Successful Primary Repair of a Traumatic Distal Biceps Tendon Rupture With the Arthrex Biceps Button System and Platelet-Rich Plasma Therapy: A Case Report and Surgical Outcome
Connor J O'Leary, Pasquale Gencarelli, James M Lee, Rahul Mittal

TL;DR
A 48-year-old man successfully recovered from a biceps tendon rupture after surgery using a button system and platelet-rich plasma therapy.
Contribution
Demonstrates the effectiveness of combining the Arthrex button system with platelet-rich plasma for faster recovery in biceps tendon repair.
Findings
The patient returned to normal activities within three months post-surgery.
Platelet-rich plasma may enhance recovery in distal biceps tendon repair.
Significant improvements in pain, range of motion, and strength were observed.
Abstract
Traumatic rupture of the distal biceps tendon is a relatively rare injury often requiring surgical reconstruction. The typical surgical repair for a traumatic distal biceps tendon rupture is a single anterior incision with cortical button fixation, followed by early mobilization, with most patients returning to full activity or sport at approximately six months postoperatively. We present a case of a 48-year-old male patient who experienced a traumatic distal biceps rupture following a water skiing accident. The patient underwent surgical repair using the Arthrex button system with the application of platelet-rich plasma. Postoperative follow-up showed significant improvement in pain, range of motion, and strength, with the patient returning to normal activities within three months. This case highlights the successful management of a distal biceps rupture and the potential role of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3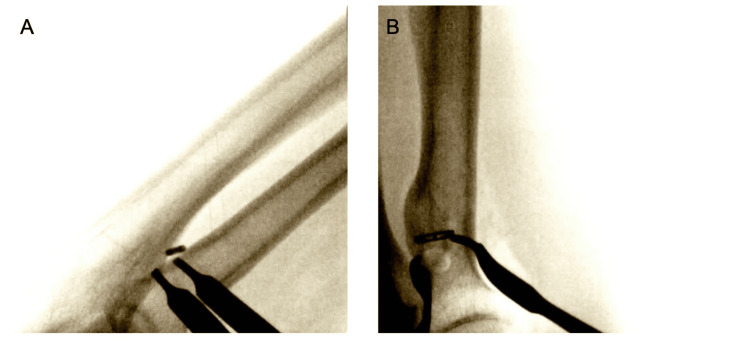 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Shoulder Injury and Treatment · Orthopedic Surgery and Rehabilitation
Introduction
Distal biceps tendon (DBT) ruptures are relatively uncommon injuries that typically occur in middle-aged males during forceful eccentric contraction of the biceps muscle against a flexed elbow such as during weightlifting or other sporting activities [1]. DBT ruptures typically affect the dominant arm, and individuals involved in athletics or high-load resistance training are particularly susceptible [1,2]. The incidence of DBT rupture has been reported between 1.2 and 5.4 per 100,000 people, and reports of DBT ruptures may be increasing due to a combination of factors, including an aging male population engaging in prolonged physical activity and advancements in clinical and diagnostic imaging [1,3-5]. While a DBT injury is typically precipitated by a forceful contraction event, risk factors, such as tobacco use, increased body mass, use of anabolic steroids, and pre-existing tendinosis, have been linked to an increased risk of DBT injury [1,3,6,7]. DBT ruptures can result in significant function impairment, loss of supination, flexion strength, and decreased resistance to fatigue [8].
Non-surgical treatment of DBT rupture is reserved for those who have low functional demand or are medically unfit to proceed with surgery [9]. It has been shown that healthy, active patients with complete DBT tears benefit from early surgical intervention, yielding improved strength and functional outcomes [10,11]. A variety of surgical plans may be considered for a DBT rupture repair, including anterior, posterior, dual-incision, or endoscopic approaches [12,13]. Less severe cases of acute DBT ruptures may be repaired primarily, while more complex acute and chronic cases may require a graft during surgical repair [5]. There are a number of published cases of DBT rupture repair; however, the level of evidence in most of these reports is regarded as weak [13]. Additionally, as orthopedic technology and techniques have advanced, there are new permutations of approaches for DBT rupture repair. Newer techniques, such as using platelet-rich plasma (PRP), which is an extract derived from the patient’s own blood that is rich in growth factors that facilitate tissue healing, have gained recognition in the conservative management of DBT injuries [14,15]. However, the lack of consensus on the surgical approach for DBT repair and the evolving toolbox of orthopedic approaches calls for more literature to be published on DBT rupture repairs. The purpose of this report is to describe a DBT rupture repair using an Arthrex BicepsButton™ Implant System (Arthrex GmbH, Munich, Germany) with the application of intraoperative PRP.
Case presentation
We present the case of a 48-year-old right-hand-dominant male with a traumatic rupture of his right DBT sustained while water skiing. The patient reported feeling a pop in his right elbow while water skiing with his arm outstretched. Subsequently, he experienced immediate pain, swelling, and functional impairment. Clinical examination revealed mild swelling in the medial aspect of the elbow, an abnormal appearance of the right biceps, and weakness in supination, pronation, and flexion, consistent with a DBT rupture. The initial evaluation included X-rays, which ruled out fractures or dislocations. An MRI confirmed the diagnosis, showing 4 centimeters of tendon retraction. Given the patient's high-demand lifestyle and desire for restoration of strength, surgical intervention was recommended.
Two and a half weeks later, the patient underwent primary repair of the distal biceps tendon using the Arthrex BicepsButton™ Implant System, supplemented with the application of PRP. The procedure was performed using a tourniquet under general anesthesia, with the patient in a supine position. A standard longitudinal incision was made distal to the flexion crease, and dissection was carried down to the biceps tendon (Figure 1). Care was taken to protect the lateral antebrachial cutaneous nerve throughout the procedure. After identification of the tendon, any scar tissue was debrided, and the biceps tendon was dissected out. A whipstitch was then placed in the distal biceps and measured (Figure 2). The Arthrex button system was then used for tendon reattachment (Figure 3). With open visualization and fluoroscopic guidance, the bicipital tuberosity was localized, and bicortical drilling was performed. The button was then advanced bicortically and flipped into place. The tendon was advanced into its anatomical location using a tension slide technique, and positioning of the button system was confirmed with fluoroscopy (Figure 4). Additional sutures were placed through the tendon substance to reinforce the repair, and PRP was injected into the repair site to promote healing. The wound was closed in layers, and a well-padded posterior splint was applied to maintain elbow flexion at 90 degrees. Postoperative neurologic examination revealed intact thumb and wrist extension with brisk capillary refill of all digits.
Complete DBT rupture with 4 cm retractionDBT: distal biceps tendon
Distal biceps tendon isolationThe DBT is isolated through a longitudinal incision distal to the flexion crease and prepared with a whipstitch.DBT: distal biceps tendon
DBT anchored with the Athrex button systemDBT: distal biceps tendon
Intraoperative fluoroscopic radiographs demonstrating alignment and confirmation of placementA. Anterior-Posterior; B. Lateral
Postoperatively, the patient’s posterior splint was removed at the one-week follow-up visit and replaced with a hinged elbow brace for three weeks. Physical therapy was started after the four-week follow-up visit. The patient reported progressively improving pain, endorsing a 2/10 pain level at the one-week follow-up and a 0/10 pain level at the eight-week follow-up appointment. Functionally, the patient had a 120-degree range of motion in 3 degrees of extension and flexion at the 8-week follow-up visit, while continuing physical therapy. At three months postoperative, the patient reported major progress. Clinical examination revealed a healed incision; full grip strength; full pronation, supination, extension, and flexion; and 5/5 strength in all planes of motion. The patient reported working with physical therapy to be transferred to the gym and was cleared for all activities.
Discussion
A systematic review by Amarasoryia et al. (2020) determined that after a DBT repair, the overall complication rate was 25%, the major complication rate was 4.6%, and the minor complication rate was 20.4% [16]. With a growing list of fixation systems and adjunct therapies, such as PRP, optimal surgical management of orthopedic conditions like complete DBT ruptures must be continually re-evaluated. While some biomechanical studies have shown that cortical button systems might handle the maximum peak load, suture anchor and interosseous screw techniques showed the least displacement, demonstrating an argument for multiple DBT rupture repair approaches [11]. Currently, there is no consensus regarding the best surgical approach for DBT rupture repair [12,17,18]. Furthermore, the long-term effects of adjunct tissue healing therapies like PRP are unknown. Ultrasound-guided PRP injection therapy has been shown to be safe and effective in patients with distal biceps tendinopathy, but its intraoperative uses have not been explored in the literature [14,15]. While the application of intraoperative PRP has shown promise in orthopedic procedures, such as rotator cuff repairs, its role in DBT rupture repair has not been discussed in the literature [19]. Ultimately, while the specifics of operative approach may vary, surgical repair of DBT rupture remains the standard of care for all patients who can tolerate the procedure. The specific surgical approach taken relies on a combination of an understanding of the distal biceps anatomy, patient assessment, and the surgeon's experience with tendon reattachment techniques [9].
It is crucial to acknowledge the limitations of the existing evidence base, particularly the predominance of low-level evidence in the most cited publications. While our case demonstrated a positive outcome, we don't have long-term data on this patient. Notably, our case provides a single patient experience without a control to serve as a comparison. This highlights the need for further research, including larger prospective cohort studies and randomized controlled trials, to clarify the optimal management strategies for DBT rupture repair.
Conclusions
This case highlights the successful management of traumatic DBT rupture using a single-incision surgical approach, resulting in favorable outcomes and patient satisfaction. The use of an Arthrex cortical button system and the incorporation of PRP adjunct therapy may offer additional benefits in promoting tissue healing and functional recovery. This case demonstrates a single, successful outcome, but further studies are warranted to evaluate the long-term efficacy and optimal timing of surgical intervention in similar cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Distal biceps tendon ruptures: incidence, demographics, and the effect of smoking Clin Orthop Relat Res Safran MR Graham SM 2752832002 https://pubmed.ncbi.nlm.nih.gov/12439270/12439270 · pubmed ↗
- 2Sports-related injuries of the biceps and triceps Clin Sports Med Bain GI Durrant AW 5555762920102088389710.1016/j.csm.2010.07.002 · doi ↗ · pubmed ↗
- 3Distal biceps tendon ruptures: an epidemiological analysis using a large population database Am J Sports Med Kelly MP Perkinson SG Ablove RH Tueting JL 201220174320152606340110.1177/0363546515587738 · doi ↗ · pubmed ↗
- 4Po CUS identification of distal biceps tendon rupture: a case report Int J Emerg Med Ali N Tan A Chenkin J 391720243847570810.1186/s 12245-024-00598-1PMC 10935799 · doi ↗ · pubmed ↗
- 5Female patient with bilateral distal biceps tendon reconstruction: a case report Trauma Case Rep Bolia IK Shontz EC Dobitsch A Mayfield CK Bashrum BS Weber AE 1008704720233738302710.1016/j.tcr.2023.100870 PMC 10293761 · doi ↗ · pubmed ↗
- 6Ruptured tendons in anabolic-androgenic steroid users: a cross-sectional cohort study Am J Sports Med Kanayama G De Luca J Meehan WP 3rd 263826444320152636243610.1177/0363546515602010 PMC 5206906 · doi ↗ · pubmed ↗
- 7Histopathological changes preceding spontaneous rupture of a tendon. A controlled study of 891 patients J Bone Joint Surg Am Kannus P Józsa L 15071525731991 https://pubmed.ncbi.nlm.nih.gov/1748700/1748700 · pubmed ↗
- 8Distal biceps tendon repair and reconstruction J Hand Surg Am Srinivasan RC Pederson WC Morrey BF 48564520203190133210.1016/j.jhsa.2019.09.014 · doi ↗ · pubmed ↗