Genetic testing for BRCA1/2 variants in Northern African women with ovarian and breast cancers: a multicentre study of an under-represented ancestry
K.S. Shohdy, L. Kassem, T. Elnahas, E.M. Barsoum, B. Gabriel, H. Elghazawy, S. Lasheen, C. Gourley, H.A. Azim

TL;DR
This study examines BRCA1/2 genetic variants in Northern African women with ovarian and breast cancers, revealing unique patterns and the feasibility of genetic testing in resource-limited settings.
Contribution
The study provides new insights into BRCA1/2 variant frequencies and patterns specific to Northern African ancestry, previously under-represented in genetic research.
Findings
BRCA1/2 pathogenic variants were found in 18.8% of patients, with similar rates to Western populations.
Northern African ancestry showed unique BRCA2 variant patterns not seen in other populations.
A bioinformatic framework reclassified 60% of variants of uncertain significance.
Abstract
There is a lack of studies investigating the burden of BRCA1/2 pathogenic variants (PVs) in Northern African countries using next-generation sequencing (NGS)-based testing in patients with epithelial ovarian (EOC) and triple-negative breast cancer (TNBC). We established a multicentre registry for genetic testing of unselected patients referred from five centres from 2019 to 2022 across Egypt. Germline or somatic BRCA1/2 sequencing was carried out by target enrichment using the AmoyDx® BRCA1/2 Mutation Kit, and sequencing was carried out using the Illumina NextSeq500 system. Genetic testing was successfully carried out for 1349 of 1420 (95%) patients tested (EOC = 1031, TNBC = 318). The median age was 55 years (range 20-86 years). We identified 258 BRCA1/2 PVs affecting 254 (18.8%) patients. The rate of BRCA1/2 PVs in EOC and TNBC was 18.2% and 20.8%, respectively. Although the rate of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
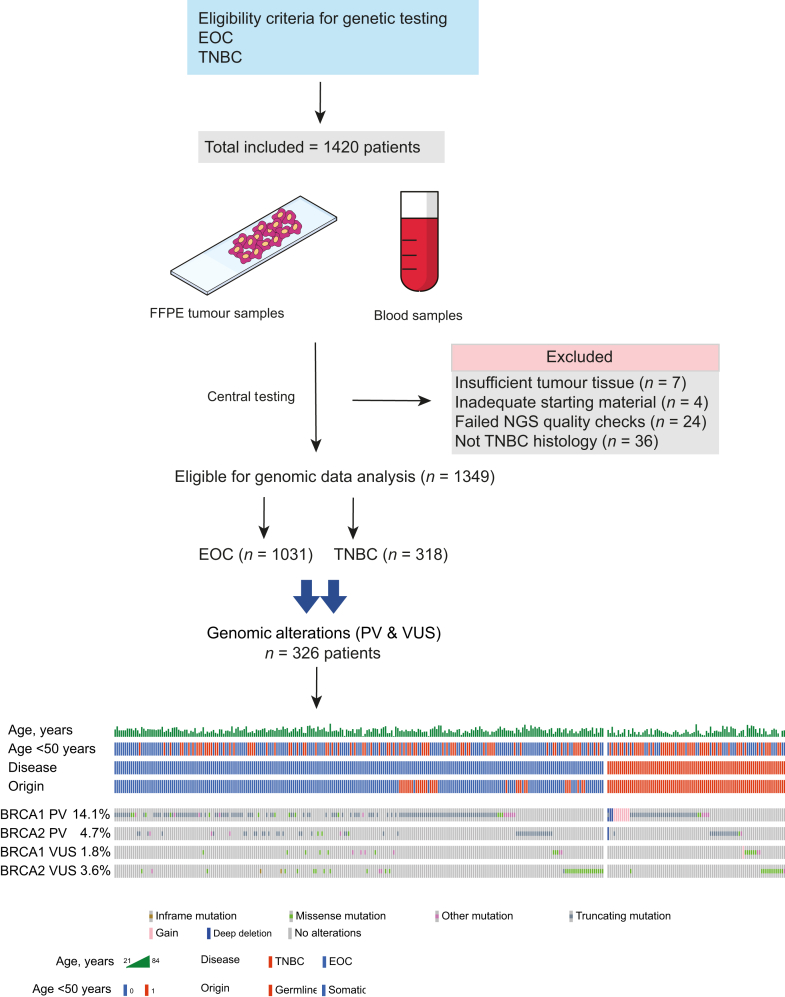 Figure 1
Figure 1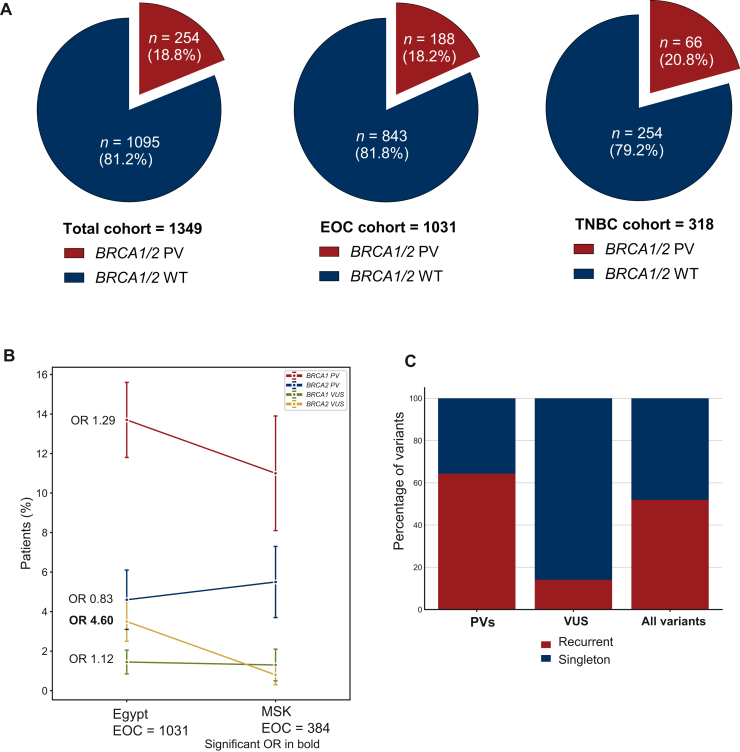 Figure 2
Figure 2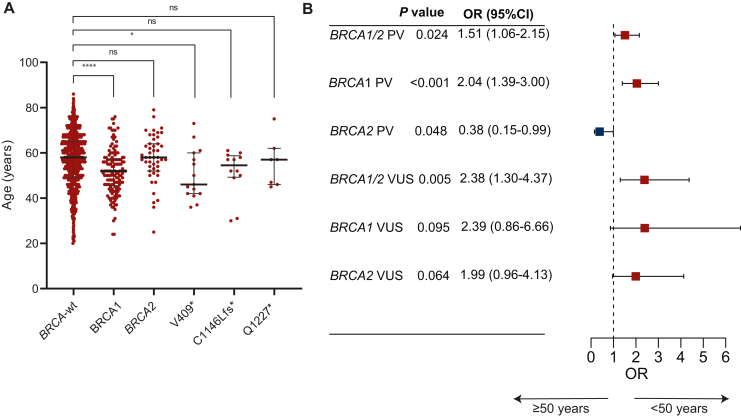 Figure 3
Figure 3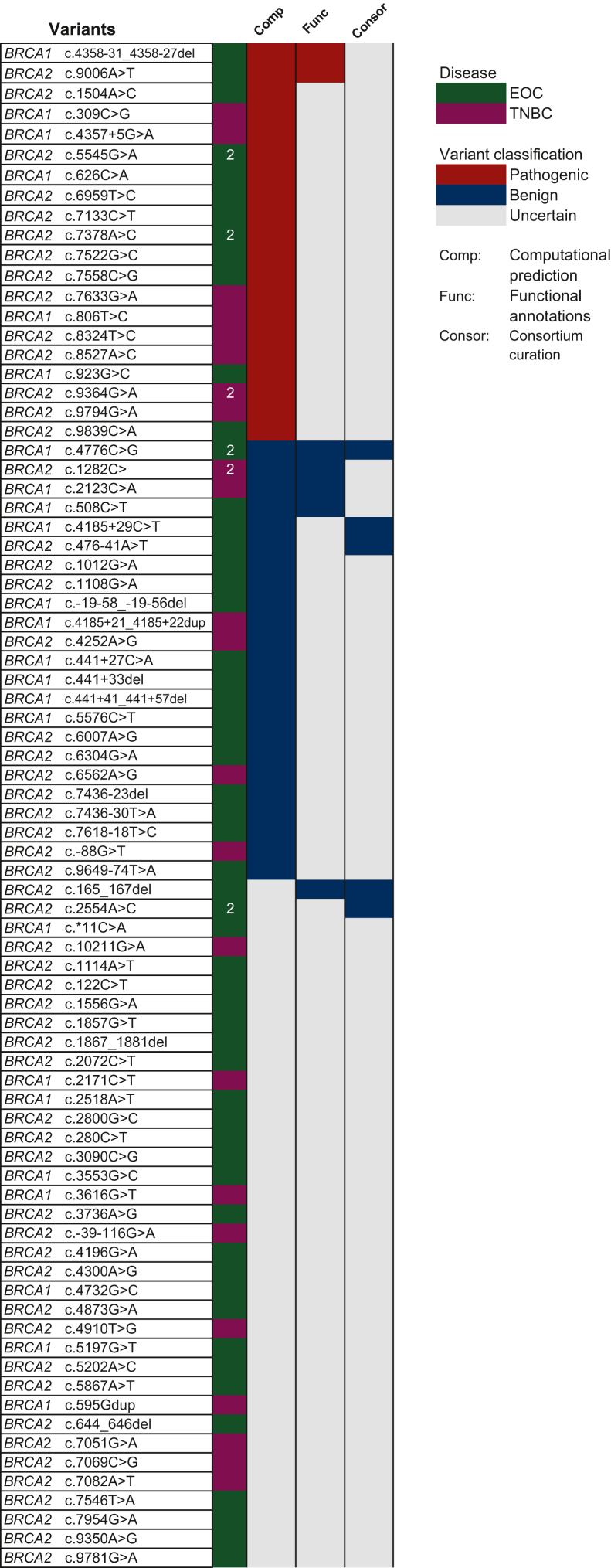 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBRCA gene mutations in cancer · CRISPR and Genetic Engineering · Cancer Genomics and Diagnostics
Introduction
Pathogenic variants (PVs) in BRCA1/2 in patients with ovarian and triple-negative breast cancer (TNBC) were extensively studied in the Western population. However, there is a paucity of studies investigating the burden of BRCA1/2 in Northern African countries using next-generation sequencing (NGS)-based genetic testing. Suboptimal treatment and poorer survival rates have been reported in low-income countries.1 Recent advancements in genomic research have identified the crucial role of BRCA gene mutations in predisposing individuals to hereditary breast and ovarian cancers.2^,^3 The lifetime risk of developing breast or ovarian cancer for BRCA1 carriers is 72% and 44%, respectively and for BRCA2 carriers is 69% and 17%, respectively.4 The presence of BRCA mutations can profoundly impact disease management and treatment outcomes, necessitating a comprehensive understanding of the clinical landscape surrounding these specific patient populations. For instance, specific BRCA mutations can mediate different disease phenotypes.5
Several studies have reported substantially diverse findings on the rate of BRCA mutations in Egyptian women,6, 7, 8 underscoring the need to refine evidence regarding the true prevalence of BRCA in the Egyptian population and the clinical implications. Our group recently conducted a systematic review of the literature that revealed a number of inconsistencies in the germline BRCA (gBRCA) testing for Egyptian women with breast cancer, including an unexpectedly high mutation rate that could indicate issues with the validity of the tests.9 Our study aimed to address these gaps in knowledge by conducting a large-scale registry study to investigate the genetic landscape of patients with breast and ovarian cancer. We sought to define the true prevalence of BRCA PVs in patients using whole-gene NGS analysis and a combined bioinformatic framework that reclassifies the variants of uncertain significance (VUS) in view of the lack of genetic epidemiology, case-control and phenotype data from such understudied ancestry. In addition, we conducted extensive comparisons with the data from multiple Western populations to identify unique BRCA variations in the Northern African ancestry.
Methods
Patient enrolment and tissue acquisition
All experimental procedures were carried out in accordance with approved guidelines and were approved by the Institutional Review Boards at Dar Salam Cancer Centre (Ministry of Health and Population-Egypt No. 2-2024/20). This was a multicentre prospectively maintained registry study that included patients referred from five cancer centres from September 2019 to August 2022 across Egypt. Eligible patients were diagnosed with histologically confirmed TNBC (for which gBRCA1/2 testing was carried out) or newly diagnosed ovarian, fallopian tube or primary peritoneal epithelial cancer (hereafter referred to as epithelial ovarian cancer, EOC) where germline or somatic BRCA1/2 testing was carried out.
Molecular testing
For somatic BRCA1/2 testing, sequencing was carried out on any relevant tissue sample containing an adequate (>30%) proportion of neoplastic cells. Processed formalin-fixed, paraffin-embedded (FFPE) tissue samples and histological sections mounted on unstained glass slides <12 months old were utilized for nucleic acid extraction. Germline testing was carried out using whole blood collected in EDTA tubes. DNA was extracted from FFPE tissue or peripheral blood sample using QIAamp DNA Mini kit (QIAGEN, Hilden, Germany). For FFPE and paired peripheral blood samples, a minimum DNA yield of 50 ng was required. BRCA1/2 NGS was carried out by target enrichment using the AmoyDx® (AmoyDx®, Xiamen, China) BRCA1 and BRCA2 Gene Mutation Detection Kit, and sequencing was carried out using the Illumina NextSeq500 system (Illumina, San Diego, CA). Testing included full gene sequencing and was able to identify single nucleotide variants (SNV), insertions, deletions (InDel) and large gene rearrangements (LRs). The analysis covered all coding exons, the border regions between exons and introns, some introns, and untranslated regions (UTR) of the BRCA1 and BRCA2 genes.
Mutations were called if the following criteria were met: for blood samples, a raw sequencing depth of ≥100×, a mutant allele frequency ≥20%; for fresh tissue and FFPE samples, a raw sequencing depth of ≥300×. Bioinformatic analysis was carried out using the AmoyDx NGS data analysis system software (ANDAS) (AmoyDx®, Xiamen, China) to obtain the related gene variant information. Interpretation of pathogenicity followed the American College of Medical Genetics and Genomics (ACMG) guideline.10 All mutations and genetic variants were referenced to cDNA positions on their respective primary transcripts and named according to the Human Genome Variation Society (HGVS) convention.
The primary endpoint was the prevalence of BRCA1/2 pathogenic variants in Egyptian women with EOC and TNBC. Secondary endpoints included the comparison of the Egyptian PVs and VUS landscape against the publicly available Western populations, in addition to the attempt to reclassify the VUS detected in our series using genomic databases, population data, experimental/functional data and computational prediction tools.
Comparison with the MSK cohort
Clinical and genetic data of the Memorial Sloan Kettering (MSK) EOC cohort (n = 384) were extracted from the supplementary tables.11 All patients underwent prospective sequencing as part of their clinical care using the MSK-IMPACT targeted sequencing panel. Genomic sequencing was carried out on tumour DNA extracted from FFPE and germline DNA was sequenced in all patients. Pathogenicity assessment of BRCA1/2 followed the ACMG, as described in the literature, Richards et al.10
Comparison with the UK diagnostic laboratory cohort
Data on cases who underwent NGS testing for BRCA1/2 at 1 of the 25 molecular diagnostic laboratory and clinical genetics services of the UK (National Health Service) and Ireland were accessible through the Can-Var UK portal.12^,^13
Reclassification of VUS
We conducted a systematic review of the literature for experimental annotations of our VUS and adopted two robust computational tools, the MVP (Missense Variant Pathogenicity prediction) for missense variants14 and SpliceAI for intron variants.15 High-quality experimental data were defined by the cancer variant interpretation group (Can-VIG UK).13 MVP uses a deep residual network for accurate prediction of missense pathogenicity and outperformed all other methods with an area under the curve (AUC) of 0.96 in an independent cohort. Code for missense prediction is available at https://github.com/ShenLab/missense. Variants with MVP scores of ≥0.85 were considered pathogenic. Variants with a score <0.70 were considered benign, and variants with a score between 0.70 and 0.85 were considered VUS.
To predict the pathogenicity of intronic VUS, we ran the SpliceAI pipeline. This package annotates genetic variants with their predicted effect on splicing, as described by Jaganathan et al.15 We used the default parameters including a 500 bp window. The code is available through https://github.com/Illumina/SpliceAI. Variants with a maximum delta score <0.10 are considered benign and variants with a score >0.20 are considered candidate pathogenic. Variants within 0.10-0.20 remained unclassified as VUS.
Statistical analysis
Comparisons of frequencies were analysed based on variable categories with the chi-square or Fisher’s exact test. A comparison of numeric variables was carried out using the Mann–Whitney U test. Logistic regression models and odds ratio (OR) were used to estimate the association between predictor variables and binary outcomes. A P value <0.05 was considered significant. Statistical analyses were conducted with STATA 14.1 (StataCorp, College Station, TX) software and Rstudio (v2024.12.1, Posit Software, PBC, Boston, MA). For gene and variant visualizations, the StJude ProteinPaint and cbioportal tools were used to create oncoplots.
Results
Overview of the study
Samples from 1420 patients were submitted for molecular analysis within the study. A total of 1349 patients completed at least one test and were included in the final analysis (Figure 1). The median age of the eligible cohort was 55 years (range 20-86 years) with one-third younger than 50 years (Table 1). All 318 patients with TNBC underwent gBRCA testing. Among 1031 patients with EOC, 121 (11.7%) had gBRCA only testing (Table 1). Molecular analysis was not successful for 36 patients with EOC. The causes were insufficient tumour tissue (n = 7), inadequate starting material (n = 4) and sequencing output failed quality metrics (n = 24) (Figure 1).Figure 1Overview of the study design, inclusion and exclusion criteria. Lower part is the oncoprint showing patients with clinically relevant variants (n = 326) including BRCA1/2 pathogenic variants (PVs) and variants of uncertain significance (VUS) across our cohort and their baseline characteristics including age, disease [epithelial ovarian cancer (EOC) versus triple-negative breast cancer (TNBC)] and origin of sample (somatic versus germline). The oncoplot was split based on the disease with EOC to the left and TNBC to the right. NGS, next-generation sequencing.Table 1. Characteristics of the eligible patients in the study and the testing outcomesTotal, n (%)EOC, n (%)TNBC, n (%)Eligible patients14201066354Successfully tested patients13491031318Germline testing439 (32.5)121 (11.7)318 (100)Median age, years (range)55 (20-86)57 (20-86)48 (20-83)Age <50 years455 (33.7)285 (27.6)170 (53.5)BRCA1/2 PVs254 (18.8)188 (18.2)66 (20.8)BRCA1/2 VUS72 (5.3)21 (8.3)51 (6.1)BRCA1 PVs190 (14.1)141 (13.7)49 (15.4)BRCA2 PVs64 (4.7)47 (4.6)17 (5.4)BRCA1 VUS24 (1.8)15 (1.5)9 (2.8)BRCA2 VUS48 (3.6)36 (3.5)12 (3.8)BRCA PVs rateAge categories, years 20 to <305 (13.9)1 (5.6)4 (22.2) 30 to <4033 (24.6)15 (22.1)18 (27.3) 40 to <5066 (23.1)46 (23)20 (23.3) 50 to <6093 (22.3)78 (23.3)15 (18.1) 60 to <7037 (10.9)33 (11.3)4 (8.3) ≥7020 (14.7)15 (12.6)5 (29.4)
Egyptian women with EOC/TNBC are enriched with BRCA1/2 pathogenic variants
We identified 343 clinically relevant variants. PVs or likely PVs totalled 258, affecting 254 patients (18.83%), and there were 85 VUS affecting 72 patients (5.34%) (Figure 2A). Across our cohort, two patients had co-occurrence of BRCA1 and BRCA2 PVs (Supplementary Figure S1, available at https://doi.org/10.1016/j.esmoop.2025.105510). The rate of BRCA1/2 PVs in EOC and TNBC was 18.2% (n = 188) and 20.8% (n = 66), respectively.Figure 2Egyptian women with epithelial ovarian cancer (EOC)/triple-negative breast cancer (TNBC) enriched with pathogenic variants (PVs). (A) Pie charts showing the rate of BRCA1/2 PVs in the total cohort and EOC and TNBC subgroups. (B) Comparison of BRCA PVs and variant of uncertain interest (VUS) rate with the Memorial Sloan Kettering (MSK) cohort with EOC. The left bars depict percentages and 95% confidence intervals of the Egyptian EOC cohort (n = 1031) and the right bars depict the MSK cohort (n = 384); statistically significant odds ratios (ORs) are in bold. (C) Percentage of recurrent (occurred in two ore more patients) and singleton (occurred in one patient only) variants identified in the study. WT, wild-type.
We examined the difference between our cohort and a Western population cohort. The MSK EOC cohort was prospectively tested using the MSK-IMPACT panel and the pathogenicity assessment followed the ACMG guidelines (see Methods). No significant difference in the BRCA1/2 PVs was observed between the Egyptian EOC and the MSK EOC cohorts (Figure 2B). It is noteworthy that the Egyptian EOC cohort was significantly enriched with BRCA2 VUS [OR 4.6, 95% confidence interval (CI) 1.41-15.01] (Figure 2B).
Patterns of pathogenic variants and their lineage uniqueness
The PVs were significantly enriched with recurrent variants compared with VUS (64.34% versus 14.11%, P < 0.001) (Figure 2C). The majority of PVs were truncating mutations (either frameshift or nonsense variants, constituting 78.2% and 84.6% of the PVs in BRCA1 and BRCA2, respectively) (Supplementary Figure S2, available at https://doi.org/10.1016/j.esmoop.2025.105510). The most commonly recurrent PVs were BRCA1 V409∗ (n = 21, 8.27%), BRCA1 C1146Lfs∗ (n = 16, 6.30%), BRCA1 Q1227∗ (n = 8, 3.15) and BRCA1 Q1111Nfs∗ (n = 6, 2.36%) (Supplementary Table S1, available at https://doi.org/10.1016/j.esmoop.2025.105510). Three of these top recurrent variants occur in exon 11 of BRCA1 gene and are caused by a deletion of one (V409∗) or four nucleotides (C1146Lfs∗ and Q1111Nfs∗). None of these are reported in normal populations (genomAD). Although the rate of PVs in our cohort was similar to the Western cancer population, there was a significant difference in the enrichment at variant level. Of the top 10 recurrent BRCA1/2 PVs, only 3 PVs were reported in the two large western datasets, the MSK (n = 1610) and the UK diagnostic laboratories cohorts (n = 80 722) (Supplementary Table S1, available at https://doi.org/10.1016/j.esmoop.2025.105510).
We examined the lineage-uniqueness of variants across BRCA1 and BRCA2 in ovarian versus breast cancer (Supplementary Figure S3A and B, available at https://doi.org/10.1016/j.esmoop.2025.105510). We identified 12 recurrent BRCA2 PVs affecting 31 patients. Interestingly, the majority (26/31, 84%) of recurrent BRCA2 PVs were lineage-unique, with only two PVs (affecting five patients) recurrent in both lineages, i.e. ovarian and breast cancer (Supplementary Figure S3A and B, available at https://doi.org/10.1016/j.esmoop.2025.105510) (chi-Square goodness of fit, P = 0.00225). The most common ovarian-unique variants were BRCA2 V1283Kfs∗ and R2272fs (Supplementary Figure S3B, available at https://doi.org/10.1016/j.esmoop.2025.105510). On the other hand, we identified 30 recurrent BRCA1 PVs affecting 130 patients, and only 36% (83/130, 64%) were lineage-unique and 14 PVs were recurrent across both lineages (chi-square goodness of fit, P = 0.19).
Outcomes of BRCA1/2 testing in EOC cohort
A total of 1031 patients with EOC had BRCA1/2 testing, either germline or somatic. The median age of the EOC cohort was 57 years (range 20-86 years). A total of 285 (28%) patients were aged <50 years. The rate of BRCA1/2 PVs was 18.33% (n = 188), with 13.7% (n = 141) occurring in BRCA1 and 4.6% (n = 47) occurring in BRCA2 (Figure 1B and Table 1). The most common type of PV in the EOC was truncating mutation (n = 155, 82.01%). The missense and splice variants occurred in 19 (10.05%) and 15 (7.94%) women, respectively. The most common PVs were BRCA1 V409∗ (n = 15, 7.98%), BRCA1 C1146Lfs∗ (n = 12, 6.38%) and BRCA1 Q1227∗ (n = 7, 3.72%). Seventy-one PVs were singletons (occurred once only) and were detected in 37.7% of women harbouring BRCA1/2 PVs. The majority of EOC patients had somatic testing, with a subgroup of only 121 (11.7%) patients having germline testing. The rate of BRCA1/2 PVs was similar in the germline subgroup compared with the somatic testing group (19% versus 18.1%).
We examined the association of age at diagnosis with BRCA1/2 PV status in the EOC cohort. Patients with BRCA1 PVs had a significantly younger median age at diagnosis compared with BRCA1/2 wild-type subgroup (Figure 3A and B). This was not evident with BRCA2 PVs. Interestingly, the top recurrent PV, BRCA1 V409∗, was associated with the youngest age (Figure 3A). The rates of BRCA1/2 PVs and VUS were not statistically significant across different age groups (Supplementary Figure S4, available at https://doi.org/10.1016/j.esmoop.2025.105510). In addition, we ran logistic regression analysis using age 50 years as cut-off. BRCA1 PVs were more likely to occur at younger age (<50 years) (OR 2.04, P < 0.001), while BRCA2 PVs were less likely to occur at younger age (OR 0.38, P = 0.048) (Figure 3B). There was a trend of BRCA1 and BRCA2 VUS to occur at younger age (Figure 3B).Figure 3BRCA1/2 and age of onset.** (A) The age distribution of patients with BRCA1 and BRCA2 pathogenic variants (PVs) compared with wild-type. Also included separately the top three recurrent BRCA1 variants. (B) Forest plot of the odds ratio (OR) and 95% confidence interval (CI) of BRCA1/2 PV and variants of uncertain interest (VUS) in women age categorized at 50 years.
Outcomes of germline testing of TNBC cohort
Germline genetic testing was successfully carried out for a total of 318 patients with TNBC. The median age was 48 years (range 22-71 years). Sixty-seven (21%) of patients harboured germline PVs in BRCA1/2 (Table 1). The frequency of PVs in BRCA1 was significantly higher than in BRCA2 [49 patients (15%) versus 17 (5%) patients, P < 0.0001]. Patients with BRCA1 PVs were significantly younger, with a median age of 43 years versus 49 years (P = 0.0.003), and no significant difference in the median age was observed in BRCA2 PV carriers (51 years versus 47.5 years, P = 0.051). Patients with BRCA1/2 VUS did not significantly differ in median age from patients with BRCA wild-type (54 years versus 48 years, P = 0.47).
Egyptian patients are enriched with intron VUS and fewer missense variants
The ClinVar database hosted at the United States National Library of Medicine largely depends on submissions from the Western population. We compared the frequency of VUS class types in ClinVar with our current cohort. We extracted 12 391 VUS reported in ClinVar. The most common variant type in the ClinVar database was missense (n = 11 214, 90.5%). Our cohort was significantly enriched with intron variants compared with ClinVar VUS (16.5% versus 4.4%, P < 0.0001) (Supplementary Figure S5, available at https://doi.org/10.1016/j.esmoop.2025.105510). Meanwhile, our cohort was less enriched with missense variants (76.5% versus 90.5%, P < 0.0001). Splice variants showed no significant difference (1.18% versus 0.83%, P = 0.72). There was no significant difference in other variant classes (P > 0.05) (Supplementary Figure S5, available at https://doi.org/10.1016/j.esmoop.2025.105510).
Experimental and computational reclassification of VUS
We undertook a systematic approach to reclassify the identified VUS in our cohort (n = 85 variants) (Figure 4). We adopted a combined approach including computational prediction, functional annotations from high-quality experimental data and academic consortia curation to reclassify the identified VUS (see Methods). Using academic consortia curation, namely ClinVar and Can-Var, five variants were reclassified as benign including BRCA2 c.165_167del and c.476-41A>T. The majority remained of uncertain significance. No large-scale healthy control data are available for the Egyptian population. The majority (68%, 58/85) of the identified VUS were not reported in the GenomAD population. We ran a computational pipeline (MVP) for missense VUS variants in our cohort (Figure 4). A total of 18 missense VUS (affecting 21 patients) were candidate pathogenic variants, 11 missense VUS (affecting 13 patients) were candidate benign variants. Variants with borderline scores or that failed to be scored remained VUS (Supplementary Figure S6, available at https://doi.org/10.1016/j.esmoop.2025.105510).Figure 4Variants of uncertain interest (VUS) reclassification. List of the VUS and their reclassification status based on computational prediction and functional data. Green colour represents epithelial ovarian cancer (EOC) and magenta represents triple-negative breast cancer (TNBC); variants occurred in two patients indicated by number ‘2’. VUS reclassified as pathogenic represented with red colour, blue for benign reclassification and grey for VUS that remained uncertain.
We conducted a systematic review of the literature for functional and experimental analysis of these variants. High-quality data defined by the cancer variant interpretation group (Can-VIG UK) were available for seven variants affecting nine patients, and they were all concordant with the computational predictions (Figure 4). This combined approach achieved a reclassification rate of 52.3% (34/65). Similarly, we ran SpliceAI for the intron variants (n = 15). Two variants were predicted to lead to loss of splice region site and are considered candidate pathogenic, and the remaining 12 were shown to have no impact on the splicing except one variant with a borderline score considered uncertain.
Taken together, our combined approach provides a reclassification of 45 variants (affecting 60% of patients). Our reductionist reclassification approach is feasible in limited resource settings in the context of the lack of case-control and genetic epidemiology data.
Discussion
To our knowledge, this is the largest study to provide comprehensive BRCA1/2 testing for Egyptian patients with EOC or TNBC. For the first time, we were able to provide a reliable prevalence of BRCA1/2 mutations in these diseases with a thorough dissection of the patterns of PVs. Additionally, we could provide a limited resource-conscious approach to gain insights into the pathogenicity of VUS.
We could verify some recurrent PVs in the Egyptian series that differ from other ethnicities. For example, the V409∗ variant was the most common PV in our series. The BRCA1 V409∗ variant was initially reported in the Japanese population16 but was recently reported in the Arab population.17^,^18 The BRCA1 Q1111Nfs∗ is an internationally distributed founder mutation, with a common ancestral origin recently attributed to Iberia.19 The fact that these recurrent mutations affect BRCA1 exon 11 may have therapeutic relevance because there is evidence that tumours that harbour BRCA1 exon 11 mutations can derive platinum and poly (ADP-ribose) polymerase (PARP) inhibitor resistance through generation of an exon 11-skipped hypomorphic isoform that partially restores BRCA1 function.20 Notably, the three Ashkenazi Jewish pathogenic founder mutations (BRCA1 185delAG, BRCA1 5382insC and BRCA2 c.5946del) were not detected in our cohort.
One important aspect we tried to explore is the lineage-unique PVs. We observed that the majority of the identified BRCA2 PVs were specific to one disease (either EOC or TNBC). This may be of importance when counselling the BRCA1/2 carriers about possible risk reduction strategies. Several nomograms are being developed to predict the future risk of having breast cancer, contralateral breast cancer or EOC in women with gBRCA mutations depending on several factors, one of them being the type of PV in BRCA1/2 gene. With the scarce data from Northern African or Egyptian women, our data could provide a deeper insight into this aspect.
The BRCA1/2 PV prevalence showed similarity in age distribution compared with the Western series.11 Specifically, our findings were consistent with other studies showing that BRCA1-mutant EOC is associated with younger age; meanwhile, BRCA2-mutant is not.21^,^22 This was observed, despite the significantly lower age of incidence (and lower life expectancy) in Egypt.
Limited resource settings suffer from a lack of genetic epidemiology, case-control, segregation and phenotype data, which makes VUS interpretation challenging. We showed that by adopting a reductionist approach relying on computational prediction and functional annotations, it is feasible to reclassify up to 60% of the identified VUS.
One of the key strengths of this study is applying whole gene sequencing and not limited to specific hotspot regions of the BRCA1/2 genes. This allows us to identify splice site, UTR and intronic variants. We believe that a significant pool of clinically relevant variants would have been missed if a restricted hotspot panel had been applied.
One of the limitations of this study is the lack of treatment outcomes. As in other limited-resource settings, PARP inhibitors are not reimbursed in the public health care system in Egypt. However, our findings helped to delineate the rate of patients who likely will benefit from precision-oncology-based management. Our VUS reclassification approach should be used cautiously in settings where there is lack of genetic epidemiology and case-control phenotype data with ongoing auditing and validation. Recently, the ongoing Egypt Genome project has been launched, aiming to sequence 100 000 healthy Egyptian individuals and 8000 individuals with disease, including top prevalent malignancies.23 The project aims to build an Egyptian genome reference that encompasses the genetic variants among Egyptians. These data will be valuable to validate our preliminary findings once available in the near future.
Our results will guide the integration of NGS-based testing into the clinical management of patients with breast and ovarian cancer, especially those from understudied ancestries. Furthermore, the findings we derived from whole gene analysis will inform the design of focused initial screening genetic testing. Our cohort is enriched with intronic variants. Again, this carries important implications against the restricted approach of testing exonic or hotspot regions of BRCA1/2, which might lead to missing significant numbers of splice pathogenic and intronic VUS variants. Overall, we believe that this work is a significant step towards harnessing the full benefits of NGS-based genetic testing to transform the precision oncology of patients with limited access to molecular testing resources.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Graham S.Hallisey E.Wilt G.Flanagan B.Rodriguez J.L.Peipins L.Sociodemographic disparities in access to ovarian cancer treatment Ann Cancer Epidemiol 320191010.21037/ace.2019.10.02PMC 700877432043078 · doi ↗ · pubmed ↗
- 2Wooster R.Bignell G.Lancaster J.Identification of the breast cancer susceptibility gene BRCA 2Nature 37865591995789792852441410.1038/378789 a 0 · doi ↗ · pubmed ↗
- 3Inagaki-Kawata Y.Yoshida K.Kawaguchi-Sakita N.Genetic and clinical landscape of breast cancers with germline BRCA 1/2 variants Commun Biol 312020193306755710.1038/s 42003-020-01301-9PMC 7567851 · doi ↗ · pubmed ↗
- 4Kuchenbaecker K.B.Hopper J.L.Barnes D.R.Risks of breast, ovarian, and contralateral breast cancer for BRCA 1 and BRCA 2 mutation carriers J Am Med Assoc 317232017240210.1001/jama.2017.711228632866 · doi ↗ · pubmed ↗
- 5Incorvaia L.Fanale D.Bono M.BRCA 1/2 pathogenic variants in triple-negative versus luminal-like breast cancers: genotype–phenotype correlation in a cohort of 531 patients Ther Adv Med Oncol 12202011910.1177/1758835920975326 PMC 774711433403015 · doi ↗ · pubmed ↗
- 6Bensam M.Hafez E.Awad D.M.E.S.Balbaa M.Detection of new point mutations of BRCA 1 and BRCA 2 in breast cancer patients Biochem Genet 521-2201415282387719210.1007/s 10528-013-9623-8 · doi ↗ · pubmed ↗
- 7Hussien Y.M.Gharib A.F.Ibrahim H.M.Abdel-Ghany M.E.Elsawy W.H.Analysis of BRCA 1 and BRCA 2 mutations in eastern Egyptian breast cancer patients Bull Egypt Soc Physiol Sci 3112011107116
- 8Abdel-Mohsen M.Ahmed O.El-Kerm Y.BRCA 1 gene mutations and influence of chemotherapy on autophagy and apoptotic mechanisms in Egyptian breast cancer patients Asian Pacific J Cancer Prev 17320161285129210.7314/apjcp.2016.17.3.128527039761 · doi ↗ · pubmed ↗