Reliability of disc diffusion testing and molecular epidemiology of penicillin-susceptible Staphylococcus aureus bacteraemia
Pernilla Kihlberg, Thor Bech Johannesen, Marc Stegger, Sara Cajander, Bo Söderquist

TL;DR
This study confirms the reliability of a common test for penicillin resistance in Staphylococcus aureus and finds high rates of penicillin-susceptible strains in blood infections.
Contribution
Validates the EUCAST disc diffusion method for penicillin resistance and provides new insights into the genetic diversity of PSSA strains.
Findings
Phenotypic susceptibility to penicillin strongly correlates with the absence of the blaZ gene.
PSSA accounted for 35.1% of bacteraemic isolates, emphasizing the need for susceptibility testing.
PSSA isolates showed high genetic diversity, with CC5 and CC45 being dominant lineages.
Abstract
Recent studies have reported an increasing prevalence of penicillin-susceptible Staphylococcus aureus (PSSA) worldwide. The reliability of disc diffusion testing for detecting penicillin-resistance has been questioned, and the molecular epidemiology of PSSA has not been studied to the same extent as that of MRSA strains. To investigate the reliability of the disc diffusion method for detecting penicillin-resistance in S. aureus, and to examine the prevalence and molecular epidemiology of PSSA in bloodstream infections. A total of 258 bacteraemic isolates obtained from one geographic region in Sweden during 2018–2019 were analysed using the disc diffusion test to detect penicillin-resistance, and genome sequenced to examine the prevalence of the blaZ gene and the molecular epidemiology of PSSA. Phenotypic susceptibility to penicillin correlated strongly with the absence of the blaZ…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
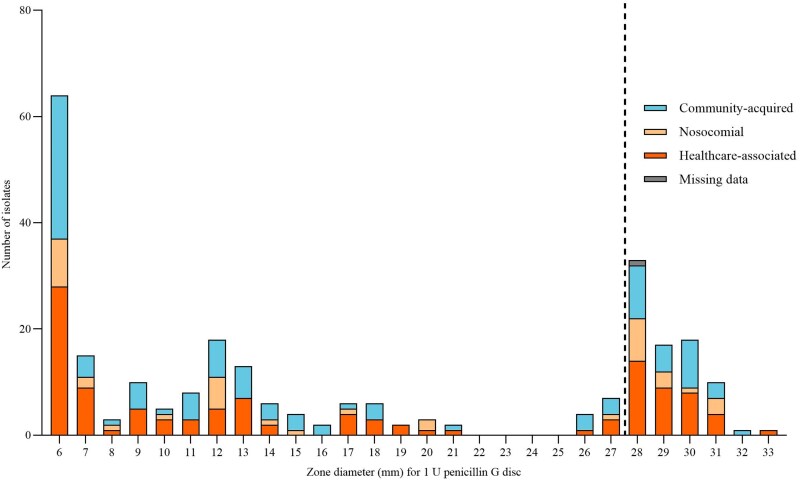 Figure 1
Figure 1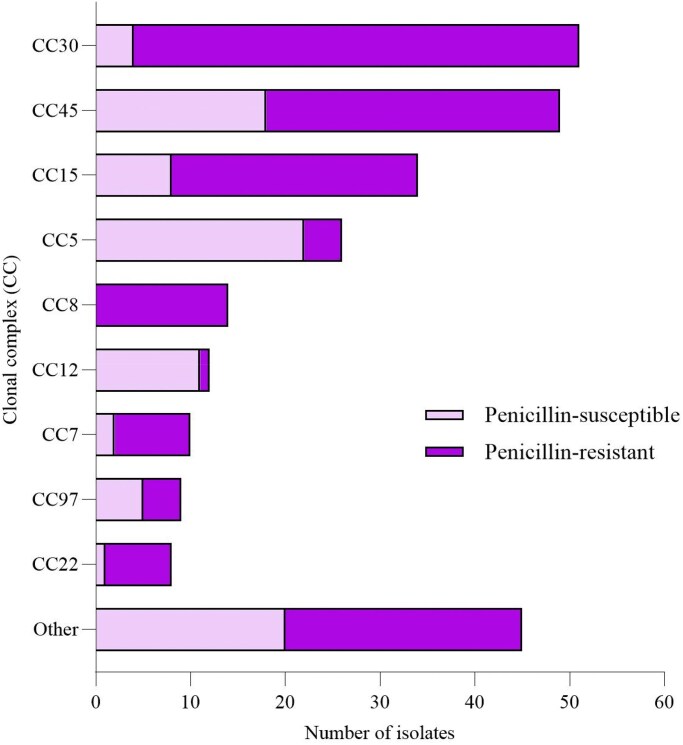 Figure 2
Figure 2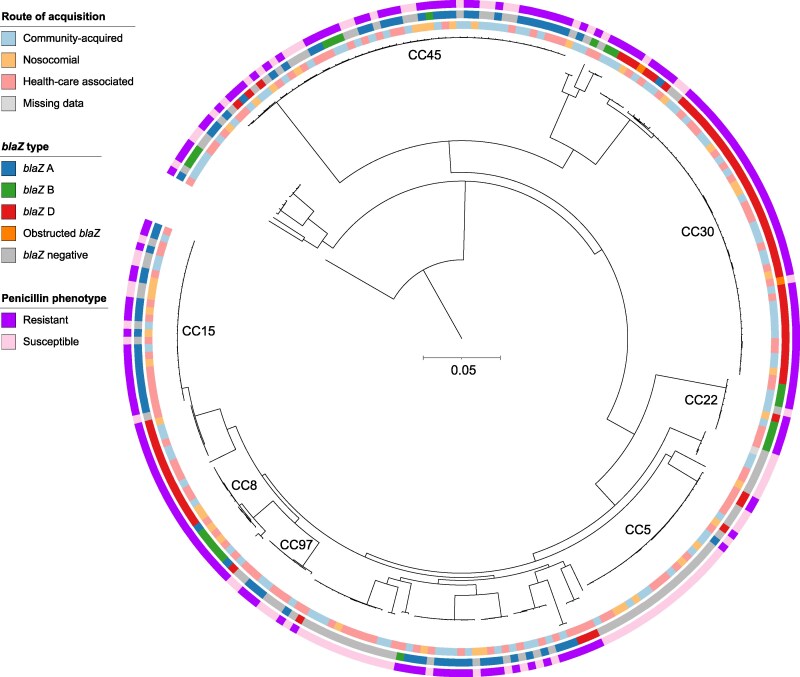 Figure 3
Figure 3- —ALF10.13039/501100001034
- —Research Committee of Region Örebro County
- —Regional Research Council Mid Sweden
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntimicrobial Resistance in Staphylococcus · Streptococcal Infections and Treatments · Bacterial Identification and Susceptibility Testing
Introduction
Staphylococcus aureus bacteraemia (SAB) is a common and life-threatening condition with significant morbidity and a 30-day mortality rate of approximately 20%.^1^ Prior to the introduction of penicillin G in the 1940s, SAB was associated with a mortality rate as high as 82%.^2–4^ The development of penicillin has revolutionized treatment outcomes and substantially reduced mortality.^4^ However, resistance to penicillin emerged shortly after its introduction.^5,6^ By the 1970s, 80%–95% of all SAB strains were resistant to penicillin G,^7^ leading many microbiology laboratories to discontinue susceptibility testing for penicillin in S. aureus.^8^
Penicillin G, a β-lactam antibiotic, inhibits penicillin-binding proteins that are essential for bacterial cell wall synthesis, ultimately causing cell death.^9^ Resistance to penicillin in S. aureus is mediated by the blaZ gene, which encodes penicillinase, an enzyme that hydrolyses the antibiotic’s β-lactam ring and thus renders it inactive.^10^ The blaZ gene is regulated by the blaR1 and blaI genes, and four types (A–D) have been described in S. aureus, located either on plasmids or on the chromosome.^11–13^ To counteract this resistance, semi-synthetic penicillinase-stable antibiotics such as oxacillin and flucloxacillin have been developed and are widely used for treating S. aureus infections.
Despite the historical dominance of penicillin-resistant S. aureus (PRSA), recent studies indicate an increasing prevalence of penicillin-susceptible S. aureus (PSSA), with rates ranging from 9% to 30% globally, depending on the region.^8,14–18^ This resurgence of PSSA has sparked renewed interest in penicillin G as a treatment option, given its favourable pharmacokinetic profile, including lower toxicity and reduced protein binding compared with isoxazolyl-penicillins.^8,19^ The optimal treatment approach for PSSA remains unclear, but retrospective studies have suggested superior outcomes when SAB is treated with penicillin G compared with cloxacillin or flucloxacillin.^20,21^
The reliability of phenotypic methods such as the disc diffusion test in detecting penicillin-susceptibility is a critical factor in the clinical decision-making process. The CLSI and EUCAST guidelines recommend disc diffusion testing using 1 and 10 U penicillin discs, respectively (Figure S1, available as Supplementary data at JAC Online).^19,22^ Although the test is generally reliable, variability in interpretation has been reported, particularly in zone edge assessment.^23^ Further complicating matters, the American Heart Association discourages the use of penicillin G for endocarditis caused by PSSA due to concerns about testing accuracy.^24^
The molecular epidemiology of emerging MRSA strains has been extensively studied, revealing the propagation of several clonal lineages with distinct genetic backgrounds.^25^ In contrast, our understanding of PSSA epidemiology is much more limited. However, previous studies have shown that the emergence of PSSA is not due to expansion of one nor a few dominant clones.^14,17,26,27^
This study aimed to evaluate the correlation between phenotypic and genotypic resistance of PSSA, to assess the reliability of EUCAST’s disc diffusion method, and to investigate the molecular epidemiology, genetic resistance markers, and routes of acquisition for PSSA in SAB.
Materials and methods
Ethics
Ethical approval was obtained from the regional ethical board in Uppsala, Sweden (reference number: 2019-04415), and the study was conducted in accordance with the 1964 Helsinki Declaration and its later amendments. The requirement for informed consent was waived due to the retrospective nature of this study.
Bacterial isolates and patient data
This population-based study was conducted in Örebro County, Sweden, from 2018 to 2019, covering a municipality of approximately 300 000 inhabitants. Clinical isolates were collected from adult patients (≥18 years) with confirmed SAB (defined as S. aureus present in one or more blood cultures) and analysed at the Department of Laboratory Medicine, Clinical Microbiology, Örebro University Hospital. The isolates were stored in a preservation broth [trypticase soy broth with 0.3% (w/w) yeast extract and 29% (v/w) horse serum] at −80°C. Exclusion criteria included polymicrobial bacteraemia (unless assessed as contamination according to medical charts), incomplete data, or special confidentiality restrictions in medical records. Patient charts were reviewed to confirm eligibility and to classify the route of acquisition as community-acquired, healthcare-associated, or nosocomial.^28^
Penicillin-susceptibility testing
Disc diffusion tests were performed according to EUCAST guidelines.^19^ A standardized inoculum was prepared by suspending bacterial colonies in sterile saline to achieve a turbidity equivalent to a 0.5 McFarland standard, and inoculated on Mueller-Hinton agar plates using 1 U penicillin G discs (Oxoid, Thermo Fisher Scientific, Basingstoke, UK). The plates were incubated in air at 35 ± 1°C for 18 ± 2 h. Zone diameters and edge appearances were assessed by two independent investigators (Figure 1). S. aureus reference isolates ATCC 29213 and ATCC 25923 were included as quality controls.
Disc diffusion test for 258 Staphylococcus aureus isolates with 1 U penicillin G disc according to the EUCAST guidelines. Mean zone diameter of two investigators. Strains with zone diameters of 6–21 mm were penicillin-resistant, and strains with zone diameters of 26–33 mm were penicillin-susceptible, as marked by the dotted line.
Whole-genome sequencing
Genomic DNA was extracted on a MagNA Pure 96 automated extraction platform (Roche, Basel, Switzerland) using the Viral NA Small Volume DNA Multi-Sample Kit (Roche), all according to manufacturers’ instructions. Quant-iT dsDNA BR and HS Assay kits (Thermo Fisher Scientific, Carlsbad, CA, USA) were used for DNA quantification and measured on the FLUOstar Omega (BMG LabTech). Libraries were prepared using the Illumina Nextera XT DNA Library Preparation Kit (Illumina, San Diego, CA, USA) and sequenced on the NextSeq 550 platform (Illumina) using a 300-cycle kit for paired-end 150 bp reads.
Genomic assembly and phylogenetic reconstruction
Draft genomes were assembled using version 3.13.1 of SPAdes.^29^ From these, blaZ alleles were identified using BLASTN and parsed for nonsense mutations to identify incomplete genes. In silico multilocus sequence typing was performed using mlst (https://github.com/tseemann/mlst) on the assembled genomes.
A core genome single nucleotide polymorphism (SNP) alignment was generated using version 1.2 of the Northern Arizona SNP Pipeline,^30^ with the chromosome of S. aureus NC_021554 as reference. This was subsequently used to infer phylogenetic relatedness using version 2.3.0 of IQ-TREE^31^ based on an alignment of 146 537 SNPs in a core genome of 2.0 Mbp (70%). The phylogenetic tree was visualized and annotated using iTOL (https://itol.embl.de/).
Statistics
Proportions were compared using Pearson’s chi-square test in version 29 of IBM SPSS Statistics. P-values <0.05 were considered statistically significant.
Results
Patient flow
In total, 296 S. aureus strains were identified, of which 25 were excluded due to polymicrobial bacteraemia, two were excluded due to incomplete data in medical charts, and seven were excluded due to confidentiality restrictions in medical records (Figure S2). Additionally, one strain was not subjected to Whole-genome sequencing (WGS), and one strain was not available for phenotypically testing due to technical issues. Two strains were identified as methicillin-resistant and were excluded from the analyses. This resulted in a final total of 258 S. aureus strains included for detailed analyses.
Phenotypic test results
Of the included isolates, 91 (35.1%) were phenotypically classified as PSSA (Figures 1–3). The assessments by the two independent investigators were 100% congruent when the zone diameter and zone edge appearance were evaluated together. Among these isolates, 89/91 (97.8%) did not carry the blaZ gene. Two (2.2%) phenotypically PSSA isolates, both belonging to clonal complex (CC) 30, were found to harbour the blaZ gene type D (Figure 3). However, one of these isolates lacked the usual start codon of the gene, while the other had a frameshift mutation caused by a single nucleotide insertion within the first 10 nucleotides of blaZ.
Proportions of CCs of penicillin-resistant and penicillin-susceptible Staphylococcus aureus strains.
A phylogenetic tree based on approximately 147 000 single nucleotide polymorphisms (SNPs) among 258 Staphylococcus aureus isolates causing bacteraemia. The tree depicts the population structure and highlights the major CCs. Three concentric annotation rings illustrate additional colour-coded metadata for each isolate: Inner ring: Route of acquisition classified as community-acquired, nosocomial or healthcare-associated. Middle ring: Prevalence and type of the blaZ gene. Outer ring: Phenotypical susceptibility demonstrating penicillin-resistance or penicillin-susceptibility. The scale bar represents 0.05 nucleotide substitutions per site.
The phenotypically PRSA isolates (n = 167) all harboured the blaZ gene. All four blaZ types were represented among these isolates: type A (n = 72; 43.1%), type B (n = 26; 15.6%), type C (n = 68; 40.7%), and type D (n = 1; 0.6%) (Figure 3).
Population structure
The population structure of the PSSA isolates (n = 91) was heterogeneous, with isolates distributed across multiple clonal complexes: CC5 (n = 22; 24.2%), CC45 (n = 18; 19.8%), CC12 (n = 11; 12.1%), CC15 (n = 8; 8.8%), CC97 (n = 5; 5.5%), CC30 (n = 4; 4.4%), CC7 (n = 2; 2.2%), CC22 (n = 1; 1.1%), and other (n = 20; 22.0%) (Figures 2 and 3).
Route of acquisition
The SAB was community-acquired in 103 (39.8%) cases, healthcare-associated in 114 (44.0%) cases, and nosocomial in 40 (15.4%) cases (Figures 1 and 3). In one case, the route of acquisition could not be determined due to insufficient information in the medical records. There was no statistically significant difference in the route of transmission between PRSA and PSSA (P = 0.73).
Discussion
The disc diffusion test according to EUCAST guidelines demonstrated high reliability in detecting PSSA by accurately differentiating strains with functional blaZ genes from those lacking or harbouring non-functional variants. In this study, nearly 98% of the isolates showed concordance between phenotypic resistance and blaZ status, emphasising the test’s robustness. Notably, 2.2% of PSSA isolates carried non-functional blaZ genes (type D). This is consistent with previous findings by Mama et al.^26^ who reported a 3.2% *blaZ-*positivity rate among PSSA isolates in Spain with various mutations in the blaZ gene (types A, B, and C). Jin et al.^17^ reported a slightly higher prevalence of blaZ-positive PSSA (7.9%) in China (types A and C). These findings, obtained through WGS, also revealed notable mutations in the blaZ gene and its regulatory gene blaR1. Interestingly, Coombs et al.^27^ found 9.6% blaZ-positive PSSA in Australia in 2020. Here, PSSA was defined according to results obtained from the automated microbiology system Vitek2, and when confirming the susceptibility with the disc diffusion test, all blaZ-positive strains were found to be phenotypically PRSA.
Our study identified a relatively high prevalence (35.1%) of PSSA among bacteraemic patients. This is consistent with the 33.1% reported by Resman et al.^14^ from southern Sweden, but stands in contrast to the lower prevalence rates reported from Spain (20.7%)^26^ and Australia (19.4%).^27^ Encouraging upward trends in PSSA prevalence have been observed both in Sweden between 1980 and 2010^32^ and in China between 2014 (3.5%) and 2019 (22.1%).^17^ The re-emergence of PSSA in recent years is not fully understood but is most likely driven by a combination of several factors. Resistance is often associated with a fitness cost for the bacteria, and a reduction in the selective pressure with the diminishing use of penicillin in favour of broad-spectrum antimicrobials might have given penicillin-susceptible strains a competitive advantage.^33,34^
The molecular epidemiology of PSSA in our cohort showed that CC5 and CC45 were the most prevalent CCs. These findings align with data from earlier studies in Sweden, Spain, and Australia.^14,26,27^ However, comparisons also highlight regional differences. For instance, CC398 was common in China and Spain, but was absent in our cohort as well as in an earlier Swedish study, and CC12 was more prevalent in our study than in previous reports.^14,17,26,27^ These findings highlight both shared trends and regional variations in the CC distribution.
We found no significant association between penicillin-resistance and the route of acquisition, with PSSA and PRSA being evenly distributed among community-acquired, healthcare-associated, and nosocomial infections. To the best of our knowledge, this aspect has not been previously investigated, although healthcare-associated and nosocomial infections are often associated with multidrug resistance.^35^
The interpretation of disc diffusion tests remains a critical component of PSSA detection. While our study achieved 100% concordance between investigators in the combined assessment of zone diameter and edge appearance, previous studies have highlighted variability in this respect. Hombach et al.^36^ demonstrated inter-individual variability among nine investigators when evaluating the performance of the disc diffusion test in discriminating between PSSA and PRSA. However, the sensitivity was likely related to the training level of the investigator. Moreover, in their study, the gold standard was based on detection of the blaZ gene without further investigation of mutations.
The presence of non-functional blaZ genes in phenotypically susceptible strains poses a potential risk of misclassification. In our study, two strains carried a non-functional blaZ gene yet were phenotypically susceptible. Although the clinical significance of non-functional blaZ genes remains unclear, concerns have been raised regarding the potential reversibility of blaZ mutations. Mama et al.^26^ observed revertants in two blaZ-positive, phenotypically susceptible strains. Additionally, Eriksen et al.^37^ reported a case where a clinical isolate lost a plasmid-borne blaZ gene during subculture, converting from resistant to susceptible.
Despite these concerns, retrospective studies have not demonstrated inferior clinical outcomes associated with penicillin treatment of PSSA. For instance, Mok et al.^38^ reported no significant differences in mortality or treatment failure between PSSA patients treated with penicillin and those treated with other agents. Furthermore, previous studies have found that treatment with isoxazolyl-penicillin was associated with higher mortality than treatment with penicillin G.^20,21^ Prospective trials, such as the ongoing S. aureus Network Adaptive Platform trial (www.snaptrial.com.au), aim to further elucidate these findings by comparing penicillin with flucloxacillin in bloodstream infections caused by PSSA.^39^ This trial employs disc diffusion testing following EUCAST or CLSI guidelines depending on laboratory practices.^39,40^
Limitations
This study has several limitations. It was conducted using PSSA isolates obtained from a limited geographical area. Furthermore, only the 1 U penicillin disc was used, as recommended by the EUCAST guidelines, rather than additionally using the 10 U penicillin disc specified in the CSLI guidelines. This might reduce the applicability of the results in regions following CSLI guidelines. However, Skov et al.^41^ reported 96% sensitivity and 100% specificity with both 1 U (EUCAST guidelines) and 10 U (CSLI guidelines) penicillin discs when the blaZ gene was used as the gold standard. Moreover, Papanicolas et al.^42^ found an even greater difference in sensitivity between the 1 U disc (100%) and the 10 U disc (89%).
Conclusion
In conclusion, the prevalence of PSSA among bacteraemic patients in our study was 35.1%. The disc diffusion test proved reliable for detecting PSSA by discriminating strains with functional blaZ genes from those lacking the gene or carrying non-functional variants. Diverse lineages were seen among the PSSA strains, with CC5, CC45, CC12, and CC15 being the most common CCs in our cohort.
Supplementary Material
dkaf187_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1van Hal SJ, Jensen SO, Vaska VL et al Predictors of mortality in Staphylococcus aureus bacteremia. Clin Microbiol Rev 2012; 25: 362–86. 10.1128/CMR.05022-1122491776 PMC 3346297 · doi ↗ · pubmed ↗
- 2Ligon BL . Penicillin: its discovery and early development. Semin Pediatr Infect Dis 2004; 15: 52–7. 10.1053/j.spid.2004.02.00115175995 · doi ↗ · pubmed ↗
- 3Skinner D, Keefer CS. Significance of bacteremia caused by Staphylococcus aureus. Arch Intern Med 1941; 68: 851–75. 10.1001/archinte.1941.00200110003001 · doi ↗
- 4Smith IM, Vickers AB. Natural history of 338 treated and untreated patients with staphylococcal septicaemia (1936-1955). Lancet 1960; 1: 1318–22. 10.1016/S 0140-6736(60)92303-513831996 · doi ↗ · pubmed ↗
- 5Kirby WM . Extraction of a highly potent penicillin inactivator from penicillin resistant staphylococci. Science 1944; 99: 452–3. 10.1126/science.99.2579.45217798398 · doi ↗ · pubmed ↗
- 6Barber M, Rozwadowska-Dowzenko M. Infection by penicillin-resistant staphylococci. Lancet 1948; 2: 641–4. 10.1016/S 0140-6736(48)92166-718890505 · doi ↗ · pubmed ↗
- 7Chambers HF . The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis 2001; 7: 178–82. 10.3201/eid 0702.01020411294701 PMC 2631711 · doi ↗ · pubmed ↗
- 8Cheng MP, René P, Cheng AP et al Back to the future: penicillin-susceptible Staphylococcus aureus. Am J Med 2016; 129: 1331–3. 10.1016/j.amjmed.2016.01.04826924388 · doi ↗ · pubmed ↗