Unmasking Cryoglobulinemia: A Cold-Blooded Complication of Hepatitis C
Alexandra M. Arges, Ari Levine

TL;DR
A man with hepatitis C developed cryoglobulinemia, an autoimmune condition, and improved after treatment, though some symptoms persisted.
Contribution
This case highlights HCV's role in mixed cryoglobulinemia and the effectiveness of antiviral therapy in managing the condition.
Findings
The patient's symptoms resolved after antiviral treatment for HCV.
Mixed cryoglobulinemia was confirmed through positive cryoglobulin testing.
Neuropathy persisted despite treatment, indicating possible long-term effects.
Abstract
A 43-year-old man presents to the hospital with two weeks of persistent fevers, accompanied by myalgias, hematochezia, and abdominal pain. Acute infectious causes were ruled out, and elevated inflammatory markers suggested inflammatory diarrhea or autoimmune conditions. Esophagogastroduodenoscopy (EGD) and colonoscopy were negative. Further testing showed positive antinuclear antibodies (ANAs), ribonucleoprotein (RNP), rheumatoid factor (RF), and hepatitis C virus (HCV) RNA, suggesting an HCV-associated autoimmune process. Hematuria and neuropathic pain raised suspicion for mixed cryoglobulinemia secondary to HCV, supported by low complement levels. Treatment started with prednisone. Cryoglobulins came back positive, confirming mixed cryoglobulinemia secondary to HCV. The patient was referred to the hepatology clinic for antiviral treatment, where he completed treatment, with symptoms…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1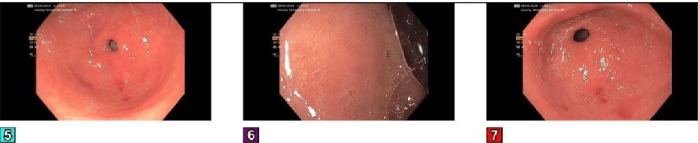 Figure 2
Figure 2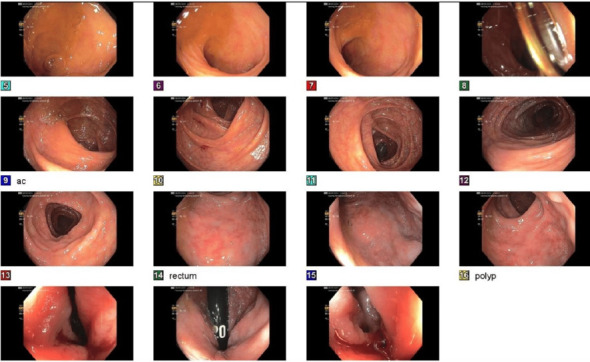 Figure 3
Figure 3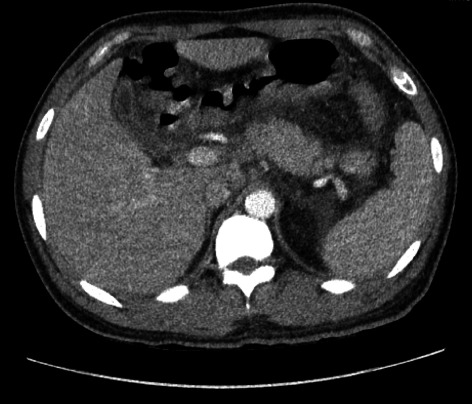 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · Liver Disease Diagnosis and Treatment · Hepatitis B Virus Studies
1. Introduction
Hepatitis C affects ∼71 million people globally, with approximately 1.5 million new infections annually [1, 2]. Approximately 80% of acute hepatitis C cases are asymptomatic, while the rest show fever, fatigue, and gastrointestinal symptoms. Up to two-thirds of the cases have extrahepatic manifestations, including mixed cryoglobulinemic vasculitis, B-cell lymphoma, autoimmune cytopenia, hypothyroidism, cardiovascular disease, and type 2 diabetes [2]. When approaching fever of unknown origin, we often prioritize ruling out infectious etiologies, including the viral hepatitides [3]. However, due to acute hepatitis C rarely being symptomatic, a clinician should inquire how chronic hepatitis C could lead to persistent fevers and consider an autoimmune etiology, such as mixed cryoglobulinemic vasculitis.
2. Case Presentation
A 43-year-old male presented to the hospital with two weeks of fevers, myalgias, diarrhea, and bloody stools. He denied any rashes, chest pain, or shortness of breath. Social history was notable for no intravenous drug use, heavy alcohol use, or tobacco use. There was no known personal or family history of autoimmune disease or known inflammatory bowel disease. On examination, he was hypertensive, tachycardic, and febrile, with periumbilical tenderness to palpation and submental cervical lymphadenopathy. As shown in Table 1, the patient's labs showed elevated liver enzymes (AST/ALT), elevated white blood cell count (WBC), elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR), and positive hepatitis C antibodies. Initial imaging was unremarkable.
On day two, he continued to experience fevers, yellow stools, and abdominal pain. The infectious workup was negative, and attention shifted to the possibility of inflammatory diarrhea. Tests for autoimmune conditions were ordered due to elevated ESR, CRP, and ferritin, as shown in Table 1.
By day three, symptoms persisted, and additional labs, as shown in Table 1, revealed positive ANA, RNP, and RF, as well as elevated hepatitis C RNA PCR, raising concerns for a hepatitis C-linked autoimmune process. Urinalysis, as shown in Table 1, also revealed hematuria, suggesting possible glomerular involvement. Esophagogastroduodenoscopy (EGD) and colonoscopy, as shown in Figures1, 2, and 3, revealed erosive gastropathy as well as erythematous rectal mucosa but lacked overt abnormalities to explain his symptoms.
On day five, the patient developed neuropathic pain in his feet, and mixed cryoglobulinemia secondary to hepatitis C was suspected. On day six, with our patient having persistent symptoms, low C3 and C4 levels, and a pending cryoglobulin test, mixed cryoglobulinemia was highest on our differential. CT imaging, as shown in Figure 4, revealed trace pleural effusion and mesenteric edema, which have been observed in the setting of cryoglobulinemia. The patient was started on prednisone 60 mg daily for suspected cryoglobulinemia and gabapentin for neuropathy, and plans were made for outpatient follow-up at a hepatitis C clinic.
On day seven, cryoglobulins were confirmed positive, as shown in Table 1, clinching the diagnosis of mixed cryoglobulinemia secondary to hepatitis C. The patient's neuropathy improved with steroids and gabapentin, and he was discharged to home, with close follow-up in hepatology clinic. Great efforts were made to try and initiate an antiviral in the inpatient setting, but these medications were not on formulary, and infectious disease consultants recommended initiation in the clinic, where his laboratory values could be monitored.
The patient followed up in clinic upon discharge and completed 8 weeks of Mavyret (glecaprevir/pibrentasvir), antiviral therapy for hepatitis C. His hepatitis C viral load was undetectable after 8 weeks of antiviral treatment. His symptoms of fevers, headache, malaise, arthralgias, and cough resolved. However, he continued to experience neuropathy in his feet, which improved with gabapentin.
3. Discussion
We present a case of HCV-associated mixed cryoglobulinemia that manifested as fever of unknown origin with predominant gastrointestinal symptoms and lacking a petechial rash. This case serves as a reminder to consider extrahepatic manifestations of HCV even in the absence of characteristic symptoms.
Mixed cryoglobulinemia is an extrahepatic complication of HCV resulting in proteins that precipitate from a patient's serum or plasma at temperatures lower than 37°C [2, 4, 5]. Reported prevalence in patients with HCV is between 40% and 65% [4]. The most common presenting symptom is a purpuric rash [2, 4, 5]. GI involvement, arthralgias, peripheral neuropathy, and glomerulonephritis can also be present [2, 4, 5].
Mixed cryoglobulinemia (types II and III) presents with polyclonal IgG and IgM with elevated rheumatoid factor (RF) and often with low C4 and normal C3 [4, 5]. Meltzer's triad of purpura, fatigue, and arthralgias appears in 80% of the cases, with purpura being the most common symptom [4]. Peripheral neuropathy is also seen [2, 4, 5]. The most common neurological consequence of HCV is peripheral neuropathy, with approximately 10% of patients with HCV having clinically symptomatic sensory or motor peripheral neuropathy, and approximately 90% of the patients with HCV-associated mixed cryoglobulinemia having neuropathy [6]. Renal involvement in mixed cryoglobulinemia shows a membranoproliferative glomerulonephritis detected through renal failure or nephritic syndrome [2, 4]. Management varies with severity, from antivirals in mild cases to IV steroids and plasma exchange for severe cases [2, 4]. Access remains a challenge for HCV treatment, with treatments lasting 8–12 weeks [1]. Hepatitis C is not typically associated with acute febrile illness, but mixed cryoglobulinemia should be considered if neuropathic pain, high inflammatory markers, positive RF, and cryoglobulins are present.
4. Conclusions
Hepatitis C is not typically associated with acute febrile illness, but mixed cryoglobulinemia should be considered if neuropathic pain, high inflammatory markers, positive RF, and cryoglobulins are present. Treatment for mixed cryoglobulinemia involves treating the underlying cause (in this case, HCV, with antivirals) and calming the immune response with steroids, rituximab, or even plasmapheresis. Peripheral cryoglobulin-related neuropathy in HCV remains difficult to treat, with some trials showing success with rituximab or plasmapheresis [5, 6].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu C. H. Kao J. H. Acute Hepatitis C Virus Infection: Clinical Update and Remaining Challenges Clinical and Molecular Hepatology 202329362364210.3350/cmh.2022.034936800699 PMC 10366792 · doi ↗ · pubmed ↗
- 2Cacoub P. Saadoun D. Extrahepatic Manifestations of Chronic HCV Infection New England Journal of Medicine 2021384111038105210.1056/NEJ Mra 203353933730456 · doi ↗ · pubmed ↗
- 3Haidar G. Singh N. Fever of Unknown Origin New England Journal of Medicine 2022386546347710.1056/NEJ Mra 211100335108471 · doi ↗ · pubmed ↗
- 4Bhandari J. Awais M. Aeddula N. R. Cryoglobulinemia Stat Pearls, Treasure Island (FL) 2024 Stat Pearls Publishing
- 5Boleto G. Vieira M. Saadoun D. Cacoub P. Hepatitis C Virus-Related Vasculitis Clinics and Research in Hepatology and Gastroenterology 2021455 p. 10157510.1016/j.clinre.2020.11.00533268038 · doi ↗ · pubmed ↗
- 6Benstead T. J. Chalk C. H. Parks N. E. Treatment for Cryoglobulinemic and Non-Cryoglobulinemic Peripheral Neuropathy Associated With Hepatitis C Virus Infection Cochrane Database of Systematic Reviews 2014201412 p. CD 01040410.1002/14651858.CD 010404.pub 22-s 2.0-84925222470 PMC 1123253225525951 · doi ↗ · pubmed ↗