Challenges in the Recognition and Management of Metastatic Sarcomatoid Carcinoma Masquerading As Post-traumatic Hematoma
Abigayle Wyer, Mena Louis, Richard Adams, Raven Richardson, Ezra Ellis, Brian Gibson

TL;DR
This paper discusses a rare case of metastatic sarcomatoid carcinoma misdiagnosed as a post-traumatic hematoma, highlighting the challenges in diagnosis and treatment.
Contribution
The paper presents a case emphasizing the importance of early biopsy and multidisciplinary care in managing metastatic sarcomatoid carcinoma.
Findings
Delayed diagnosis of metastatic sarcomatoid carcinoma led to complex surgical interventions and postoperative complications.
Immunohistochemical analysis was critical in confirming the pulmonary origin of the carcinoma.
Multidisciplinary care, including psychological support, is essential for managing advanced sarcomatoid carcinoma.
Abstract
Sarcomatoid carcinoma is an aggressive and rare form of cancer characterized by rapid metastatic spread and diagnostic complexity. This case describes a 68-year-old male presenting initially with persistent thigh swelling and pain following minor trauma. His symptoms were accompanied by systemic signs, including night sweats, constipation, abdominal pain, and dark stools. Despite persistent clinical deterioration, initial imaging suggested a benign etiology, such as hematoma or infection, leading to delayed diagnosis. Subsequent CT scans revealed significant intra-abdominal disease involving the bowel and omentum, with metastatic pulmonary involvement identified upon further imaging. Surgical exploration uncovered extensive metastatic sarcomatoid carcinoma originating from the lung, involving the bowel, omentum, and thigh soft tissues, necessitating extensive resection and complex…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
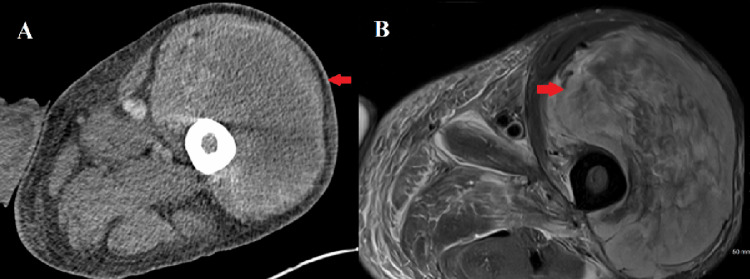 Figure 1
Figure 1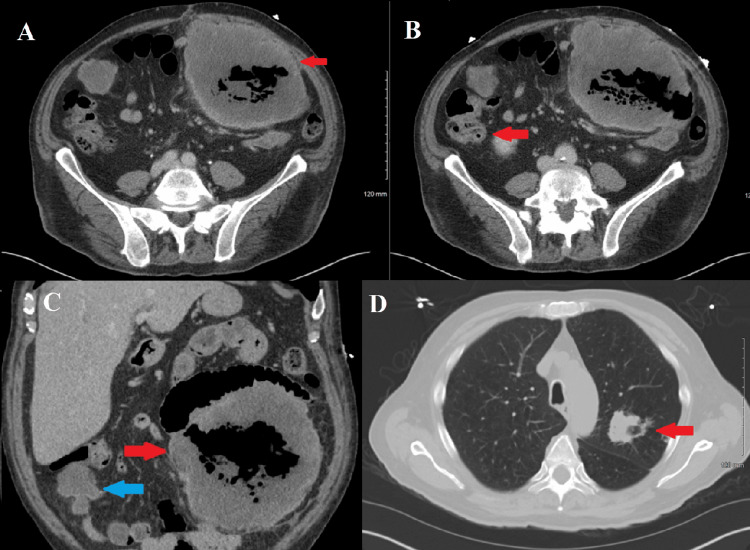 Figure 2
Figure 2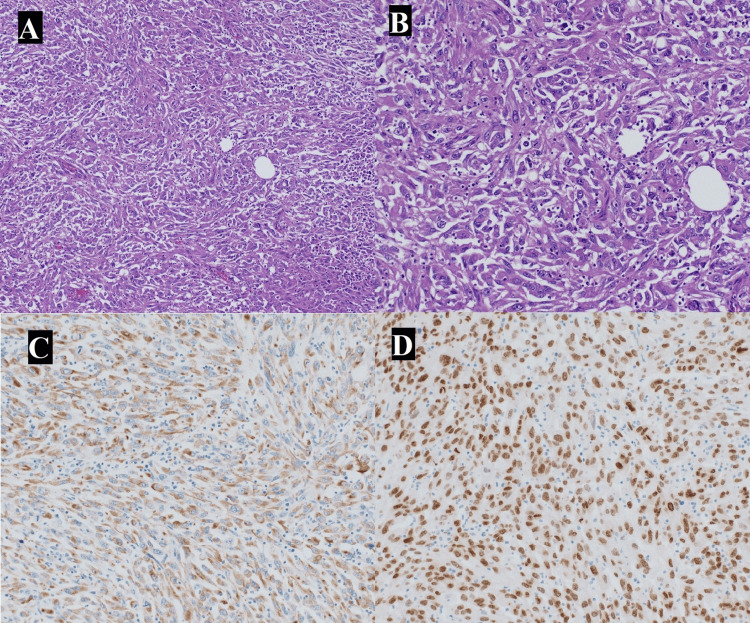 Figure 3
Figure 3| Lab | Value | Reference value |
| White blood cell (WBC) count | WBC 35.8 × 10³/µL | 4,000–11,000 µL |
| Hemoglobin (Hgb) | 12.0 g/dL | 12.0 - 15.5 g/dL |
| Hypoalbuminemia | 2.2 g/dL | 3.5 to 5.5 g/dL |
| Alkaline phosphatase | 220 U/L | 44 and 147 IU/L |
| INR | 1.29 | 0.8 and 1.1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Cancer and Skin Lesions · Cancer Diagnosis and Treatment
Introduction
Sarcomatoid carcinoma is an aggressive and poorly differentiated subtype of carcinoma characterized by both epithelial and mesenchymal histologic features [1]. It most commonly originates in the lungs but may also arise from the kidneys, urinary bladder, or other visceral organs [2]. Clinically, sarcomatoid carcinomas tend to present aggressively, often demonstrating rapid local progression and widespread metastatic disease at diagnosis [3]. This tumor type poses significant diagnostic challenges due to its heterogeneous morphology, nonspecific clinical manifestations, and frequent confusion with benign conditions or primary sarcomas [4].
Metastatic sarcomatoid carcinoma typically involves common metastatic sites such as lymph nodes, liver, bones, and brain [5]. However, unusual presentations, including soft-tissue metastases or extensive intra-abdominal involvement, are relatively uncommon and may obscure initial clinical impressions, complicating early diagnosis and intervention [6]. As such, clinicians must maintain a high degree of suspicion, particularly in cases of persistent and progressive soft tissue lesions or unexplained systemic symptoms such as weight loss, night sweats, and gastrointestinal changes [7].
Soft tissue metastases originating from a primary pulmonary sarcomatoid carcinoma are especially rare, often initially misdiagnosed as trauma-induced hematomas or infectious processes [8]. In these instances, the absence of resolution or progression despite conservative therapy or seemingly appropriate antibiotic regimens should prompt clinicians toward aggressive diagnostic interventions [9]. Definitive imaging combined with early biopsy procedures plays a critical role in establishing accurate diagnoses, guiding subsequent multidisciplinary management, and improving patient outcomes. Considering its aggressive biology, early identification and surgical intervention, complemented by a multidisciplinary approach involving oncology, surgery, radiology, and pathology, are essential to optimize patient care. Despite therapeutic advances, the prognosis remains guarded, reinforcing the necessity for prompt diagnosis, effective symptom palliation, and attentive management of complications [10].
Case presentation
A 68-year-old male with a significant past medical history of coronary artery disease status post two stent placements, asthma, hypertension, cholecystectomy, left inguinal hernia, and an incidental left renal mass presented to the emergency department complaining of left thigh pain and swelling lasting approximately four months. He initially associated the onset of symptoms with minor trauma after striking his leg against a pipe; however, he denied any associated bruising or skin breaks at the injury site. Approximately three months later, persistent swelling and escalating pain in the affected thigh developed, particularly exacerbated by ambulation and the supine position, preventing tolerance of an MRI scan. He additionally reported associated symptoms including constipation, vague abdominal pain, night sweats, and dark, soft stools lasting approximately one month despite self-administering over-the-counter Alka-Seltzer and nightly Tylenol for symptomatic relief.
On initial evaluation, he had a large, painful, swollen left leg mass with no erythema. He did not have abdominal pain on physical exam. Laboratory results revealed marked leukocytosis, mild anemia, hypoalbuminemia, elevated alkaline phosphatase, and a mildly prolonged international normalized ratio (INR) (Table 1). Initial CT imaging demonstrated a sizable heterogenous thigh mass within the anterior muscular compartment measuring 11.0 × 16.3 × 11.3 cm, presumed initially to be a large hematoma (Figure 1, panel A). A subsequent MRI further characterized this lesion as a heterogeneously enhancing mass predominantly involving the vastus lateralis muscle, measuring up to 15.2 cm, again suspected to be a hematoma versus infectious process, with no clear nodularity indicating malignancy (Figure 1, panel B).
The CT scan and MRI of the patientA: CT scan in axial view reveals a left thigh mass in the anterior compartment measuring 11 x 16 x 11 cm (red arrow); B: MRI in axial view reveals a heterogenous peripherally enhancing mass in the anterior compartment of the thigh, predominantly in the vastus lateralis musculature, measuring 15.2 cm (red arrow)
Concurrent CT of the abdomen and pelvis revealed a centrally necrotic peritoneal mass measuring 17.5 cm with satellite lesions, encasing small bowel loops and abutting adjacent bowel with suspicion for transmural invasion, highly suggestive of malignancy (Figure 2, panels A-C). A chest CT demonstrated a mildly spiculated left upper lobe pulmonary mass concerning for malignancy and multiple bilateral pulmonary nodules suggestive of metastatic involvement (Figure 2, panel C). Surgical consultation was recommended given these alarming findings, prompting admission to the trauma and acute care surgery (TACS) service for comprehensive evaluation and intervention.
CT scan of the abdomen and chestA: Axial view of abdomen reveals a centrally necrotic peritoneal mass left of the midline measuring 17.5 cm (red arrow); B: Axial view of abdomen reveals a satellite mass in the right abdomen measuring 5 cm (red arrow); C: Coronal view of abdomen reveals a centrally necrotic peritoneal mass left of the midline measuring 17.5 cm (red arrow) and a satellite mass in the right abdomen measuring 5 cm (blue arrow); D: Axial view of chest reveals a mildly spiculated left upper lobe mass (red arrow)
The patient underwent exploratory laparotomy, transverse colectomy, small bowel resection, partial omentectomy, peritoneal biopsy, and an incisional biopsy of the left thigh lesion. Intraoperatively, extensive metastatic involvement was noted with a necrotic mass intimately adherent to multiple bowel loops and mesenteric tissues, necessitating substantial resection. Pathological evaluation of the excised tissues revealed metastatic, poorly differentiated sarcomatoid carcinoma with immunohistochemical staining positive for pan-cytokeratin, vimentin, carbonic anhydrase IX (CA-IX), cytokeratin 7 (CK7), and thyroid transcription factor 1 (TTF-1), highly consistent with a pulmonary primary (Figure 3, panels A-D). Postoperative management involved addressing significant ileus and transient aspiration pneumonia. The patient gradually improved clinically and was discharged in stable condition after multidisciplinary care and counseling for his metastatic diagnosis.
Histopathology imagesA: Histopathology slide using hematoxylin and eosin stain (H&E) stain demonstrating sarcomatoid carcinoma at 10x magnification; B: Histopathology slide using H&E stain demonstrating sarcomatoid carcinoma at 20x magnification; C: Histopathology slide using pankeratin stain demonstrating sarcomatoid carcinoma; D: Histopathology slide using TTF-1 immunostain demonstrating sarcomatoid carcinomaTTF-1: Thyroid transcription factor 1
Discussion
Pulmonary sarcomatoid carcinoma (PSC) is a rare and aggressive subtype of non-small cell lung cancer (NSCLC), accounting for approximately 0.1% to 0.4% of all malignant lung tumors [11]. Patients are frequently diagnosed at advanced stages of disease, limiting the feasibility of surgical intervention [12]. Furthermore, PSC is notably resistant to first-line chemotherapy, contributing to its poor prognosis [13]. The overall survival rate for PSC is around 20% lower than that of other NSCLC subtypes, which have a reported survival rate of approximately 45%, with a median survival of only 2.3 months at the time of diagnosis [14]. Although gastrointestinal metastases from lung cancer are relatively uncommon, small bowel involvement has been reported in 2.6% to 10.7% of cases [15]. Those at highest risk include men (73%) with a median age of 63.2 years (range: 36.8-79.7), most of whom are current or former smokers (94.6%) [16].
Metastatic sarcomatoid carcinoma is characterized by rapid growth and unusual metastatic spread, frequently resulting in challenging clinical presentations [17]. In this patient, an initially benign-appearing thigh mass following minor trauma diverted attention from the possibility of metastatic cancer. Persistent swelling, increasing pain, and the presence of systemic symptoms such as night sweats, constipation, abdominal pain, and stool changes were critical indicators that warranted earlier suspicion of a malignant process. Physicians should maintain a high degree of suspicion for metastatic disease when benign explanations like trauma or infection fail to account adequately for progressive clinical deterioration or persistence of symptoms.
Radiologic evaluation posed a significant diagnostic challenge in this patient. Initial CT and MRI scans misinterpreted the thigh mass as a hematoma or potential infection, which delayed biopsy and definitive diagnosis. While MRI is superior for soft tissue evaluation, sarcomatoid carcinomas often contain hemorrhagic and necrotic components that mimic benign lesions radiologically [18]. Thus, reliance on serial imaging without definitive tissue sampling risks significant diagnostic delay. Early biopsy, prompted by lack of improvement or worsening symptoms, is essential for correct diagnosis, timely staging, and appropriate management.
Histopathological confirmation through biopsy remains the cornerstone for diagnosing sarcomatoid carcinoma [1]. Immunohistochemical analysis played a pivotal role in identifying the primary site in this patient [13]. Markers such as pan-cytokeratin, CK7, vimentin, CA-IX, and TTF-1 pointed strongly toward a pulmonary origin, thereby shaping subsequent clinical decisions [19]. Accurate immunohistochemistry is invaluable for treatment planning, prognostication, and targeted therapy selection [20].
The intraoperative management of extensive metastatic disease, as demonstrated in this patient, requires meticulous planning and surgical expertise. Extensive tumor involvement and adherence to multiple loops of bowel necessitated significant resection, including small bowel, colon, and omental segments. Recognizing and effectively managing such widespread metastatic lesions intraoperatively can significantly improve symptoms and quality of life. However, postoperative complications such as prolonged ileus, aspiration pneumonia, and wound management difficulties remain important considerations.
Postoperative management demands careful attention to common complications such as ileus and aspiration pneumonia, both evident in this patient’s course [21]. Aggressive fluid resuscitation, nutritional support, and timely pulmonary interventions mitigate the morbidity associated with extensive surgical resections [22]. Monitoring leukocytosis trends and early management of postoperative infections or aspiration events help prevent severe complications, shorten hospital stays, and improve patient recovery outcomes [23].
Additionally, addressing the psychological impact of a metastatic cancer diagnosis is crucial for comprehensive patient care [24]. The patient's acknowledgment of depressive symptoms highlights the importance of early psychiatric consultation and emotional support. Incorporating mental health assessments into routine oncologic care can significantly improve patient coping strategies, adherence to therapy, and overall quality of life during challenging treatment courses [25].
Conclusions
Metastatic sarcomatoid carcinoma presenting with atypical soft tissue involvement poses significant diagnostic and therapeutic challenges. Persistent unexplained soft tissue swelling accompanied by systemic symptoms warrants early biopsy, even if imaging suggests benign pathology. Definitive diagnosis via histopathology and immunohistochemistry, aggressive surgical intervention balanced with careful postoperative management, and multidisciplinary supportive care are essential components in managing this aggressive malignancy effectively. Increased clinician awareness of unusual metastatic presentations and a proactive diagnostic approach significantly enhances patient outcomes and quality of care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcomatoid carcinoma: a clinicopathological dichotomy Cureus Ghosal R Roychowdhury D Chatterjee RP Sultana M Sinha S 016202410.7759/cureus.53565 PMC 1091408238445157 · doi ↗ · pubmed ↗
- 2Characteristics and clinical outcomes of sarcomatoid carcinoma of the lung Clin Lung Cancer Ung M Rouquette I Filleron T 3913971720162710568410.1016/j.cllc.2016.03.001 · doi ↗ · pubmed ↗
- 3Epidemiology of and prognostic factors for patients with sarcomatoid carcinoma: a large population-based study Am J Cancer Res Xu Z Wang L Tu L 3801381410202033294268 PMC 7716166 · pubmed ↗
- 4Sarcomatoid carcinoma presenting as cancers of unknown primary: a clinicopathological portrait BMC Cancer Huey RW Makawita S Xiao L 9651920193162360210.1186/s 12885-019-6155-6PMC 6796453 · doi ↗ · pubmed ↗
- 5Metastatic sarcomatoid carcinoma to bone J Surg Oncol Sabharwal S Li Brizzi CL Wangsiricharoen S Gross JM Strike SA Levin AS Morris CD 1446145212820233765082810.1002/jso.27433 · doi ↗ · pubmed ↗
- 6Metastatic sarcomatoid renal cell carcinoma manifesting as a subcutaneous soft tissue mass J Cutan Pathol Logunova V Sokumbi O Iczkowski KA 8748774420172867545710.1111/cup.12998 · doi ↗ · pubmed ↗
- 7Outcome of patients with metastatic sarcomatoid renal cell carcinoma: results from the International Metastatic Renal Cell Carcinoma Database Consortium Clin Genitourin Cancer Kyriakopoulos CE Chittoria N Choueiri TK 013201510.1016/j.clgc.2014.08.01125450036 · doi ↗ · pubmed ↗
- 8Metastatic sarcomatoid renal cell carcinoma treated with vascular endothelial growth factor-targeted therapy J Clin Oncol Golshayan AR George S Heng DY 2352412720091906497410.1200/JCO.2008.18.0000 · doi ↗ · pubmed ↗