Dilated thoracoabdominal and epigastric veins in a hemodialysis patient with SVC occlusion: case report and literature review
Yanlin Zhou, Bo Tu, Ziming Wan

TL;DR
A hemodialysis patient with complete blockage of the superior vena cava was managed without surgery, showing that conservative treatment can be effective.
Contribution
The study presents a rare case of successful conservative management of complete SVC occlusion in hemodialysis patients.
Findings
The patient's existing arteriovenous fistula remained functional for five years without intervention.
Collateral veins were sufficient for hemodialysis access despite complete SVC occlusion.
Conservative management was chosen over interventional or surgical options based on patient evaluation.
Abstract
For several reasons, the incidence of superior vena cava(SVC) obstruction continues to rise, as a serious complication of hemodialysis(HD) access, and is becoming a major cause of access depletion. It is also the most difficult challenge for vascular access workers. Here we present the case of a HD patient with complete SVC occlusion, and why no intervention was made. A 50-year-old man on maintenance HD was admitted for markedly dilated thoracoabdominal wall veins and superficial epigastric veins. Digital subtraction angiography(DSA) revealed a complete occlusion of the SVC. Treatment options include interventional therapy, closing the arteriovenous fistula(AVF) to reduce venous pressure and creating a new lower extremity arteriovenous(AV) access, or open surgery. The patient's venous hypertension syndrome and AV access function were carefully evaluated, leading to a decision for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
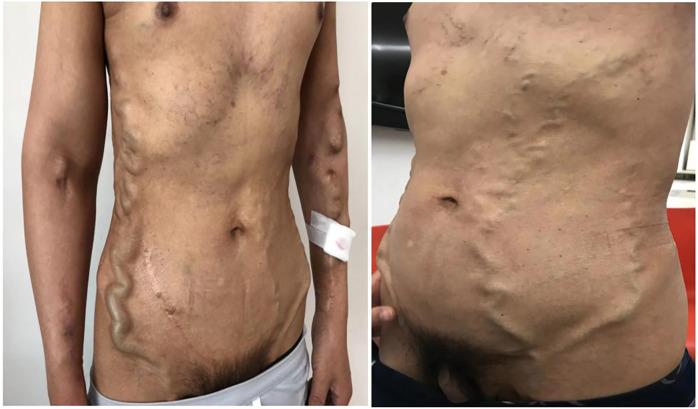 Figure 1
Figure 1 Figure 2
Figure 2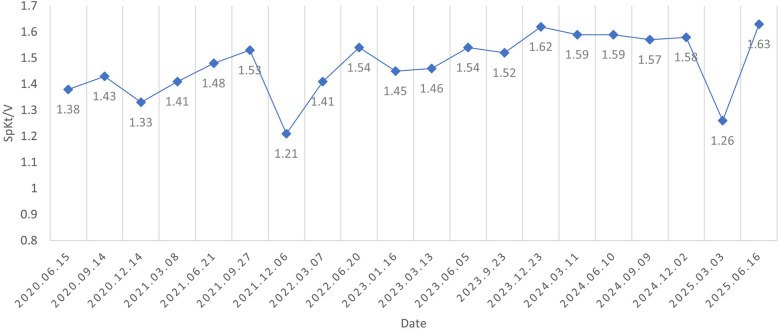 Figure 3
Figure 3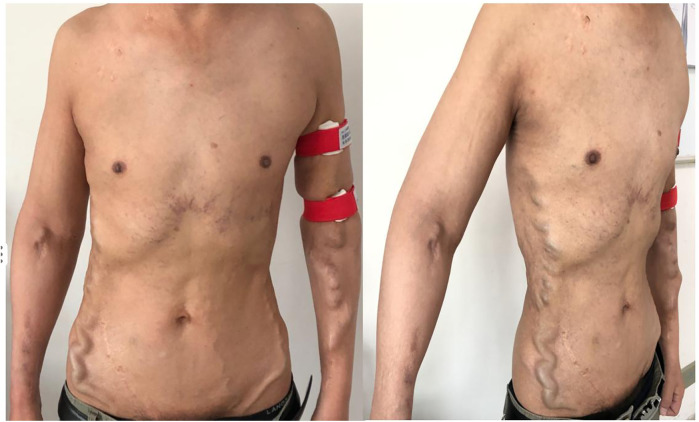 Figure 4
Figure 4| Year | Vascular access |
|---|---|
| 1994–1995 | Direct puncture of the radial artery and cephalic vein, and a right forearm AVF was established, then he continuted HD with mature AVF. |
| 2007–2011 | He continued dialysis with normal function of the right forearm AVF. |
| 2011 | The right forearm AVF was occluded, then the right elbow AVF was reconstructed and subsequently occluded. |
| 2011–2014 | A semi-permanent catheter was placed in the right internal jugular vein. |
| 2014–2015 | The blood flow in the right internal jugular vein semi-permanent catheter remained poor despite repeated administration of urokinase thrombolysis and replacement with a semi-permanent catheter. |
| 2015-until now | A left forearm AVF was successfully established and matured for use in the HD unit until now, after which the right internal jugular vein semi-permanent catheter was removed. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Vascular Procedures and Complications · Vascular anomalies and interventions
Introduction
The SVC is the largest vein, conveying blood from the head, neck, arm, and chest to the right atrium. Partial or complete obstruction the SVC is observed most frequently in lung cancer and lymphoma. With the increase in non-malignant diseases, dialysis catheters now account for about 5% of SVC obstruction (1). SVC stenosis occurs in approximately 9.4% of chronic HD patients carrying a tunneled cuffed catheter (2).
Two primary effects of SVC obstruction on maintenance HD patients are observed (3, 4). The first is venous hypertension syndrome, manifesting with limb swelling or pain, cutaneous congestion, pigmentation, or even ulceration, and open superficial chest wall veins. If the SVC lesions are serious, facial edema, head and neck distention, pleural effusion, and chylothorax may be observed. Another manifestation is access dysfunction, including decline of HD adequacy, increase of venous pressure during HD, prolonged hemostasis after needle removal from AVF, continuous progress of fistula tumor-like dilatation, and repeated thrombosis in the fistula.
Patients with HD have fewer symptoms of SVC obstruction compared with cancer patients (5), perhaps because HD patients may have a longer sub-clinical or chronic process leading to SVC occlusion, providing time for collateral circulation development (6). Here we report the case of a 50-year-old man receiving HD who was admitted for markedly dilated thoracoabdominal wall and superficial epigastric veins, and discuss the therapeutic strategy used.
Case report
A 50-year-old man maintained with HD was admitted for markedly dilated thoracoabdominal wall and superficial epigastric veins (Figure 1), with notable machinery murmur and tremor. He had previously been diagnosed with uremia in 1994, and a right forearm AVF was established for HD access. He received kidney transplantation in 1995, but the renal allograft failed in 2007, necessitating further dialysis. He had a semi-permanent catheter placed in the right internal jugular vein from 2011 to 2014 following an occluded right forearm and right elbow AVF. A left forearm AVF was established in 2015 and used for HD access until the present illness. The patient's complete vascular access history was presented in Table 1.
The patient presented markedly dilated thoracoabdominal wall and superficial epigastric veins.
At presentation, vital signs were within normal limits, and there was no swelling or pain in the extremities, neck, or head. Cutaneous examination revealed no congestion or ulceration, infection, nonhealing wounds, or incisions. He also reported no symptoms of the respiratory (hoarse voice, dyspnea) or neurological (visual or auditory disturbances, cognitive disabilities) systems. Blood cell count and liver function were normal. Abdomen ultrasound did not identify cirrhosis, splenomegaly, or portal vein thrombosis. Thoracic computed tomography showed no abnormalities of lung or mediastinum and no pleural effusion. Echocardiography showed no abnormal cardiac structure or function. DSA revealed a complete occlusion of the SVC (Figure 2) and a markedly dilated azygos vein. Vascular access function was further assessed, and color Doppler ultrasound of the AVF identified no fistula stenosis. During multiple dialysis sessions, no increased venous pressure was observed, and there was no prolonged hemostasis after HD. Dialysis adequacy was measured by single pool Kt/V(SpKt/V). The calculated SpKt/V was >1.2. Based on these observations, the patient was determined to have a complete SVC occlusion with markedly dilated thoracoabdominal wall and superficial epigastric veins, but no other venous hypertension symptoms and signs, and no evidence of access dysfunction. After thoroughly discussing the treatment options and associated risks with the patient, a conservative management approach was opted without immediate intervention, but following him closely. Every month, we recorded the appearance, diameter, and size of the lateral branches. We carefully examined whether the patient developed any new related symptoms and signs of SVC occlusion. Every three months, SpKt/V was used to evaluate HD adequacy, and the AVF was monitored by ultrasound.
DSA revealed a complete occlusion of the SVC.
After five years of follow-up, HD sufficiency was evaluated every 3 months. SpKt/V remained acceptable; we here present 5 years of data (Figure 3). His left forearm AVF continues to function well. Both the AVF and compensated superficial epigastric veins could be punctured for HD access. Moreover, the dilated thoracoabdominal wall veins and superficial epigastric veins remained unchanged (Figure 4). No new symptoms or signs of SVC obstruction or serious complications, including gastrointestinal and intracranial disease, developed. We continue to follow him conservatively.
SpKt/V was assessed every three months and remained above 1.2 throughout the five-year follow-up period.
The appearance of collateral brancheswas comparable to that observed five years ago.
Discussion
Most HD patients have only mild or no symptoms, and the central veins are not routinely imaged. The incidence of CVS/obstruction in publications ranged from 3% to 60% (7), but the incidence of complete SVC obstruction is very low. Non-tunneling catheter use, subclavian vein or left jugular vein access, repeated catheterization, and prolonged indwelling time all increase the risk of CVS/occlusion (8). The patient's SVC obstruction was related to the long indwelling time of the semi-permanent catheter in the right internal jugular vein.
It is vital to choose an appropriate therapeutic schedule for a patient with SVC obstruction. Treatment options (9) for SVC obstruction include interventional therapy, closing the AVF to reduce the venous pressure of compensatory vessels with the need to create a new, lower extremity AV access, and open surgery. Due to the numerous underlying complications in HD patients, the difficulty and risk of anesthesia with surgical procedures are very high. Endovascular therapy, including percutaneous transluminal angioplasty (PTA) or PTA with stenting, is currently the preferred treatment for SVC occlusions because it is minimally invasive (10). Surgical operations should be considered secondary and are only used when endovascular therapy has failed. These interventions succeed in opening the lesion in 40%–80% of cases. However, primary patency with PTA or PTA with stenting for CVS/occlusions is very poor, about 82.3% and 88.9% at one month, 57.1% and 67.8% at 6 months, with 1-year rates of 38.9% and 53.8%, 2-year rates of 29.4% and 39.4%, respectively (11). Zhao YL et al. (12) reported that the overall 2-year vascular access patency rate following PTA with stenting for SVC stenosis in HD patients was 33.2%. Moreover, SVC obstruction in HD patients often includes thrombosis, fibroplasia, calcification, and even long-segment occlusion, and a standard wire may not be able to cross the lesion. More aggressive techniques, such as sharp recanalization and radiofrequency guidewire, may be required to transverse the blockage (7). The most serious complications that can occur during central venous recanalization include the perforation of large veins, leading to massive hemorrhage in the chest or pericardial space, pericardial tamponade, acute heart failure, and pneumothorax (13). If endovascular therapy for SVC obstruction is successful, venous hypertension is reduced and the degree of collateral branches is visibly decreased. However, opening a completely obstructed SVC is difficult and high-risk, and repeated intervention due to low patency may be required.
Endovascular treatment for asymptomatic CVS can cause more rapid progression to symptomatic CVS/occlusion (14). The 2019 update to the KDOQI Clinical Practice Guideline for Vascular Access (15) recommended that CVS/occlusion does not require intervention in asymptomatic or mildly symptomatic patients with working HD access. This was the case for our patient with very severe, complete SVC occlusion and excellent collateral compensation without swelling, pain, respiratory or neurologic symptoms, or access dysfunction. Whether to perform an intervention warrants careful evaluation. The esophageal varices are observed commonly in HD patients with SVC obstruction. About 8% of patients with these varices may have upper gastrointestinal bleeds, and some can experience major hemorrhage (5, 16). We recommended that this patient undergo gastroscopy to evaluate the presence of esophageal varices, which was at risk of future massive gastrointestinal bleeding. Unfortunately, our patient refused gastroscopy. Intracranial hypertension can present with non-specific signs and symptoms that are not easily detected. Cases have been reported of CVS/occlusion in HD patients leading to severe neurological diseases, including idiopathic perimesencephalic subarachnoid hemorrhage, cerebral infarction, venous congestive encephalopathy, epilepsy, and syncope (17). Rupture and bleeding of lateral branches, as well as thrombosis, pose serious risks to the patient and may potentially endanger his life.
Conservative treatment was selected after communicating treatment options to the patient, given the potential and serious risks for the patient. Venous hypertension remains a risk, so clinical symptoms and signs must be closely observed, and access function regularly monitored. Gastroscopy and neuroimaging should be performed to further evaluation upon patient consent.The patient was followed up at regular intervals of one to three months throughout the five-year follow-up period and remains clinically stable. Conservative treatment appears to have been beneficial for this patient. However, further clinical studies are needed to confirm this observation. The natural history and underlying mechanisms of interaction between CVS/obstruction and collateral circulation merit further study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Straka C Ying J Kong FM Willey CD Kaminski J Kim DWN. Review of evolving etiologies, implications and treatment strategies for the superior vena cava syndrome. Springerplus. (2016) 29(5):229–42. 10.1186/s 40064-016-1900-7PMC 477167227026923 · doi ↗ · pubmed ↗
- 2Labriola L Seront B Crott R Borceux P Hammer F Jadoul M. Superior vena cava stenosis in haemodialysis patients with a tunnelled cuffed catheter: prevalence and risk factors. Nephrol Dial Transplant. (2018) 33(12):2227–33. 10.1093/ndt/gfy 15029893920 · doi ↗ · pubmed ↗
- 3Echefu G Stowe I Lukan A Sharma G Basu-Ray I Guidry L Central vein stenosis in hemodialysis vascular access: clinical manifestations and contemporary management strategies. Front Nephrol. (2023) 3:1280666. 10.3389/fneph.2023.128066638022724 PMC 10664753 · doi ↗ · pubmed ↗
- 4Kitrou P Katsanos K Karnabatidis D. Management of central venous stenoses and occlusions. Cardiovasc Intervent Radiol. (2023) 46(9):1182–91. 10.1007/s 00270-023-03461-737460644 PMC 10471665 · doi ↗ · pubmed ↗
- 5Siegel Y Kuker R. Superior vena Cava obstruction in hemodialysis patients: symptoms, clinical presentation and outcomes compared to other etiologies. Ther Apher Dial. (2016) 20(4):390–3. 10.1111/1744-9987.1239526991314 · doi ↗ · pubmed ↗
- 6Kapur S Paik E Rezaei A Vu DN. Where there is blood, there is a way: unusual collateral vessels in superior and inferior vena cava obstruction. Radiographics. (2010) 30(1):67–78. 10.1148/rg.30109572420083586 · doi ↗ · pubmed ↗
- 7Tabriz DM Arslan B. Management of central venous stenosis and occlusion in dialysis patients. Semin Intervent Radiol. (2022) 39(1):51–5. 10.1055/s-0041-174215235210733 PMC 8856783 · doi ↗ · pubmed ↗
- 8Toomay S Rectenwald J Vazquez MA. Central venous stenosis in hemodialysis patients. Semin Dial. (2016) 29(3):201–3. 10.1111/sdi.1247826926841 · doi ↗ · pubmed ↗