.13) | 0.011 |
| SD of time asleep (10 min) | 1.02 (0.94 to 1.11) | 0.797 | 0.98 (0.90 to 1.07) | 0.691 | 0.98 (0.90 to 1.07) | 0.683 | 1.02 (0.93 to 1.12) | 0.717 |
| Participants (n=6860) | |
|---|---|
|
| |
| Age, years | 63.0 (54.2–69.1) |
| Sex | |
| Female | 4898 (71.4%) |
| Male | 1962 (28.6%) |
| Ethnicity | |
| White | 6595 (96.1%) |
| Black, African, Caribbean or Black British | 28 (0.4%) |
| South Asian | 100 (1.5%) |
| Mixed, multiple or other | 137 (2.0%) |
| IMD decile | 7 (5–9) |
| Highest educational level attained | |
| Primary or secondary | 671 (9.8%) |
| Higher or further (A levels) | 956 (13.9%) |
| College or university | 3093 (45.1%) |
| Post-graduate | 2140 (31.2%) |
| Follow-up, months | 29.4 (24.4–32.5) |
|
| |
| Sleep duration, h | 6.8 (1.0) |
| Sleep quality | |
| Good | 2290 (33.4%) |
| Medium | 2731 (39.8%) |
| Medium–low | 1508 (22.0%) |
| Low | 331 (4.8%) |
| Reported sleep problems | 2247 (32.8%) |
|
| |
| BMI, kg/m² | |
| <25 | 3416 (49.8%) |
| 25 to <30 | 2208 (32.2%) |
| ≥30 | 1236 (18.0%) |
| General health | |
| Excellent | 1446 (21.1%) |
| Very good | 2855 (41.6%) |
| Good | 1794 (26.2%) |
| Fair | 631 (9.2%) |
| Poor | 134 (2.0%) |
| Asthma or COPD | 1156 (16.9%) |
| Autoimmune disease | 611 (8.9%) |
| Diabetes | |
| Pre-diabetes | 6348 (92.5%) |
| Diabetes | 212 (3.1%) |
| Heart disease | 259 (3.8%) |
| Hypertension | 1502 (21.9%) |
| Immunosuppression or organ transplantation | 322 (4.7%) |
| Medications | |
| Benzodiazepines | 29 (0.4%) |
| Non-benzodiazepine hypnotics and sedatives | 79 (1.2%) |
|
| |
| Infection data type | |
| Swab test | 6353/6855 (92.7%) |
| Antibody test | 123/6855 (1.8%) |
| Symptoms only | 379/6855 (5.5%) |
| Self-reported infection severity | |
| Asymptomatic | 445 (6.5%) |
| Mildly unwell | 2171 (31.6%) |
| Moderately unwell | 2244 (32.7%) |
| Very unwell or hospitalised | 2000 (29.2%) |
| Ever reports long COVID | 333 (4.9%) |
- —AIM Foundation
- —Hyphens Pharma
- —http://dx.doi.org/10.13039/100001605Epilepsy Foundation
- —UKRI Industrial Strategy Challenge Fund
- —http://dx.doi.org/10.13039/501100022603DSM Nutritional Products
- —Health Data Research UK BREATHE Hub
- —Thornton & Ross
- —Karl R Pfleger Foundation
- —NIHR Clinical Research Network
- —Cytoplan
- —Pharma Nord
- —SYnergy Biologics
- —Warburtons
- —http://dx.doi.org/10.13039/100015652Barts Charity
- —Fischer Family Foundation
- —http://dx.doi.org/10.13039/100014013UK Research and Innovation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLong-Term Effects of COVID-19 · Sleep and related disorders · COVID-19 and Mental Health
Introduction
Long COVID, which describes the post-acute sequelae of SARS-CoV-2 infection, is estimated to affect at least 10% of people who are infected.1 One of the most common symptoms of long COVID is poor sleep quality, which is reported by an estimated 45% of COVID-19 survivors after both mild and severe disease.24 However, different timings of assessment across studies and infrequent follow-up have made it difficult to track the trajectory of sleep after infection,5 with the majority of data only covering the first 6 months after infection.2 Additionally, few studies have factored in pre-infection sleep,2 6 and those that do often rely on retrospectively collected data, which is subjected to recall bias and can be unreliable.7 The situation is further complicated by the economic and public health restrictions present during the COVID-19 pandemic, during which stress, restrictions to movement, loss of morning commutes and changes to employment are likely to have increased or decreased sleep duration and quality at different timepoints, independently of infection.7 8
Importantly, the relationship between sleep and long COVID may be bidirectional. Pre-existing sleep problems have been shown to increase the risk of upper respiratory infections, including influenza and SARS-CoV-2, as well as hospitalisation with COVID-19.9 Sleep quality has also been implicated in the development of long COVID among those infected, with studies finding a wide range of sleep-related measures such as sleep quality, sleep duration and pre-existing sleep disorders predicting the development of long COVID.1013 This research, however, is still in its infancy, with studies presenting conflicting findings on the associations with different sleep measures10 11; heterogeneity between study definitions of long COVID, ranging between symptoms lasting 4 weeks10 and 6 months12; and reliance on retrospectively reported pre-infection sleep data.12 More research is therefore needed to build our understanding of this relationship.
Understanding the role of sleep in long COVID risk and recovery is of key importance, both in preventing and treating long COVID as well as preventing the known negative impacts of poor sleep, such as reduced quality of life14 and poorer health outcomes.15 With prospectively collected data on pre-infection sleep and regular long-term follow-up of post-infection sleep, the COVIDENCE UK cohort study (https://www.qmul.ac.uk/covidence) is well placed to examine the bidirectional relationship between sleep and long COVID. We therefore aimed to evaluate how pre-infection sleep quality is associated with risk of long COVID and to track changes in sleep duration during the year after SARS-CoV-2 infection.
Methods
Study design and participants
COVIDENCE UK is a prospective, longitudinal, population-based observational study of COVID-19 in the UK population.16 Inclusion criteria were age 16 years or older and UK residence at enrolment, with no exclusion criteria. Participants were invited through a national media campaign via print and online newspapers, radio, television, social media and online advertising. Participants who enrolled in the study completed an online baseline questionnaire and monthly follow-up questionnaires to capture information on potential symptoms of COVID-19, results of nose or throat swab tests for SARS-CoV-2, long COVID and sleep characteristics. The study was launched on 1 May 2020 and closed to enrolment on 6 October 2021. This analysis uses follow-up data to June 2023. The final COVIDENCE UK cohort was majority women (70.2%) and white (93.7%), with under-representation of people younger than 50 years, men and minoritised ethnicities.16 This study is registered with ClinicalTrials.gov, NCT04330599.
For this analysis of COVIDENCE UK data, we excluded participants who had been hospitalised with COVID-19 to focus on community cases. We additionally excluded participants with less than 12 weeks of follow-up after their infection date.
Patient and public involvement
The COVIDENCE UK study design and development of participant-facing materials were guided by a team of patient and public involvement representatives. Patients and the public were not involved in the conduct, reporting or dissemination plans of this research.
SARS-CoV-2 infection
We defined evidence of a SARS-CoV-2 infection as a positive SARS-CoV-2 swab test or antibody test. As many people with long COVID were infected before widespread testing was available, we also included symptom-defined COVID-19 (based on the algorithm described by Menni et al17) with no concurrent negative SARS-CoV-2 test. Participants additionally reported the severity of their symptoms as mild (able to do most of usual activities), moderate (unable to do usual activities, but without requiring bedrest) or severe (requiring bedrest).
Infection dates were defined as the date of the test, for swab tests, and the date of symptom onset, for participants with symptom-defined COVID-19. Participants reporting positive antibody tests were asked to recall a suspected infection date (based on symptoms, swab test results or close proximity to a COVID-19 case); participants unable to provide a date, who nonetheless reported probable COVID-19 symptoms17 before their antibody test, were assigned the symptom onset date as their infection date.
To enable inclusion of pre-infection data, time since infection was included as a categorical variable with the following categories: no infection, infection within the past month, infection 1–3 months before, infection 3–6 months before, infection 6–9 months before and infection 9–12 months before. We chose these categories to enable a clearer distinction between the effects of the acute infection (≤1 month), ongoing symptomatic COVID-19 (1–3 months) and different phases of post-COVID-19 syndrome (>3 months).
We classified the likely SARS-CoV-2 variant as pre-Omicron or post-Omicron according to infection date, with the threshold set at 20 December 2021.18
Long COVID
Long COVID is variably defined by public health bodies as symptoms occurring more than 4 weeks after infection19 20 or more than 12 weeks after infection21; there is still no international consensus. We therefore defined long COVID as at least two consecutive positive responses to the question ‘Would YOU say that you currently have “long COVID”, that is, ongoing symptoms more than 4 weeks after the onset of proven or suspected COVID-19?’ occurring at least 4 weeks after the participant’s first recorded infection date, and with at least one positive response more than 12 weeks after their first reported infection.
We constructed this definition to reflect a minimum frequency and persistence of ongoing symptoms—that is, symptoms occurring at least 4 weeks after the acute infection, with a duration of at least 2 months, and without having resolved by 12 weeks post-infection. Participants were defined as not having long COVID if they never reported possible or suspected long COVID during follow-up.
Participants reporting long COVID were asked to report on 16 potential long COVID symptoms, covering gastrointestinal, neurological, musculoskeletal and cardiopulmonary problems; details on these symptoms have been published elsewhere.22
Sleep quality
We included measures of sleep that reflected timing, duration, efficiency and variability, using a subset of questions from the Pittsburgh Sleep Quality Index designed to measure sleep duration and sleep efficiency (online supplemental appendix p 2).23 The questions used in COVIDENCE UK focus on sleep duration and sleep efficiency. In each monthly questionnaire, participants are asked to report the average hours of actual sleep from the past month. Up to May 2021, participants were also asked to report average sleep times (ie, when they turned out the lights in order to sleep) and rising times (ie, when they got up). Between October 2020 and May 2021, all participants were asked to additionally report whether they were experiencing problems sleeping, regardless of their infection status; after May 2021, only participants reporting long COVID were asked to report on sleep problems.
We calculated the midpoint of sleep as the rising time minus half the hours spent asleep. We calculated sleep efficiency as the percentage of time in bed (ie, time between sleep times and rising times) spent asleep. Owing to strong collinearity between sleep duration and sleep efficiency, we constructed a sleep quality variable based on age-specific recommendations from the National Sleep Foundation (online supplemental appendix figure S1).24 25 For variability, we included the SD of sleep midpoint, sleep duration and sleep efficiency, calculated over all surveys completed at least 7 days before the infection date.
For pre-infection sleep, we used sleep data taken from each participant’s baseline survey, or their first pre-infection monthly survey if baseline measures were unavailable (<1% of participants).
Covariates
We identified potential risk factors for long COVID from the literature (online supplemental appendix table S1). Focusing on those that might be associated with sleep quality,26 27 we constructed directed acyclic graphs (DAGs) to identify potential confounders and to establish whether any adjustments could introduce bias (online supplemental appendix figure S2). Based on our DAG, the minimally sufficient adjustment set comprised age; sex; body mass index; socioeconomic status, as captured by the Index of Multiple Deprivation28 (in quartiles) and highest level of educational achievement (categorised as primary or secondary, higher or further, college or university, or postgraduate); baseline health, comorbidities and anxiety or depression; and level of physical activity (categorised as 0 hour, 1–3 hours or ≥4 hours of vigorous physical activity per week). To increase statistical power, we used the number of comorbidities each participant had from the following list: diabetes, heart disease (coronary artery disease or heart failure), hypertension, respiratory disease (asthma or chronic obstructive pulmonary disease; COPD) and immunosuppressants or organ transplantation. These comorbidities are present in the COVIDENCE UK dataset and have all been found to be associated with long COVID (online supplemental appendix table S1). We adjusted separately for self-reported general health, and for presence of anxiety and depression, based on the Patient Health Questionnaire-4.29
For our analysis of post-infection sleep, we additionally included current employment status (defined as employed/working, not employed/working (unemployed, furloughed or retired), or other) and vaccination status (any SARS-CoV-2 vaccines vs none; online supplemental appendix figure S3).
Statistical analysis
For our analysis of long COVID risk, we included all participants with evidence of a SARS-CoV-2 infection and pre-infection sleep data for all characteristics investigated. We carried out binary logistic regressions among infected participants, with pre-infection sleep characteristics as the exposures and long COVID as the outcome. Based on our DAG (online supplemental appendix figure S2), we fitted an initial model without infection variables to estimate the total effect of pre-infection sleep characteristics on long COVID risk, and then included infection-related variables to explore how much infection severity mediated this effect, comparing model fit with the likelihood ratio test. We used orthogonal polynomial contrasts to test for linear trends in the ordinal sleep quality variable.
For our analysis of post-infection sleep, we included all participants with evidence of a SARS-CoV-2 infection who had data on pre-infection sleep quality and sleep problems. We carried out a repeated-measures analysis of average monthly sleep duration, with time since infection as the exposure, using multilevel linear mixed models with random intercepts for participants. We censored cases at 1-year post-infection or if they were reinfected. To explore how reporting long COVID manifests in sleep duration, we defined a three-level, time-varying long COVID variable: does not report long COVID, reports long COVID without sleep problems and reports long COVID with sleep problems. Further details on the model are included in the online supplemental appendix (p 8).
We did several sensitivity analyses. First, to reduce the risk of misclassification, we restricted all analyses to people with test-confirmed COVID-19. Second, to explore the effect of sleep on different severities of long COVID, we calculated the total number of the 16 potential long COVID symptoms22 reported by each individual with long COVID and restricted the long COVID risk analysis to those who reported more than five of the 16 symptoms included (ie, excluding the lowest quartile). Third, to ensure better comparability between baseline sleep data, we restricted the post-infection sleep analysis to participants with pre-infection sleep data from the first month that both sleep quality and sleep problems data were collected (October 2020). Finally, to assess the individual contributions of sleep duration and sleep efficiency towards long COVID risk, we carried out exploratory analyses substituting each variable in the model in the place of sleep quality.
We handled missing data with listwise deletion, under the assumption that data were missing at random, and that missingness was independent of the outcome variable, conditional on the covariates (online supplemental appendix pp 9–12 and tables S2 and S3).30 We then explored potential selection bias using inverse probability weighting for logistic regressions.30 All data were analysed with Stata/MP V.18. A p value of less than 0.05 was considered significant.
Results
Long COVID risk analysis
Between May 2020 and March 2021, we enrolled 3994 participants who were included in our analysis of long COVID risk (online supplemental appendix figure S4). SARS-CoV-2 infections were recorded between July 2020 and March 2023. Participants were followed up for a median of 13.1 months (IQR 9.0–16.4) after their SARS-CoV-2 infection, during which 327 (8.2%) reported long COVID a median of five times (IQR 3–9; table 1). Compared with participants who did not report long COVID, those reporting long COVID were more likely to be younger and female, with lower levels of educational attainment, lower levels of physical activity, worse general health, higher body mass index, and a greater burden of comorbidities (table 1). Participants reporting long COVID were also more likely to have been infected before the Omicron variant was dominant and to have experienced a more severe acute infection and were less likely to have been vaccinated at the time of infection (table 1).
We found an association between pre-infection sleep quality and long COVID, with p-for-trend analyses suggesting higher risk of long COVID with lower sleep quality, regardless of infection severity (table 2; online supplemental appendix table S4). We additionally observed an association between greater variability in sleep efficiency and increased risk of long COVID, which was significant when adjusted for infection severity (table 2). Our results were similar after applying inverse probability weighting to correct for potential selection bias (data not shown). When considering sleep duration and sleep efficiency separately, we found lower sleep efficiency to be associated with higher risk of long COVID, but we lacked power to detect any association between sleep duration and long COVID (online supplemental appendix table S5). Restricting our analysis to participants with test-confirmed COVID-19 did not substantially affect our results (table 2; online supplemental appendix table S6). Restricting our analysis to participants who may have a more severe form of long COVID (ie, reporting a greater number of long COVID symptoms) strengthened the association observed for low-quality sleep (table 2; online supplemental appendix table S6).
post-infection sleep analysis
Between May 2020 and June 2021, we enrolled 6860 participants who were included in our analysis of post-infection sleep (table 3; online supplemental appendix figure S5). Their reported SARS-CoV-2 infections occurred between October 2020 and March 2023. Participants were followed up from enrolment for a median of 29 months (IQR 24–32). 2247 (32.9%) participants reported sleep problems at baseline (table 3).
We found that sleep duration increased slightly in the month immediately following a SARS-CoV-2 infection (figure 1; online supplemental appendix tables S7 and S8). The size of this increase was dependent on the severity of the acute infection, with no increase for people who were asymptomatic or had mild disease (figure 1; online supplemental appendix tables S7 and S8). Across all infection severities, no significant changes in sleep duration were observed more than 1 month after infection (figure 1; online supplemental appendix tables S7 and S8). Greater fluctuations in sleep duration were seen when assessing participants according to long COVID status. Participants who reported long COVID without sleep problems experienced a greater increase in sleep duration in the first month after infection, and a slower return to pre-infection sleep duration (figure 1; online supplemental appendix tables S7 and S8). Those who reported long COVID with sleep problems experienced a slight decrease in sleep duration between 1 and 6 months after infection, after which sleep duration returned to pre-infection levels (figure 1; online supplemental appendix tables S7 and S8). However, the number of people with long COVID with sleep problems was small, leading to greater uncertainty in our estimates.
Changes in sleep duration after SARS-CoV-2 infection overall (A) and by infection severity (B) and long COVID status (C). Figure shows estimated changes to sleep duration over time in all participants (A), and according to severity of the acute infection (B) and long COVID status (C). Long COVID status is further categorised according to whether participants were reporting long COVID with sleep problems or long COVID without sleep problems. Estimates shown are contrasts of predictive margins from the regression models, with 95% CIs. Regression estimates are included in the online supplemental appendix tables S7 and S8. Red dashed line indicates pre-infection sleep duration.
When restricting our analyses to participants with pre-infection sleep data from October 2020, we saw a greater reduction and more extended fluctuations in sleep duration among people reporting long COVID with sleep problems (online supplemental appendix table S8). No other substantial changes were observed in our results across our sensitivity analyses (online supplemental appendix table S8).
Discussion
In this large population-based prospective study, we found that poor-quality sleep—defined by the combination of sleep duration and sleep efficiency—and greater variability over time in sleep efficiency before SARS-CoV-2 infection were both associated with increased risk of reporting long COVID. By contrast, we found no evidence that pre-infection sleep timing nor variability in sleep duration affects the risk of long COVID. We observed an increase in sleep duration over the month following a SARS-CoV-2 infection, with greater increases among participants with more severe acute infections. After 1 month, however, sleep duration largely returned to pre-infection levels. Participants reporting long COVID showed greater fluctuations and slower recovery of pre-infection sleep duration, with the direction of change depending on whether their long COVID presented with sleep problems. Estimated changes to sleep were all less than 25 min per night and did not last more than 6 months after infection.
Short sleep duration and sleep disturbances have been found to be associated with increased incidence of upper respiratory tract infections, including COVID-19,9 31 32 as well as poorer outcomes from these infections.9 32 Our longitudinal analysis extends these findings to show the bidirectional nature of the relationship between sleep and COVID-19 within the same cohort. A large cross-sectional study33 of both community and hospitalised COVID-19 cases has previously shown a bidirectional relationship between insomnia and long COVID, reporting increased risk of long COVID among people with prepandemic insomnia and a higher prevalence of post-infection insomnia among people with long COVID. However, this study relied on retrospectively reported sleep data and did not benefit from repeated measures of sleep after infection to track whether insomnia symptoms resolved over time.
We show that the quality of pre-infection sleep predicts long COVID risk, independently of the severity of the acute infection, supporting and extending findings from a previous study10 done exclusively in women. While the mechanisms behind long COVID remain unknown, sleep quality and disturbances are known to play a part in many of the candidate mechanisms under investigation,1 such as persistent inflammation,34 changes to the gut microbiota35 and autoimmunity.34 Sleep problems are additionally linked to poor mental health,36 which has been shown to predict long COVID.37 Our sleep quality measure combined the effects of both sleep efficiency and sleep duration, but exploratory analyses suggested that low and inconsistent sleep efficiency—which can reflect a range of sleep disturbances, such as increased sleep latency and fragmented sleep—was driving the relationship observed. This is in line with other studies, which have found increased risk of long COVID associated with pre-infection sleep disturbances,1012 whereas results on sleep duration are inconsistent10 11 and do not always take into account the simultaneous effect of sleep efficiency.38 Together, these findings suggest short sleep duration, on its own, is unlikely to substantially increase the risk of long COVID; instead, the focus should be on ensuring consistently good-quality sleep to aid recovery from future infections.
The small increase in sleep duration we observed in the month after SARS-CoV-2 infection, followed by a return to pre-infection sleep duration, is consistent with recovery from acute respiratory infection,39 and will reflect the experience of the many people who recover well from SARS-CoV-2 infection. However, our finding that participants with and without long COVID recovered their pre-infection sleep duration within 6 months after infection contrasts with the few other studies that have looked at sleep duration specifically. A cross-sectional survey in both hospitalised and non-hospitalised participants showed a decrease in satisfaction with sleep duration 6 months after infection40; however, this subjective measure of pre-infection sleep was retrospectively reported and the duration itself was not measured. Wearable devices have been used to objectively record sleep duration, showing different results in community and hospitalised cohorts. At 6 months after infection, a cohort of mostly non-hospitalised participants had a mean sleep duration that was 17 min shorter than that of uninfected controls,41 whereas hospitalised participants from the Post-Hospitalisation COVID-19 (PHOSP) cohort reported sleeping for an hour longer at 7 months after infection than a cohort of non-hospitalised controls.3 Our findings may reflect a quicker recovery among less severe cases of COVID-19 as well as the benefit of comparing post-infection sleep duration with prospectively collected pre-infection sleep data; indeed, another study in the PHOSP cohort showed no difference in sleep duration at 8 months after discharge when compared with a different control cohort.42
Although all groups in our analysis recovered their pre-infection sleep duration within 6 months after infection, some participants continued to report long COVID with sleep problems after this period. There is substantial evidence on sleep disturbances after COVID-19,2 43 with an estimated prevalence of 25% after 12 months,2 increasing to 50% among people hospitalised with COVID-19.44 Some facets of sleep health may therefore continue to be affected once pre-infection sleep duration has been recuperated, and further research is needed to better understand how longer term sleep problems manifest in long COVID.
This population-based study has several strengths. Our use of prospectively collected, pre-infection sleep data strengthens our estimates of pre-infection sleep; the majority of studies to date have relied on retrospectively reported pre-infection sleep data,3 33 38 40 41 and research has shown that people asked to retrospectively recall their sleep before the pandemic estimated that they slept much better than they actually did.7 Our extended follow-up enabled us to capture long COVID symptoms presenting at any point after infection and to record sleep duration over the entire year after infection, in contrast with other studies that have relied on a cross-sectional approach,33 40 infrequent assessments11 or shorter follow-up.41 Monthly responses from our participants meant that we were able to track changes in sleep duration with detail that would have been missed if observations had been further apart, while simultaneously allowing us to adjust for time-varying factors that may affect people’s sleep habits—particularly in the context of a pandemic that limited people’s movement and employment.
This study also has various limitations. First, we relied on self-reported measures of sleep, rather than actigraphy or polysomnography data, meaning our response data were subjective and subjected to recall bias. Additionally, as sleep data were reported as monthly averages, we will have missed smaller fluctuations. Second, we were unable to assess changes to sleep quality—a variable defined by both sleep duration and sleep efficiency—after SARS-CoV-2 infection; this is because questions used to calculate sleep efficiency were removed from the COVIDENCE UK questionnaire in May 2021, to reduce the burden on participants. Sleep is a multidimensional entity, and the recovery we observed in sleep duration may not necessarily be reflected in other dimensions of sleep, which should be evaluated in future studies. Third, our study is restricted to community cases of COVID-19, meaning our findings may not reflect the experiences of people with severe disease. However, several studies in hospitalised people have been published6 42; as long COVID occurs across all severities of the initial disease,1 it is important to assess its impact in the community as well as in those hospitalised. Fourth, as the severity of the acute infection may also be associated with pre-infection sleep,9 including people with symptomatic COVID-19 in our reference group may have underestimated the impact of pre-infection sleep on long COVID risk. However, we had too few asymptomatic participants to exclude symptomatic participants from the reference group. Fifth, we lacked detailed data on participants’ use of sleep aids such as hypnotics and sedatives throughout their follow-up, and particularly after infection; as a result, we may have underestimated the effect of SARS-CoV-2 infection on sleep duration if participants experiencing problems supported their recovery with these aids. Sixth, COVIDENCE UK is a self-selected cohort,16 and so certain groups—such as older age groups, women and people of white ethnicity—are over-represented in our study, which may limit the generalisability of our results. Seventh, we analysed our data under the assumption that data were missing at random, which may have biased our results. However, sensitivity analyses using inverse probability weight to correct for potential selection bias resulted in similar findings. Finally, as with any observational study, we cannot rule out the possibility of unmeasured or residual confounding influencing our findings. However, the richness of the data collected in COVIDENCE UK means that we were able to control for various potential confounders in our analyses.
In conclusion, our study highlights the bidirectional relationship between sleep and long COVID, illustrating how poor-quality sleep before SARS-CoV-2 infection may increase the risk of long COVID, and describing changes to sleep duration after SARS-CoV-2 infection. The modest changes to sleep duration we observed in these non-hospitalised cases of COVID-19 largely resolved within 6 months, potentially reflecting a quicker recovery of pre-infection sleep characteristics among less severe infections.
Supplementary material
10.1136/bmjresp-2024-002506online supplemental file 1
10.1136/bmjresp-2024-002506online supplemental file 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Davis HE Mc Corkell L Vogel JM et al Long COVID: major findings, mechanisms and recommendations Nat Rev Microbiol 2023211334610.1038/s 41579-022-00846-236639608 PMC 9839201 · doi ↗ · pubmed ↗
- 2Linh TTD Ho DKN Nguyen NN et al Global prevalence of post-COVID-19 sleep disturbances in adults at different follow-up time points: A systematic review and meta-analysis Sleep Med Rev 20237110183310.1016/j.smrv.2023.10183337597302 · doi ↗ · pubmed ↗
- 3Jackson C Stewart ID Plekhanova T et al Effects of sleep disturbance on dyspnoea and impaired lung function following hospital admission due to COVID-19 in the UK: a prospective multicentre cohort study Lancet Respir Med 2023116738410.1016/S 2213-2600(23)00124-837072018 PMC 10156429 · doi ↗ · pubmed ↗
- 4Carnes-Vendrell A Piñol-Ripoll G Ariza M et al Sleep quality in individuals with post-COVID-19 condition: Relation with emotional, cognitive and functional variables Brain Behav Immun Health 20243510072110.1016/j.bbih.2023.10072138269302 PMC 10806261 · doi ↗ · pubmed ↗
- 5Tedjasukmana R Budikayanti A Islamiyah WR et al Sleep disturbance in post COVID-19 conditions: Prevalence and quality of life Front Neurol 202213109560610.3389/fneur.2022.109560636698905 PMC 9869804 · doi ↗ · pubmed ↗
- 6Choudhry AA Shahzeen F Choudhry SA et al Impact of COVID-19 Infection on Quality of Sleep Cureus 202113 e 1818210.7759/cureus.1818234722016 PMC 8544642 · doi ↗ · pubmed ↗
- 7Gao C Scullin MK Sleep health early in the coronavirus disease 2019 (COVID-19) outbreak in the United States: integrating longitudinal, cross-sectional, and retrospective recall data Sleep Med 20207311010.1016/j.sleep.2020.06.03232745719 PMC 7320269 · doi ↗ · pubmed ↗
- 8Falkingham JC Evandrou M Qin M et al Prospective longitudinal study of “Sleepless in Lockdown”: unpacking differences in sleep loss during the coronavirus pandemic in the UKBMJ Open 202212 e 05309410.1136/bmjopen-2021-053094 PMC 872458034980617 · doi ↗ · pubmed ↗