Prevention of bicalutamide-induced breast events in patients with prostate cancer: a meta-analysis of randomized controlled trials
Luca Spagnolo, Daniele Tienforti, Carolina Moretto, Camilla Tonni, Vittoria Donatelli, Alessandro Ferranti, Gennaro Puocci, Claudio Capuano, Arcangelo Barbonetti

TL;DR
This study finds that tamoxifen is most effective in preventing breast issues caused by bicalutamide in prostate cancer patients, with radiotherapy as a good alternative.
Contribution
A meta-analysis comparing the effectiveness of tamoxifen, anastrozole, and radiotherapy in preventing bicalutamide-induced breast events.
Findings
Tamoxifen reduced breast events by 82% compared to bicalutamide alone.
Radiotherapy reduced gynecomastia risk by 52% and breast pain by 34%.
Anastrozole showed no significant benefit in preventing breast events.
Abstract
This study aimed to quantitatively assess the effectiveness of tamoxifen, anastrozole, and radiotherapy in preventing bicalutamide-induced breast events—specifically gynecomastia and breast pain—in patients with prostate cancer. A systematic review and meta-analysis of randomized controlled trials (RCTs) was conducted according to PRISMA-P guidelines. A comprehensive search was performed in PubMed, Scopus, and Web of Science for English-language studies without temporal restrictions. Studies were included if they involved prostate cancer patients treated with bicalutamide receiving preventive interventions (tamoxifen, anastrozole, or radiotherapy) compared to bicalutamide alone (or bicalutamide plus placebo/sham). Data extraction focused on the incidence of gynecomastia and breast pain, and study quality was assessed using the Jadad scale. Risk ratios (RR) with 95% confidence intervals…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
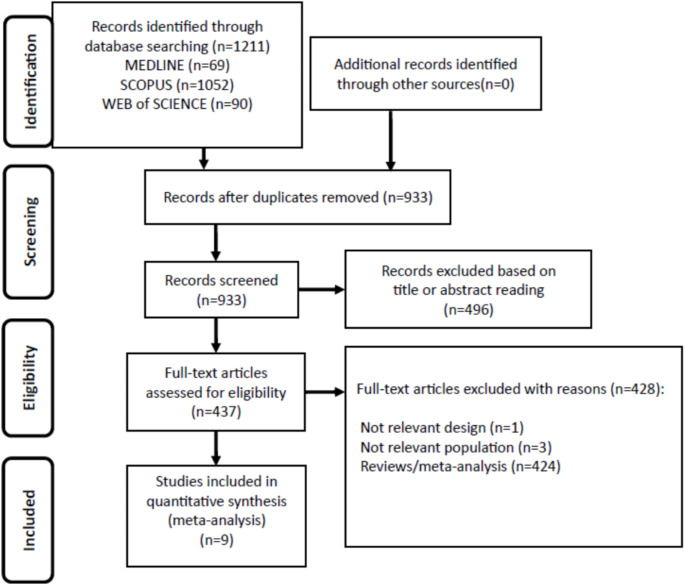 Figure 1
Figure 1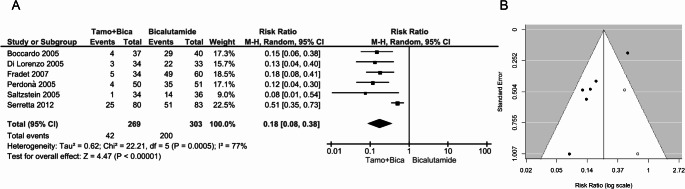 Figure 2
Figure 2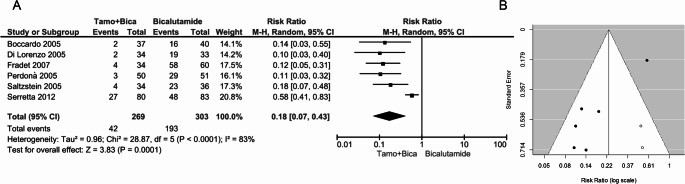 Figure 3
Figure 3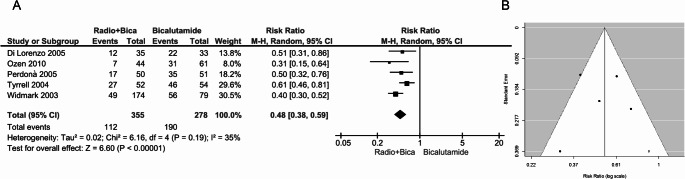 Figure 4
Figure 4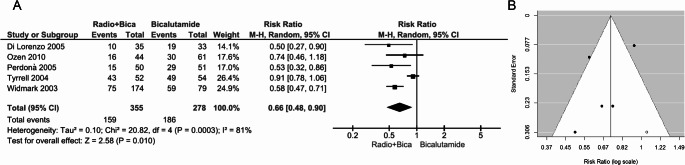 Figure 5
Figure 5- —Università degli Studi dell’Aquila
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Male Breast Health Studies · Estrogen and related hormone effects
Introduction
Prostate cancer is a multi-stage disease that exists as a continuum of several, partially overlapping stages, including localized, locally advanced, metastatic, and hormone-refractory forms [1, 2]. The common therapeutic approaches in early stages include radical prostatectomy, radiotherapy, and active monitoring [3, 4]. Bicalutamide is a potent non-steroidal antiandrogen administered at 150 mg per day. It was historically considered a treatment option for patients with locally advanced, non-metastatic (M0) prostate cancer [5–11]. However, current National Comprehensive Cancer Network (NCCN) [12] and European Society for Medical Oncology (ESMO) [13] guidelines no longer recommend it as a first-line therapy, favoring next-generation androgen receptor pathway inhibitors (ARPIs) (e.g., enzalutamide, apalutamide, darolutamide) due to their superior efficacy and safety profile. Nevertheless, the guidelines form the European Association of Urology (EAU) [14] still recognize a role for bicalutamide in certain clinical scenarios, particularly for patients who cannot tolerate next-generation ARPIs. Importantly, while enzalutamide monotherapy has been associated with a 44.9% incidence of gynaecomastia [15], bicalutamide remains a well-documented cause of breast-related side effects, including gynecomastia and breast pain [7–11]. Gynecomastia is a benign overgrowth of glandular tissue in the male breast induced by an imbalance in sex hormones: while decreasing androgen levels should inhibit breast enlargement, increased estrogen levels promote mammary glandular development [16, 17]. Gynecomastia progresses through distinct stages. In its initial phase, which may last up to two years, the condition is characterized by a “proliferative” process involving both ductal cells and fibroblastic-stromal tissue [18]. This phase is frequently accompanied by pain and breast tenderness, although gynecomastia may eventually present as an isolated symptom without pain [19]. Over time, the condition may become chronic and irreversible due to stromal hyalinization and fibrosis [20].
Bicalutamide interferes at multiple levels with the hormonal balance that regulates the proliferative state of mammary glandular tissue in males [21]. As an androgen receptor antagonist, it diminishes the antiproliferative effects of testosterone while simultaneously inducing a compensatory increase in testosterone levels that are aromatized into 17-beta-estradiol [22]. An increased estrogen/androgen ratio underlies the pathophysiology of breast complications associated with bicalutamide therapy [17, 23]. On this basis, pharmacological strategies to prevent breast enlargement aim to block the estrogen-specific stimulation of mammary tissue and/or to limit the peripheral aromatization of testosterone. Anti-estrogens, such as tamoxifen, and aromatase inhibitors, such as anastrozole, have been employed for these purposes [1, 6, 24–27]. Low-dose irradiation therapy, by reducing the responsiveness of mammary tissue to hormonal stimulation, represents another non-surgical strategy to mitigate the effects of bicalutamide on the breast [24, 28–31]. Although the literature documents the efficacy of some approaches– including tamoxifen treatment– the small sample sizes do not allow for definitive conclusions. For other strategies, such as treatment with aromatase inhibitors and radiotherapy, the evidence remains inconclusive [32].
The aim of our study is to quantitatively assess the effectiveness of tamoxifen, anastrozole, and radiotherapy in preventing bicalutamide-induced gynecomastia and breast pain in patients with prostate cancer through a systematic review and meta-analysis of randomized controlled trials (RCTs).
Materials and methods
The study was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) [33]. The study is registered in the PROSPERO (International Prospective Register of Systematic Reviews) database under the identification number CRD42023484338.
Systematic search strategy
A systematic search was performed in PubMed, Scopus, and Web of Science. The selection was restricted to studies published in English, with no temporal limits. The following search terms were used: “gynecomastia,” “breast enlargement,” “mastodynia,” “breast pain,” “breast event*,” “bicalutamide,” “antiandrogen*,” “SERM*,” “selective estrogen receptor modulator*,” “tamoxifen,” “clomiphene,” “aromatase inhibitor*,” “aromatase inhibition,” “anastrozole,” “radiotherapy,” and “breast irradiation.” Boolean AND/OR operators were applied to combine these terms appropriately.
Inclusion/exclusion criteria
The study selection proceeded in several steps. First, a comprehensive identification of articles on the topic was achieved through database searches. After duplicate removal, titles and abstracts were screened. Finally, two reviewers (D.T. and C.M.) independently assessed the full texts of the remaining articles to verify eligibility. Only studies meeting the following criteria were included: (1) RCTs; (2) studies conducted in patients with prostate cancer treated with bicalutamide; (3) studies in which patients received a preventive treatment regimen with tamoxifen, anastrozole, or radiation therapy; (4) studies that compared the preventive treatment group with a control group receiving bicalutamide alone (or bicalutamide plus placebo/sham) in terms of bicalutamide-induced breast events (gynecomastia and/or breast pain).
Data extraction
For each selected study, the following information was extracted by two authors (L.S. and D.T.): the first author’s name, publication year, the number of patients experiencing the event(s) (gynecomastia and/or breast pain) in the “bicalutamide with preventive treatment” group versus the group bicalutamide alone (or bicalutamide plus placebo/sham)”, and the total number of patients in both groups.
Quality assessment
The methodological quality of each study was evaluated using the Jadad scale [34], a validated instrument that assesses randomization, double blinding, and losses to follow-up on a scale from 0 to 5. A score of ≥ 3 was considered indicative of good methodological quality. Two authors (A.F. and G.P.) evaluated the quality of each selected study, involving a third author (A.B.) to solve any disagreement.
Statistical analysis
The efficacy of each intervention (tamoxifen, anastrozole, and radiotherapy) in preventing bicalutamide-induced adverse breast events was assessed by calculating risk ratios (RR) with 95% confidence intervals (95% CIs). Data were pooled using random-effects models even in the presence of minimal heterogeneity; a fixed-effects model was applied only when no heterogeneity was detected. Between-study heterogeneity was evaluated using Cochran’s Chi-square test (Q test) and the I² statistic, with I² ≥ 50% and/or a P value < 0.05 considered indicative of significant heterogeneity [35]. Sub-analyses were performed to explore potential sources of heterogeneity. Publication bias was examined by inspecting the symmetry of funnel plots [36]. To adjust for potential publication bias, Duval and Tweedie’s “trim-and-fill” method was applied [37], which identifies putative missing studies to rebalance the distribution and yields an adjusted pooled estimate. Analyses were conducted using RevMan (Review Manager, version 5.3) and R statistical software with the metafor package (version 3.6.3, 2020; The R Foundation for Statistical Computing, Vienna, Austria).
Results
Study selection
The online database search initially retrieved 1211 studies. After removing duplicates, 933 studies remained. Following the screening of titles and abstracts, 496 studies were excluded as not relevant. Thus, as shown in Fig. 1, after further full text evaluation, 9 studies met the inclusion criteria [1, 6, 24–30]. The main details of the eligible studies, including their methodological quality scores according to the Jadad scale, are presented in Table 1. With the exception of one RCT [30], all studies were assigned a score of ≥ 3.
Fig. 1. Flow diagram showing an overview of the study selection process
Table 1. Main characteristics of the RCTs included in the meta-analysis and their methodological quality scores according to the Jadad scaleStudyCountryInterventionsGynecomastia assessmentBreast pain assessmentFollow-up(months)Jadad scoreWidmark et al., 2003NorwayBica alone (n = 79) or with RT 12 to 15 Gy in a single fraction or 15 Gy in 3 fractions (n = 174) on a target between 4–6 cm diameterPhysical examination, self-reported, PCSS questionnairePhysical examination, self-reported, PCSS questionnaire122Tyrrell et al., 2004Sweden and UKBica with sham (n = 54) or with asingle 10 Gy RT dose (n = 52) on a 5 cm diameter circle of tissue around the nippleCallipersSelf-reported124Boccardo et al., 2005ItalyBica with Placebo (n = 40) or Tam 20 mg daily (n = 37) or Anas 1 mg daily (n = 36)Callipers orultrasoundSelf-reportedMedian: 12(range: 1 to 25)4Di Lorenzo et al., 2005ItalyBica alone (n = 33) or with Tam 10 mg daily (n = 34) or a single 12 Gy RT dose (n = 35) on a 5 cm diameter circle of tissue around the nippleCallipersSelf-reportedMedian 26(range: 13 to 35)3Perdonà et al., 2005ItalyBica alone (n = 51) or with Tam 10 mg daily (n = 50) or a single 12 Gy RT dose (n = 50) on a 5 cm diameter circle of tissue around the nippleCallipersSelf-reported123Saltzstein et al., 2005USABica with Placebo (n = 36) or Tam 20 mg daily (n = 34) or Anas 1 mg daily (n = 36)Physical examination and a questionnaireQuestionnaire95Fradet et al., 2007Canada, Finland, Norway and UKBica with Placebo (n = 60) or Tam 1 (n = 58), 2.5 (n = 45), 5 (n = 47), 10 (n = 34) or 20 mg (n = 34)CallipersSelf-reported125Ozen et al., 2010TurkeyBica alone (n = 61) or with RT 12 Gy dosein 2 fractions of 6 Gy each onconsecutive days (n = 44) on a 5 cm diameter circle of tissue around the nippleCallipersSelf-reported123Serretta et al., 2012ItalyBica alone (n = 83) or withTam 10 mg daily (n = 80)Self-administeredvisual analogue scaleSelf-administeredvisual analogue scaleMedian 15(range: 12 to 36)3A Jadad score ≥ 3 documented a good methodological quality. Anas, anastrozole; Bica, bicalutamide; Gy, Gray; PCSS, Prostate Cancer Symptom Scale; Tam, tamoxifen; RT, radiotherapy
Tamoxifen in prevention of bicalutamide-induced gynecomastia
Six RCTs provided data on 572 patients treated with bicalutamide, of whom 269 also received tamoxifen. As shown in Fig. 2A, the pooled estimate revealed an 82% risk reduction of gynecomastia in the tamoxifen-treated group (RR: 0.18, 95% CI: 0.08–0.38, p < 0.00001). However, significant between-study heterogeneity was observed (I² = 77%, p = 0.0005). The skewed funnel plot suggested publication bias, which was confirmed by the trim-and-fill test that identified two putative missing studies (Fig. 2B). Nevertheless, publication bias did not fully explain the heterogeneity, as the overall estimate recalculated after the inclusion of the two putative missing studies still revealed significant heterogeneity (adjusted pooled RR: 0.23, 95% CI: 0.13–0.39; I² = 60%, p = 0.004). In contrast, when the analysis was restricted to the three double-blind, randomized, placebo-controlled trials [6, 25, 26], the overall estimate remained substantially unchanged (RR: 0.15, 95% CI: 0.08–0.27, p < 0.00001 with fixed-effects model) and heterogeneity disappeared (I² = 0%, p = 0.72).
Fig. 2(A) Forest plot and (B) funnel plot depicting the effect of tamoxifen in preventing bicalutamide-induced gynecomastia. In panel A, the diamond represents the overall estimate (with the width indicating the 95% CI), and the boxes represent the weight of individual studies in the pooled result. In panel B, the trim-and-fill test identifies two putative missing studies (white circles) on the right side of the distribution
Tamoxifen in prevention of bicalutamide-induced breast pain
As shown in Fig. 3A, tamoxifen treatment demonstrated significant efficacy in preventing bicalutamide-induced breast pain (RR: 0.18, 95% CI: 0.07–0.43, p = 0.00001). However, significant between-study heterogeneity was registered (I² = 83%, p < 0.0001). The skewed funnel plot indicated publication bias, which was confirmed by the trim-and-fill test that identified two putative missing studies (Fig. 3B). Nonetheless, publication bias did not fully account for the heterogeneity, as the overall estimate recalculated after the inclusion of the putative missing studies still showed significant heterogeneity (adjusted pooled RR: 0.23, 95% CI: 0.13-0.42; I² =65%, *p=*0.0009). On the contrary, when the analysis was restricted to the three double-blind, randomized, placebo-controlled trials [6, 25, 26], the overall estimate remained largely unchanged (RR: 0.15, 95% CI: 0.08-0.27, p < 0.00001 with fixed-effects model) with no between-study heterogeneity (I² = 0%, p = 0.82).
Fig. 3(A) Forest plot and (B) funnel plot depicting the effect of tamoxifen in preventing bicalutamide-induced breast pain. In panel A, the diamond represents the overall estimate (with the width indicating the 95% CI), and the boxes represent the weight of individual studies in the pooled result. In panel B, the trim-and-fill test identifies two putative missing studies (white circles) on the right side of the distribution
Radiotherapy in prevention of bicalutamide-induced gynecomastia
Five RCTs provided data on 633 patients treated with bicalutamide, of whom 355 also underwent radiotherapy. Notably, only the RCT by Tyrrell [29] was a double-blind, sham-controlled trial. As shown in Fig. 4A, the pooled estimate indicated a 52% risk reduction of gynecomastia in the radiotherapy-treated group (RR: 0.48, 95% CI: 0.38–0.59, p < 0.00001) with non-significant heterogeneity (I² = 35%, p = 0.19). The trim-and-fill test identified one putative missing study (Fig. 4B), the inclusion of which, did not affect the overall estimate (adjusted pooled RR: 0.53, 95%CI: 0.41-0.86, p<0.0001).
Fig. 4(A) Forest plot and (B) funnel plot depicting the effect of radiotherapy in preventing bicalutamide-induced gynecomastia. The diamond represents the overall estimate (with the width indicating the 95% CI), and the boxes represent the weight of individual studies in the pooled result. In panel B, the trim-and-fill test identifies one putative missing study (white circle) on the right side of the distribution
Radiotherapy in prevention of bicalutamide-induced breast pain
As shown in Fig. 5A, the overall efficacy of radiotherapy in preventing bicalutamide-induced breast pain reached statistical significance (RR: 0.66, 95% CI: 0.48–0.90, p = 0.01). However, significant between-study heterogeneity was observed (I² = 81%, p = 0.0003). The skewed funnel plot indicated publication bias, which was confirmed by the trim-and-fill test that identified one putative missing study (Fig. 5B). Nevertheless, publication bias did not completely account for the heterogeneity, as the overall estimate recalculated after adjustment for the putative missing study still revealed significant heterogeneity (adjusted pooled RR: 0.73, 95% CI: 0.58–0.92; I² = 63.6%, p = 0.004).
Fig. 5(A) Forest plot and (B) funnel plot depicting the effect of radiotherapy in preventing bicalutamide-induced breast pain. In panel A, the diamond represents the overall estimate (with the width indicating the 95% CI), and the boxes represent the weight of individual studies in the pooled result. In panel B, the trim-and-fill test identifies one putative missing study (white circle) on the right side of the distribution
Anastrozole in prevention of bicalutamide-induced breast events
The potential usefulness of anastrozole in preventing bicalutamide-induced breast events was evaluated in only two RCTs, both of which were double-blind, placebo-controlled. These studies provided data on a total of 148 patients treated with bicalutamide, of whom 72 also received anastrozole. The pooled estimates demonstrated that anastrozole was ineffective in preventing both bicalutamide-induced gynecomastia (RR: 0.75, 95% CI: 0.54–1.04, p = 0.08; I² = 0%, p = 0.55) and breast pain (RR: 0.88, 95% CI: 0.64–1.21, p = 0.08; I² = 4%, p = 0.31).
Discussion
Although bicalutamide has historically played a role in the management of prostate cancer, its clinical relevance has declined with the advent of more effective androgen receptor inhibitors. While NCCN [12] and ESMO guidelines [38] no longer recommend it as a preferred option, EAU guidelines [39] still consider it a viable alternative in specific cases. However, a key concern associated with bicalutamide use is its high incidence of gynaecomastia [7–11], which can significantly impact patient adherence and quality of life. This adverse effect primarily results from its antagonistic action on androgen receptors in breast tissue, leading to an imbalance in the estrogen–androgen ratio and, consequently, to the stimulation of breast tissue growth [10]. Unlike recent studies that primarily focus on enzalutamide-induced breast-related side effects, our study directly addresses the management of bicalutamide-induced gynaecomastia, which remains an underexplored yet clinically relevant issue. Recently, Tsuboi et al. [40] provided a broad analysis of breast-related side effects in antiandrogen therapy and assessed the prevention of gynecomastia and breast pain in patients undergoing antiandrogen therapy for prostate cancer. Nevertheless, their meta-analysis did evaluate aromatase inhibitors as a preventive or therapeutic strategy. By addressing this gap, our study offers a more comprehensive and targeted approach to managing this well-recognized adverse effect.
The results of this meta-analysis highlight the efficacy of specific strategies—such as tamoxifen and radiotherapy—while demonstrating the limited utility of anastrozole in mitigating these adverse events. Nevertheless, the small number of available trials on the efficacy of anastrozole prevents definitive conclusions.
Although tamoxifen has not yet been approved by the Food and Drug Administration (FDA) for this indication, our meta-analysis demonstrated its robust efficacy in preventing both gynecomastia and breast pain associated with bicalutamide therapy. Pooled estimates from six RCTs indicated that tamoxifen reduced the risk of breast events by 82%. Despite significant heterogeneity across studies—particularly in the analysis of gynecomastia prevention—sensitivity analyses restricted to double-blind, placebo-controlled RCTs yielded consistent results and eliminated heterogeneity. These findings are consistent with tamoxifen’s established role as a selective estrogen receptor modulator (SERM), which competes with estrogen for receptor binding in mammary tissue and effectively mitigates estrogenic stimulation [6]. Notably, its ability to block estrogen receptors in the breast while acting as an estrogen agonist in other tissues (such as bone) provides a therapeutic advantage in managing gynecomastia without adversely affecting other estrogen-dependent tissues [41]. Although the asymmetry observed in the funnel plots of tamoxifen analyses suggested the presence of publication bias, adjusted RRs using the trim-and-fill method confirmed the robustness of the results.
Radiotherapy, particularly low-dose breast irradiation, is another modality employed to prevent or manage gynecomastia. This approach induces fibrosis and tissue atrophy, thereby limiting the proliferative effects of estrogen on breast tissue [29, 42]. In our analysis, radiotherapy emerged as an effective strategy, reducing the risk of gynecomastia by 52% and breast pain by 34%. Unlike tamoxifen, the effectiveness of radiotherapy in preventing gynecomastia was associated with minimal heterogeneity—likely due to uniform treatment protocols across studies. However, its efficacy in preventing breast pain was less pronounced and accompanied by significant heterogeneity, which persisted even after adjusting for publication bias. These findings suggest that radiotherapy may not uniformly address all aspects of bicalutamide-induced breast events, particularly subjective symptoms such as pain [30].
Anastrozole, an aromatase inhibitor, acts by inhibiting the conversion of androgens to estrogens. Given that bicalutamide indirectly increases estrogen levels by reducing androgenic feedback on the hypothalamic–pituitary–gonadal axis, anastrozole could theoretically reduce estrogen production and attenuate its stimulatory effects on breast tissue [43]. In contrast to tamoxifen and radiotherapy, however, our meta-analysis did not demonstrate significant efficacy for anastrozole in preventing either gynecomastia or breast pain. This lack of efficacy, arising from the results of only two RCTs, may reflect insufficient suppression of estrogen levels needed to counteract the hormonal imbalances induced by bicalutamide, which aligns with the limited and inconsistent evidence available for aromatase inhibitors in this setting [6, 25].
Our findings have several clinical implications. First, tamoxifen should be considered the first-line preventive treatment for bicalutamide-induced breast events given its superior efficacy and consistent results across trials. Radiotherapy represents a viable alternative, particularly for patients who are intolerant to tamoxifen or in cases where preventing gynecomastia is prioritized over managing breast pain. Conversely, the lack of benefit observed with anastrozole suggests that its routine use in this setting is unwarranted. Furthermore, while both tamoxifen and radiotherapy demonstrated efficacy, the heterogeneity observed in some analyses highlights the importance of tailoring preventive strategies to individual patient profiles. Factors such as baseline hormonal levels, comorbidities, breast tissue responsiveness, and patient preferences should guide treatment decisions. Finally, the choice between tamoxifen and radiotherapy should also take into account potential side effects. Systemic effects of tamoxifen may include hot flashes [24, 25], an increased risk of cardiovascular events [27], which may be particularly relevant in older patients with cardiovascular comorbidities. On the other hand, prophylactic radiotherapy is a localized intervention, generally well tolerated, but associated with potential short-term skin irritation, nipple tenderness, mild discomfort, and pruritus at the treatment site [1, 24, 28, 29].
This study also has limitations. Although all RCTs on tamoxifen consistently indicate its efficacy in preventing both bicalutamide-induced gynecomastia and breast pain, the overall quality of the evidence is limited by the low number of RCTs, small sample sizes, and the relatively wide confidence intervals of documented outcomes. These factors limit the statistical power of the overall effect estimates. Additionally, potential attrition bias exists, as not all RCTs adequately reported dropout rates. Significant heterogeneity was observed among the RCTs—a heterogeneity that was not explained by publication bias but was eliminated when the three non-double-blind, placebo-controlled trials were excluded. This heterogeneity likely also reflects differences in tamoxifen dosing (10 mg versus 20 mg daily) and treatment duration (ranging from 3 to 12 months). In the absence of comparative studies, no definitive recommendation can be made regarding the optimal dosage. In an open multicenter randomized phase 3 trial [44], daily treatment with tamoxifen 20 mg was superior to a regimen involving tamoxifen 20 mg weekly (after an initial 8-week period of daily therapy) in preventing bicalutamide-induced gynecomastia and breast pain. Regarding anastrozole, the two available RCTs [6, 26] consistently reported its ineffectiveness in preventing bicalutamide-induced breast events. Overall, the small sample sizes of the included trials limit the generalizability of our findings. In contrast, radiotherapy appears to offer some prophylactic efficacy, although the availability of only one sham-controlled RCT [29], variations in doses (10 to 15 Gy), treatment modalities, and the significant heterogeneity observed in the analysis of breast pain downgrades the overall quality of the evidence.
Future studies should aim to evaluate the comparative efficacy of these preventive strategies in larger populations and explore potential combination therapies to enhance outcomes. Moreover, the long-term safety profiles of these interventions—particularly tamoxifen and radiotherapy—warrant further investigation to ensure their broader applicability in clinical practice.
In conclusion, this meta-analysis highlights tamoxifen and radiotherapy as effective strategies for preventing bicalutamide-induced breast events, with tamoxifen demonstrating superior efficacy in both gynecomastia and breast pain prevention. On the contrary, although further RCTs are warranted, anastrozole does not appear to offer significant benefits in this context. These findings underscore the need for individualized approaches to managing bicalutamide-induced adverse effects and call for further high-quality research to refine treatment recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perdonà S, Autorino R, De Placido S, D’Armiento M, Gallo A, Damiano R, Pingitore D, Gallo L, De Sio M, Bianco AR, Di Lorenzo G (2005) Efficacy of tamoxifen and radiotherapy for prevention and treatment of gynaecomastia and breast pain caused by bicalutamide in prostate cancer: a randomised controlled trial. Lancet Oncol.;6(5):295–300. 10.1016/S 1470-2045(05)70103-0. PMID: 1586337710.1016/S 1470-2045(05)70103-015863377 · doi ↗ · pubmed ↗
- 2Hamdy FC, Donovan JL, Lane JA, Metcalfe C, Davis M, Turner EL, Martin RM, Young GJ, Walsh EI, Bryant RJ, Bollina P, Doble A, Doherty A, Gillatt D, Gnanapragasam V, Hughes O, Kockelbergh R, Kynaston H, Paul A, Paez E, Powell P, Rosario DJ, Rowe E, Mason M, Catto JWF, Peters TJ, Oxley J, Williams NJ, Staffurth J, Neal DE (2023) Protec T Study Group. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med.;388(17):1547–1558. 10.1056/NEJ Moa 2214122. Epub 2023 · doi ↗ · pubmed ↗
- 3Iversen P (2002) Antiandrogen monotherapy: indications and results. Urology.;60(3 Suppl 1):64–71. 10.1016/s 0090-4295(02)01576-5. PMID: 1223105310.1016/s 0090-4295(02)01576-512231053 · doi ↗ · pubmed ↗
- 4Boccardo F, Rubagotti A, Battaglia M, Di Tonno P, Selvaggi FP, Conti G, Comeri G, Bertaccini A, Martorana G, Galassi P, Zattoni F, Macchiarella A, Siragusa A, Muscas G, Durand F, Potenzoni D, Manganelli A, Ferraris V, Montefiore F (2005) Evaluation of tamoxifen and anastrozole in the prevention of gynecomastia and breast pain induced by bicalutamide monotherapy of prostate cancer. J Clin Oncol.;23(4):808– 15. 10.1200/JCO.2005.12.013. PMID: 1568152510.1200/JCO.2005.12.01315681525 · doi ↗ · pubmed ↗
- 5See W, Iversen P, Wirth M, Mc Leod D, Garside L, Morris T (2003) Immediate treatment with bicalutamide 150 mg as adjuvant therapy significantly reduces the risk of PSA progression in early prostate cancer. Eur Urol.;44(5):512-7; discussion 517-8. 10.1016/s 0302-2838(03)00366-x. PMID: 1457274710.1016/s 0302-2838(03)00366-x 14572747 · doi ↗ · pubmed ↗
- 6Wirth MP, See WA, Mc Leod DG, Iversen P, Morris T, Carroll K (2004) Casodex Early Prostate Cancer Trialists’ Group. Bicalutamide 150 mg in addition to standard care in patients with localized or locally advanced prostate cancer: results from the second analysis of the early prostate cancer program at median followup of 5.4 years. J Urol.;172(5 Pt 1):1865-70. 10.1097/01.ju.0000140159.94703.80. PMID: 1554074010.1097/01.ju.0000140159.94703.8015540740 · doi ↗ · pubmed ↗
- 7See WA, Wirth MP, Mc Leod DG, Iversen P, Klimberg I, Gleason D, Chodak G, Montie J, Tyrrell C, Wallace DM, Delaere KP, Vaage S, Tammela TL, Lukkarinen O, Persson BE, Carroll K, Kolvenbag GJ, Casodex Early Prostate Cancer Trialist Group (2002). Bicalutamide as immediate therapy either alone or as adjuvant to standard care of patients with localized or locally advanced prostate cancer: first analysis of the early prostate cancer program. J Urol.;168(2):429– 35. Erratum in: J Urol 2002;168(6):2558. · pubmed ↗
- 8Iversen P, Mc Leod DG, See WA, Morris T, Armstrong J, Wirth MP (2010) Casodex Early Prostate Cancer Trialists’ Group. Antiandrogen monotherapy in patients with localized or locally advanced prostate cancer: final results from the bicalutamide Early Prostate Cancer programme at a median follow-up of 9.7 years. BJU Int.;105(8):1074-81. 10.1111/j.1464-410X.2010.09319.x. PMID: 2212921410.1111/j.1464-410X.2010.09319.x 22129214 · doi ↗ · pubmed ↗