Analysis of inter-hospital transfer on clinical outcomes after primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: A secondary analysis of the BRIGHT-4 trial
Xiaolin Su, Miaohan Qiu, Chengqi Gu, Xiuhui Yang, Bin Liu, Fanbo Meng, Bin Ning, Wei Li, Zhixiong Zhong, Zhengzhong Wang, Bei Shi, Zhuo Shang, Zhenyang Liang, Yi Li, Yaling Han, Gregg W. Stone, Syba Sunny, Alison Farrell, Alison Farrell, Alison Farrell

TL;DR
This study found that transferring STEMI patients for PCI does not worsen 30-day outcomes, and bivalirudin reduces risks of death and bleeding compared to heparin.
Contribution
The study provides evidence that inter-hospital transfer does not negatively impact outcomes and that bivalirudin is effective regardless of transfer status.
Findings
Transferred patients had no worse 30-day outcomes compared to directly admitted patients.
Bivalirudin reduced the risk of death or major bleeding in both transferred and directly admitted patients.
Timely PCI was more important than the need for transfer in determining outcomes.
Abstract
Previous studies evaluating the influence of inter-hospital transfer on mortality in ST-segment elevation myocardial infarction (STEMI) patients undergoing primary percutaneous coronary intervention (PCI) reported conflicting results. The multicenter BRIGHT-4 trial demonstrated that bivalirudin plus a post-PCI high-dose infusion (1.75 mg/kg/h) reduced the 30-day primary endpoint of all-cause mortality or Bleeding Academic Research Consortium (BARC) types 3–5 bleeding compared with heparin monotherapy in STEMI patients. This study aimed to assess the impact of inter-hospital transfer on clinical outcomes and the effectiveness of bivalirudin versus heparin in STEMI patients undergoing PCI. In BRIGHT-4, 2,121 (35.7%) patients were transferred to a tertiary hospital for primary PCI while 3,817 (64.3%) were directly admitted to an interventional facility. The primary outcome was the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
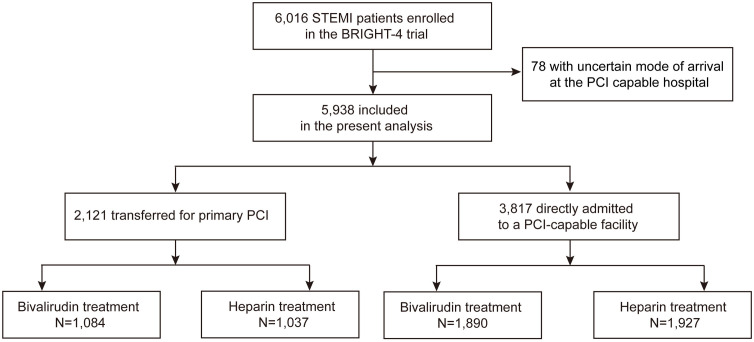 Fig 1
Fig 1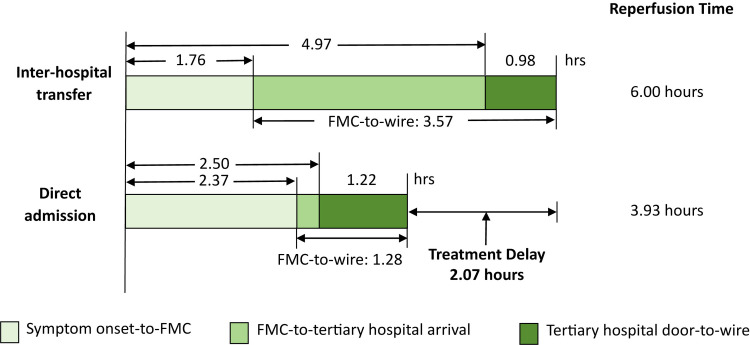 Fig 2
Fig 2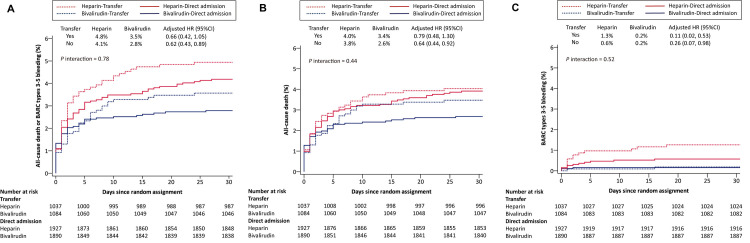 Fig 3
Fig 3- —Chinese Society of Cardiology Foundation
- —National Key Research and Development Project
- —National Key Research and Development Project
- —Jiangsu Hengrui Pharmaceuticals
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Antiplatelet Therapy and Cardiovascular Diseases · Venous Thromboembolism Diagnosis and Management
Background
Primary percutaneous coronary intervention (PCI) is the preferred method to achieve reperfusion in patients with ST-segment elevation myocardial infarction (STEMI), provided that it can be performed in a timely fashion [1,2]. However, approximately 20%−50% of STEMI patients require transfer to a PCI center after initial presentation to a non-PCI capable hospital [3–6], resulting in longer ischemic times compared with direct admission to tertiary interventional hospitals. As a result, more than 40% of transferred patients in the United States fail to achieve the guideline-recommended first medical contact (FMC)-to-device time of 120 min [7], which may reduce myocardial salvage. In some studies, inter-hospital transfer for primary PCI has been identified as a major predictor of higher 12-month mortality [4], whereas other studies have not demonstrated clearly worsened outcomes after transfer for primary PCI [6,8–11].
Prolonged ischemic time has been associated with increased fibrin content of intracoronary thrombi [12], making them more resistant to anticoagulation with heparin which binds primarily with fluid-phase but not clot-bound thrombus. Bivalirudin, in contrast, has high affinity for both clot-bound and fluid-phase thrombin, preventing the initiation and propagation of clot formation [13]. Bivalirudin might thus be a more appropriate anticoagulation strategy for patients presenting late after symptom onset, including those undergoing inter-hospital transfer. In the HORIZONS-AMI trial, procedural anticoagulation with bivalirudin resulted in lower rates of cardiac mortality and major bleeding compared with heparin plus a glycoprotein IIb/IIIa inhibitor (GPI), regardless of transfer for primary PCI [6]. However, in current clinical practice in which GPI are not routinely used with heparin and a post-PCI bivalirudin infusion is recommended after primary PCI, little is known regarding the outcomes of and the optimal anticoagulation strategy for transferred patients with STEMI.
In the large-scale BRIGHT-4 trial, bivalirudin plus a post-PCI high-dose infusion (1.75 mg/kg/h) for 2–4 hrs reduced the 30-day rates of all-cause mortality, major bleeding and stent thrombosis compared with heparin monotherapy in patients with STEMI undergoing primary PCI [14]. The present post hoc analysis therefore aimed to compare the clinical outcomes of patients with STEMI transferred to tertiary hospitals for PCI with those who presented directly at an interventional facility, and to investigate whether inter-hospital transfer had an impact on the outcomes of anticoagulation with bivalirudin versus heparin as used in contemporary clinical practice.
Methods
Study design and participants
The design, major inclusion and exclusion criteria, and results of the BRIGHT-4 trial have been published [14,15]. Briefly, BRIGHT-4 was an investigator-sponsored, open-label, randomized controlled trial conducted at 87 clinical centers in China. Between February 14th, 2019 and April 7th, 2022, 6,016 patients with STEMI undergoing primary PCI with radial artery access within 48 hrs of symptom onset were enrolled. Exclusion criteria included use of fibrinolytic therapy, anticoagulants or GPI before cardiac catheterization. Eligible patients were randomly assigned (1:1) to receive either bivalirudin with a post-PCI high-dose infusion for 2–4 hrs or unfractionated heparin monotherapy. The use of GPI was reserved for procedural thrombotic complications in both groups. The study protocol was approved by the ethics committee of the General Hospital of Northern Theatre Command as well as at each participating center (S1 Text). The study was performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was provided by all patients or their legal representatives before randomization. Further details regarding the original study protocol and statistical analysis plan are provided in the Supporting Information (S2 and S3 Texts). This study is reported as per the Consolidated Standards of Reporting Trials (CONSORT) guideline (S1 Checklist).
For the present post hoc analysis, 78 (1.3%) patients with uncertain mode of arrival at the PCI capable hospital were excluded. The remaining 5,938 patients were categorized into two groups: (1) patients who initially presented at a tertiary hospital for primary PCI (the direct admission group), and (2) patients who initially presented at a non-PCI capable hospital before being transferred to a tertiary facility for PCI (inter-hospital transfer group). All patients were randomized at the tertiary facility before receiving any study drug. All patients also received dual antiplatelet therapy with aspirin and either clopidogrel or ticagrelor at physician discretion. Other medications were prescribed according to current guidelines.
Clinical outcomes and definitions
The primary outcome was the composite of all-cause death or Bleeding Academic Research Consortium (BARC) types 3–5 bleeding occurring within 30 days after randomization. The secondary outcomes were major adverse cardiac or cerebral events (MACCE, defined as the composite of all-cause death, (recurrent) myocardial infarction (MI), ischemia-driven target vessel revascularization (TVR), or stroke) and its components; stent thrombosis according to Academic Research Consortium definite or probable criteria; BARC types 2–5 bleeding; the composite of all-cause death or BARC types 2–5 bleeding; acquired thrombocytopenia; and net adverse clinical events (NACE, the composite of MACCE or BARC types 3–5 bleeding). The specific definitions for these outcomes have been previously described [14]. All endpoints were adjudicated by an independent committee using original source documents.
Symptom onset was the time that symptoms (e.g., chest pain, dyspnea, cardiac arrest) began that led the patient to seek medical attention [16]. FMC was the time when the paramedics arrived at the patient’s side. The times of arrival at the transfer and tertiary hospitals were recorded. Wire time was the time of wire crossing the infarct lesion [2].
Statistical analysis
Continuous variables are presented as mean and standard deviation (SD) or median and interquartile ranges (IQR) and were compared using a Student t test or the Wilcoxon rank-sum test respectively. Categorical variables are expressed as frequencies (%) and were compared using the χ² test or Fisher’s exact test. No imputation was used to infer missing values. Time-to-event rates were estimated using the Kaplan–Meier method and were compared with the log-rank test.
Multivariable Cox proportional hazards regression models were used to adjust baseline imbalances between groups. Variables included in the Cox model were age, sex, body mass index, hypertension, diabetes, smoking, previous MI, previous PCI, previous stroke, Killip class, hemoglobin, platelet count, estimated glomerular filtration rate (eGFR), medical therapy (randomized anticoagulant, aspirin, P2Y12 inhibitors, bail-out tirofiban), arterial access, coronary arteries treated, thrombus aspiration, pre- and post-PCI TIMI flow, and procedure strategies (PCI, coronary artery bypass surgery, coronary angiography, none). The Cox proportional hazards assumption for the primary outcome was confirmed graphically using log(−log) plots. Given the multi-center design of the study, Cox frailty models were further applied to estimate hazard ratios (HRs) for the primary outcome, incorporating center as a random intercept to account for clustering effects.
To confirm the robustness of our findings, propensity score matching (PSM) was conducted between patients with and without inter-hospital transfer using a 1:1 nearest-neighbor matching algorithm with a caliper of 0.05 standard deviations. The matched variables were identical to those included as covariates in multivariable Cox models. In addition, we excluded patients with symptom onset-to-wire time exceeding 24 hrs and employed multivariable Cox models to test the consistency of our hypothesis. All statistical analyses were two-sided and were performed with SAS version 9.4.
Results
Baseline characteristics
Among the 5,938 study patients, 2,121 (35.7%) were transferred to the tertiary hospital for primary PCI while 3,817 (64.3%) patients were directly admitted to a PCI-capable facility. The flowchart of the study is provided in Fig 1. Patients in the inter-hospital transfer group were less likely to have hypertension and history of MI or PCI compared with those in the direct admission group but were more likely to smoke and have anemia (Table 1). Symptom onset-to-FMC time was significantly shorter in the inter-hospital transfer group as was the duration from tertiary hospital arrival to wire time. However, after accounting for a median inter-hospital transfer time of 132 min, the median symptom onset-to-wire time was approximately 2 hrs longer in the inter-hospital transfer group compared with the direct admission group (6.00 versus 3.93 hrs, P < 0.0001) (Table 1 and Fig 2).
Table 1: Baseline characteristics.
The flowchart of the study population.PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
Intervals for patients to a PCI facility.PCI, percutaneous coronary intervention; FMC, first medical contact.
Procedural data and medications are presented in Tables 2 and S1. Compared with the direct admission group, the patients requiring inter-hospital transfer were more likely to be treated with clopidogrel than ticagrelor, had a slightly higher use of radial artery access, were slightly less likely to undergo PCI (but more often in the left anterior descending than the right coronary artery), were less likely to undergo thrombus aspiration, and had better pre-PCI rates of TIMI 2/3 flow but similar post-PCI rates of TIMI 3 flow.
Table 2: Medications and procedural data.
As presented in S2 and S3 Tables, baseline characteristics, procedural data, and medications among patients randomized to heparin versus bivalirudin in the inter-hospital transfer and direct admission groups were well-matched.
Clinical outcomes
At 30 days, there were no significant differences in the rates of the primary composite outcome, all-cause mortality, BARC types 3–5 bleeding, stent thrombosis, MACCE or NACE between the inter-hospital transfer and direct admission groups. However, acquired thrombocytopenia was slightly more common in the inter-hospital transfer group. These findings were similar after adjustment for differences in baseline characteristics, procedural data, and medications (Table 3).
Table 3: Clinical outcomes at 30 days.
The outcomes of bivalirudin plus a post-PCI high-dose infusion for 2–4 hrs versus heparin monotherapy on 30-day clinical outcomes in the inter-hospital transfer and direct admission groups, adjusted for differences in baseline covariates and treatments, are shown in Table 4. There were no significant interactions between randomized anticoagulation use and the transfer versus direct admission subgroup on any of the 30-day primary or secondary endpoints (Fig 3).
Table 4: Clinical outcomes at 30 days according to randomization to bivalirudin vs. heparin.
Time-to-event curves at 30 days for the primary outcome and its components.(A) All-cause death or BARC types 3–5 bleeding; (B) All-cause death; (C) BARC types 3–5 bleeding. BARC, Bleeding Academic Research Consortium.
As shown in S4 Table, the results from both standard Cox models and Cox frailty models for the primary outcome were consistent, which suggested that the observed associations were not significantly influenced by inter-center variability. Furthermore, we conducted a PSM analysis, which identified 1882 well-balanced pairs. The results of this sensitivity analysis (see S5 Table) were in line with our primary findings. Lastly, we performed an additional analysis excluding patients with symptom onset-to-wire time exceeding 24 hrs, and applied multivariable Cox models. The results (see S6 and S7 Tables) remained consistent with those from the primary analysis.
Analysis according to symptom onset-to-wire time
As shown in S8 and S9 Tables, significant differences emerged in 30-day outcomes between patients with a symptom onset-to-wire time of ≥3 hrs compared with <3 hrs. Delayed reperfusion was associated with greater 30-day cardiovascular, all-cause mortality and stroke, despite similar rates of reinfarction, stent thrombosis and major bleeding, and lower rates of ischemia-driven TVR. These findings were consistent in both the inter-hospital transfer and direct admission groups. According to S10 Table, we further stratified the symptom onset-to-wire time and found that the incidence of the primary outcome increased with longer symptom onset-to-wire intervals, regardless of whether the analysis was conducted in the overall population or in the directly admitted and transferred subgroups. Although the ≥12 hrs group showed a slight decrease in the primary outcome, this finding should be interpreted with caution given the relatively small number of patients in this category.
Discussion
In the present analysis from the BRIGHT-4 trial, 30-day clinical outcomes were not significantly worse in patients with STEMI presenting at a non-PCI capable hospital who were transferred to a tertiary facility for primary PCI compared with direct admission at the interventional center, despite an increase in total ischemic time of approximately 2 hrs. In addition, the relative effects of bivalirudin with a post-PCI high-dose infusion for 2–4 hrs compared with heparin monotherapy, with GPI use reserved for bail-out complications in both arms, were consistent for all 30-day primary and secondary outcomes in the inter-hospital transfer and direct admission groups. The principal results from the BRIGHT-4 trial that bivalirudin reduced the 30-day composite outcome of all-cause death or major bleeding thus apply to patients both presenting at a PCI capable center or requiring transfer, despite the additional delay required.
Although transferring STEMI patients to a tertiary hospital for primary PCI prolongs the total ischemic time, previous studies evaluating the effect of inter-hospital transfer versus direct admission on mortality in patients with STEMI undergoing primary PCI have yielded conflicting results [3–6,8–11,16–19]. For example, Chan and colleagues reported from a single-center prospective registry study of 594 STEMI patients that inter-hospital transfer compared with direct admission to the PCI center was associated with a longer total median ischemic time of 78 min, as well as higher 30-day and 1-year mortality [16]. Conversely, in the randomized HORIZONS-AMI trial of 3,602 patients with STEMI, 30-day and 1-year clinical outcomes were comparable in patients transferred for primary PCI compared with those directly admitted to a tertiary center, despite a reperfusion delay of approximately 67 min [6]. However, in neither of these studies was primary PCI performed with the regimens that are most widely recommended and used in contemporary practice, namely heparin monotherapy and bivalirudin with a several hour post-PCI high-dose infusion. These were the randomized anticoagulation regimens used in the large-scale BRIGHT-4 trial. Moreover, in BRIGHT-4 primary PCI was also routinely performed with radial artery access, and with use of ticagrelor in the majority of patients, practices that have been shown to further reduce mortality [20,21]. These considerations warranted a re-examination of the outcomes of STEMI patients presenting at non-PCI capable versus tertiary facilities in BRIGHT-4.
In BRIGHT-4, a substantial proportion (35.7%) of patients presenting with STEMI required inter-hospital transfer prior to primary PCI. This process delayed reperfusion by about 2 hrs. Nonetheless, after adjustment for differences in baseline covariates and treatments, this delay was not associated with a significant increase in mortality, major bleeding, MACCE or NACE. There might be several explanations for this observation. First, the benefit of reperfusion therapy in reducing mortality is greatest within the first 1–3 hrs after symptom onset, most likely due to the time-dependence of myocardial salvage before transmural infarction is established. After that early period, the impact of reperfusion therapy on reducing mortality is substantially less, and thus time to reperfusion is less critical [22,23]. In our study, 30-day cardiovascular and all-cause mortality was increased in patients with symptom onset-to-wire time of ≥3 hrs compared with <3 hrs, despite similar rates of ischemic and bleeding events, likely reflecting the impact of delayed reperfusion on myocardial salvage. Symptom onset-to-wire time ≥3 hrs was associated with mortality in both the direct admission and inter-hospital transfer groups. Thus, it is likely that the total ischemic time before reperfusion, rather than the mode of transfer, had a greater effect on survival in STEMI. In this regard, the somewhat shorter symptom onset to FMC and tertiary hospital door-to-wire times in the inter-hospital transfer group compared with the direct admission group likely mitigated the impact of the time required for inter-hospital transfer. Second, we cannot exclude the role that differences in baseline features and ancillary treatments in the inter-hospital transfer and direct admission groups might have had on the results. In the PL-ACS registry [4], transferred patients had higher-risk baseline characteristics, which might have contributed to their greater mortality at 30 days. In BRIGHT-4, however, clinical outcomes were similar both before and after covariate adjustment. Additionally, it is also worth noting that ticagrelor, providing faster and greater P2Y12 receptor inhibition than clopidogrel, was more frequently chosen in patients directly admitted for primary PCI, which might be due to a worse baseline clinical profile in the direct admission group or lack of ticagrelor in some referring hospitals. These limitations at referring hospitals emphasize the necessity for optimized reperfusion strategies in scenarios when delays are inevitable. Current guidelines advocate the pharmaco-invasive strategy when FMC-to-wire time exceeds 120 min [2]. However, our study excluded patients who received thrombolytic therapy prior to PCI, which limited our ability to evaluate the pharmaco-invasive strategy. This critical evidence gap highlights the urgent need for future studies comparing clinical outcomes between STEMI patients undergoing direct primary PCI and those receiving pharmaco-invasive therapy following inter-hospital transfer.
Importantly, in BRIGHT-4 the mode of transfer neither potentiated nor attenuated the benefits observed with bivalirudin with a post-PCI high-dose infusion for 2–4 hrs compared with heparin monotherapy. After covariate adjustment for differences in patient characteristics (e.g., differences in baseline TIMI flow rates) and adjunctive treatments (e.g., ticagrelor versus clopidogrel use, which take time to work in STEMI [24,25]), the relative hazards for all primary and secondary ischemic and bleeding outcomes with these anticoagulation regimens were consistent in the inter-hospital transfer and direct admission groups. Thus, the principal results of BRIGHT-4 apply to transfer patients as well as those presenting to a tertiary facility – STEMI patients undergoing primary PCI who are anticoagulated with bivalirudin plus a post-PCI high-dose infusion for 2–4 hrs have lower rates of all-cause mortality, major bleeding, stent thrombosis and NACE compared with heparin monotherapy [14]. Future studies with larger sample sizes or longer follow-up periods may help clarify whether this trend translates into a significant benefit.
The reduction in stent thrombosis in BRIGHT-4 after primary PCI with bivalirudin compared with heparin, even in patients presenting late after prolonged transfer, is notable. In the HORIZONS-AMI trial, the rate of stent thrombosis within the first 4 hrs after randomization was increased in patients treated with bivalirudin compared with heparin [26]. However, all heparin-treated patients in that trial also received a GPI, the only therapy shown to reduce stent thrombosis after stent implantation in STEMI [27], and bivalirudin was discontinued immediately after the PCI procedure, a risk factor for early stent thrombosis given its short (25-minute) half-life. In contrast, in BRIGHT-4, the platelet activation that is known to occur after heparin use alone [28] likely resulted in increased rates of early stent thrombosis in patients randomized to heparin monotherapy without routine GPI administration, and in the bivalirudin arm, the median 3-hr post-PCI bivalirudin infusion was sufficient to suppress stent thrombosis in the early risk period, as first described in the EUROMAX trial [29].
Symptom onset-to-FMC time in BRIGHT-4 was longer than in previous studies, in part due to inclusion of patients with STEMI as late as 48 hrs after symptom onset, as opposed to 12 or 24 hrs in previous studies [3,4,6,17]. Moreover, the inter-hospital transfer group had a median FMC-to-wire time of 3.57 hrs (reflecting large inter-hospital distances in China, as well as other logistical considerations in transport), well past the guideline-recommended duration of 120 min [2]. As door-in door-out (DIDO) times of ≤30 min have been associated with lower in-hospital mortality [30], it is imperative to minimize referral-related delays. However, tertiary hospitals managed to significantly reduce door-to-wire times in transferred patients by proactively preparing the catheterization laboratory and bypassing the emergency room [6].
This study highlighted the value of a time-based stratified management strategy that prioritized total ischemic time over the specific mode of transfer. It underscored the essential role of timely reperfusion in optimizing outcomes for both directly admitted and transferred STEMI patients. The results supported the hypothesis that bivalirudin might serve as a preferable anticoagulant option during primary PCI, offering enhanced safety and survival benefits compared to heparin monotherapy, regardless of whether patients were transferred or not. Nonetheless, further research is warranted to evaluate the long-term prognostic implications of inter-hospital transfer and to assess the sustained benefits of bivalirudin therapy over time.
This study also has some limitations. First, as a post hoc analysis, randomization was not stratified by transfer status, and no adjustment was made for multiple comparisons, which may have increased the risk of type I error. Although multivariable analysis was used to adjust for differences in baseline characteristics, medications and procedures (most of which were modest) between the inter-hospital transfer and direct admission groups, selection bias and unmeasured confounders cannot be excluded. These results should be interpreted with caution in the context of an underpowered subgroup analysis. Accordingly, our results should be considered hypothesis-generating rather than conclusive inference and warrant dedicated, prospective confirmation. Second, we did not collect detailed data regarding the use of emergency medical services and DIDO times, resulting in our inability to accurately analyze all the reasons for treatment delay. Finally, as the present analysis reports only 30-day outcomes, further studies are needed to investigate the impact of transfer on the long-term prognosis of STEMI patients.
We concluded that in the BRIGHT-4 trial, transferring patients with STEMI presenting at a non-PCI capable hospital to a tertiary facility for primary PCI was not associated with significantly worse 30-day mortality, MACCE or NACE compared with direct admission, despite treatment delays and longer times to reperfusion. Procedural anticoagulation with a post-PCI high-dose bivalirudin infusion for 2–4 hrs was associated with lower rates of 30-day all-cause mortality, major bleeding, and stent thrombosis compared with heparin monotherapy, regardless of whether patients were transferred or admitted directly to the interventional facility for primary PCI.
Supporting information
S1 TableMedications and procedural data.(DOCX)
S2 TableBaseline characteristics of patients randomized to heparin versus bivalirudin.(DOCX)
S3 TableMedications and procedural data in patients randomized to bivalirudin versus heparin.(DOCX)
S4 TableComparison of HRs (95% CI) for the primary outcome: Cox model versus Cox frailty model.(DOCX)
S5 TableClinical outcomes at 30 days after propensity score matching.(DOCX)
S6 TableClinical outcomes at 30 days in patients with symptom onset-to-wire time ≤24 hrs.(DOCX)
S7 TableClinical outcomes at 30 days according to randomization to bivalirudin versus heparin in patients with symptom onset-to-wire time ≤24 hrs.(DOCX)
S8 TableClinical outcomes at 30 days according to symptom onset-to-wire time.(DOCX)
S9 TableClinical outcomes at 30 days in the direct admission versus inter-hospital transfer groups according to symptom onset-to-wire time.(DOCX)
S10 TableMultivariable-adjusted HRs (95% CI) of 30-day primary outcome according to symptom onset-to-wire time.(DOCX)
S1 ChecklistCONSORT 2025 checklist.(DOCX)
S1 TextInstitutional review boards.(DOCX)
S2 TextStudy protocol.(DOCX)
S3 TextStatistical analysis plan.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1O’Gara PT, Kushner FG, Ascheim DD, Casey DE Jr, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2013;127(4):e 362–425. doi: 10.1161/CIR.0b 013e 3182742 cf 6 23247304 · doi ↗ · pubmed ↗
- 2Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–77. doi: 10.1093/eurheartj/ehx 393 28886621 · doi ↗ · pubmed ↗
- 3Rathod KS, Jain AK, Firoozi S, Lim P, Boyle R, Nevett J. Outcome of inter-hospital transfer versus direct admission for primary percutaneous coronary intervention: an observational study of 25,315 patients with ST-elevation myocardial infarction from the London Heart Attack Group. Eur Heart J Acute Cardiovasc Care. 2020;9(8):948–57.32193943 10.1177/2048872619882340 · doi ↗ · pubmed ↗
- 4Kawecki D, Gierlotka M, Morawiec B, Hawranek M, Tajstra M, Skrzypek M, et al. Direct admission versus interhospital transfer for primary percutaneous coronary intervention in ST-segment elevation myocardial infarction. JACC Cardiovasc Interv. 2017;10(5):438–47. doi: 10.1016/j.jcin.2016.11.028 28216215 · doi ↗ · pubmed ↗
- 5Hu D, Hao Y, Liu J, Yang N, Yang Y, Sun Z. Inter-hospital transfer in patients with acute myocardial infarction in China: findings from the improving care for cardiovascular disease in China-acute coronary syndrome project. Front Cardiovasc Med. 2022;9:1064690.36568538 10.3389/fcvm.2022.1064690 PMC 9773877 · doi ↗ · pubmed ↗
- 6Wöhrle J, Desaga M, Metzger C, Huber K, Suryapranata H, Guetta V, et al. Impact of transfer for primary percutaneous coronary intervention on survival and clinical outcomes (from the HORIZONS-AMI Trial). Am J Cardiol. 2010;106(9):1218–24. doi: 10.1016/j.amjcard.2010.06.049 21029816 · doi ↗ · pubmed ↗
- 7Hillerson D, Li S, Misumida N, Wegermann ZK, Abdel-Latif A, Ogunbayo GO, et al. Characteristics, process metrics, and outcomes among patients with ST-elevation myocardial infarction in rural vs urban areas in the US: a report from the US national cardiovascular data registry. JAMA Cardiol. 2022;7(10):1016–24. doi: 10.1001/jamacardio.2022.2774 36044196 PMC 9434481 · doi ↗ · pubmed ↗
- 8van Diepen S, Widimsky P, Lopes RD, White KR, Weaver WD, Van de Werf F. Transfer times and outcomes in ST-elevations myocardial infarction patients undergoing inter-hospital transfer for primary percutaneous coronary intervention: APEX-AMI insights. Circ Cardiovasc Qual Outcomes. 2012;5(4):437–44.22589297 10.1161/CIRCOUTCOMES.112.965160 PMC 3571720 · doi ↗ · pubmed ↗