Quadricuspid Aortic Valve With Severe Aortic Regurgitation
Takumi Minatoya, Atsushi Hayashi, Hiroki Okamoto, Kohei Asada, Noriyuki Takashima, Tomoaki Suzuki, Yoshihisa Nakagawa

TL;DR
This paper discusses how quadricuspid aortic valves, once only detectable during surgery, can now be identified preoperatively using advanced imaging techniques.
Contribution
The paper highlights the role of modern imaging in preoperative detection and management of quadricuspid aortic valves.
Findings
Quadricuspid aortic valves can now be detected preoperatively using transthoracic echocardiography.
Further imaging with transesophageal echocardiography or CT can guide surgical strategies.
Abstract
Whenever a quadricuspid aortic valve (QAV) was present, it was historically only identified during open heart surgery. However, recent advances in transthoracic echocardiography have made it possible to detect QAV preoperatively. Further evaluation using transesophageal echocardiography or computed tomography before open surgery may help guide the surgical treatment strategy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
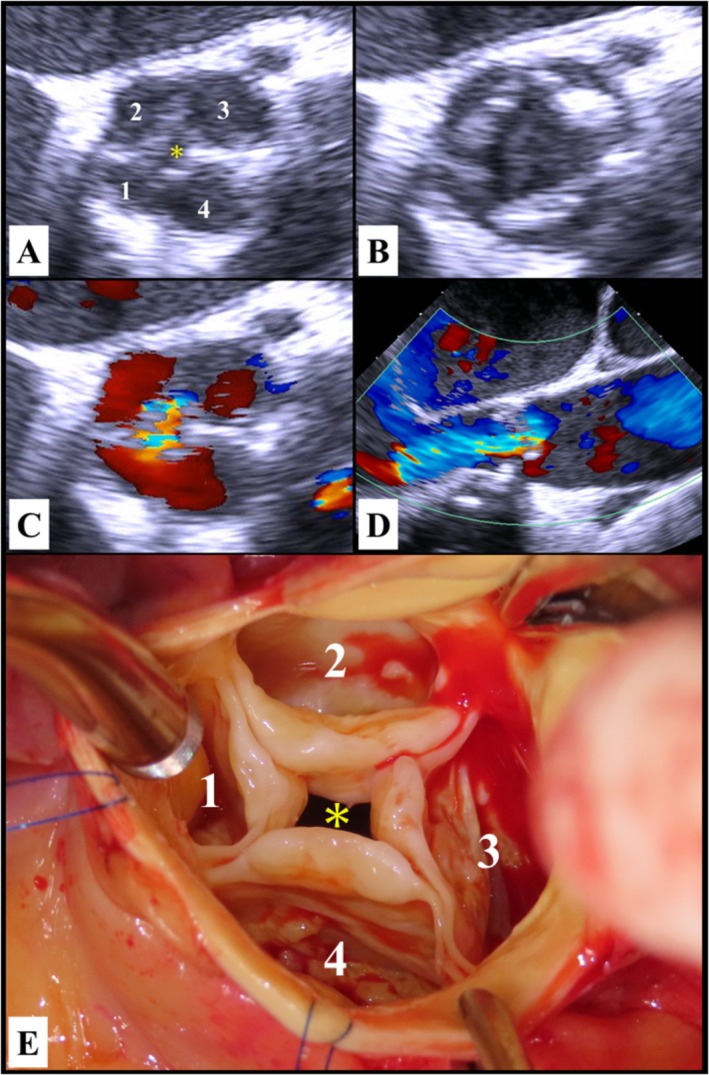 FIGURE 1
FIGURE 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Aortic Disease and Treatment Approaches · Infective Endocarditis Diagnosis and Management
Case Report
1
A 76‐year‐old man presented to the emergency department with acute dyspnea and was admitted to our hospital with a diagnosis of acute heart failure. The patient had a history of hypertension, dyslipidemia, and severe aortic regurgitation (AR) with reduced left ventricular (LV) contractility and LV enlargement, but had discontinued his outpatient visits 3 years before this admission. On physical examination, his blood pressure was 110/79 mmHg, and cardiac auscultation revealed a III/VI diastolic murmur along the left sternal border. A chest radiograph showed a cardiothoracic ratio of 73% with a butterfly shadow in both lungs. Blood tests revealed an elevated brain natriuretic peptide level (2278 pg/mL). Transthoracic echocardiography showed severe AR, LV contractile dysfunction with an LV ejection fraction of 25%, and LV dilatation with an LV end‐diastolic diameter of 63 mm. Within a few days of admission, his status improved. Due to symptomatic severe AR with the severely reduced LV function and LV enlargement, aortic valve replacement surgery was recommended.
Preoperative transesophageal echocardiography in the short‐axis view showed that the aortic valve had four leaflets (Figure 1A,B), consistent with a QAV, and a central jet of AR (Figure 1C,D). Surgical findings revealed the presence of a QAV characterized by four equal‐sized cusps (Figure 1E). This configuration was classified as type A according to the Hurwitz and Roberts classification [1, 2]. A bioprosthetic valve was implanted. He had an uneventful postoperative course.
Preoperative transesophageal echocardiography showed four leaflets in the short‐axis view of the aortic valve (A, diastolic phase; B, systolic phase). Severe central aortic regurgitation (C, short‐axis view; D, long‐axis view) resulted from a small diastolic coaptation defect (A and E, asterisk). Intraoperatively, the surgeon's view revealed a quadricuspid aortic valve (E). The four cusps were of equal size and the accessory cusp was located between the right and left cusps (A and E, 1: Right‐coronary cusp, 2: Non‐coronary cusp, 3: Left coronary cusp, 4: Accessory cusp).
Author Contributions
Takumi Minatoya: writing – original draft. Atsushi Hayashi: writing – review and editing. Hiroki Okamoto: writing – review and editing. Kohei Asada: resources. Noriyuki Takashima: resources. Tomoaki Suzuki: resources. Yoshihisa Nakagawa: supervision.
Consent
Written informed consent was obtained from the patients to publish this report in accordance with the journal's patient consent policy.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1L. E. Hurwitz and W. C. Roberts , “Quadricuspid Semilunar Valve,” American Journal of Cardiology 31 (1973): 623–626, 10.1016/0002-9149(73)90332-9.4698133 · doi ↗ · pubmed ↗
- 2M. Y. Tsang , M. M. Abudiab , N. M. Ammash , et al., “Quadricuspid Aortic Valve: Characteristics, Associated Structural Cardiovascular Abnormalities, and Clinical Outcomes,” Circulation 133 (2016): 312–319, 10.1161/CIRCULATIONAHA.115.017743.26635401 · doi ↗ · pubmed ↗