Psychological distress and compliance with sanitary measures during the Covid-19 pandemic
Irwin Hecker, Solène Wallez, Honor Scarlett, José Luis Ayuso-Mateos, Richard Bryant, Giulia Caggiu, Claudia Conflitti, Katalin Gémes, Josep Maria Haro, Vincent Lorant, Roberto Mediavilla, Ellenor Mittendorfer-Rutz, Anna Monistrol-Mula, Matteo Monzio Compagnoni

TL;DR
This study finds that psychological distress affects compliance with sanitary measures during the pandemic differently in men and women.
Contribution
The study reveals gender-specific and education-based differences in how psychological distress influences compliance with sanitary measures.
Findings
Women with psychological distress showed increased compliance with sanitary measures.
Men with psychological distress, especially those with low education, showed decreased compliance.
Educational level modified the relationship between distress and compliance in men.
Abstract
This study aims to understand the relationship between the experience of psychological distress and compliance with COVID-19 sanitary measures. We testeed whether this relationship was modified by individuals’ gender and socioeconomic status (i.e., educational level and employment). Data from four European cohort studies (n = 13,635), were analysed using an Individual Participant Data (IPD) meta-analytic approach. Mixed effect models were employed to examine associations between mental health difficulties and compliance with sanitary measures, as well as effect modification by socioeconomic status. Statistical models were stratified by gender. We found a statistically significant association between mental health difficulties and increased compliance with sanitary measures in women, while amongst men the statistically significant association observed was opposite. Moreover, there was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
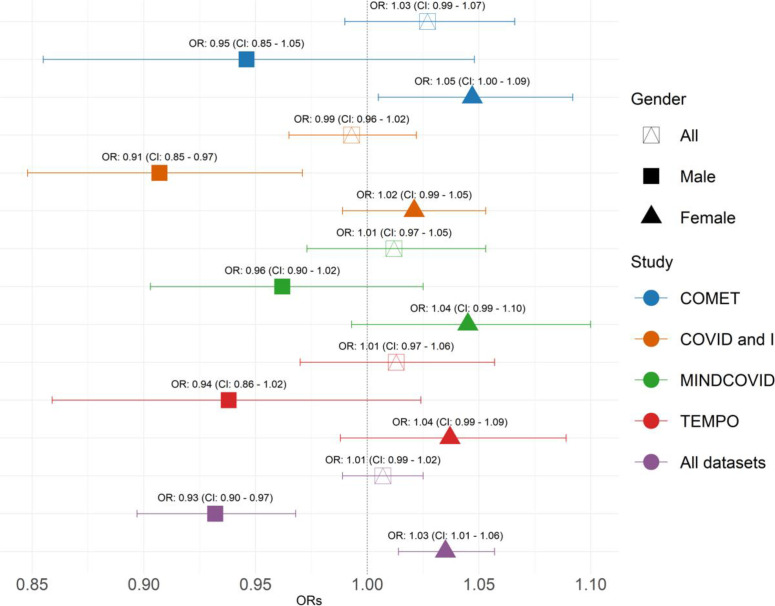 Fig 1
Fig 1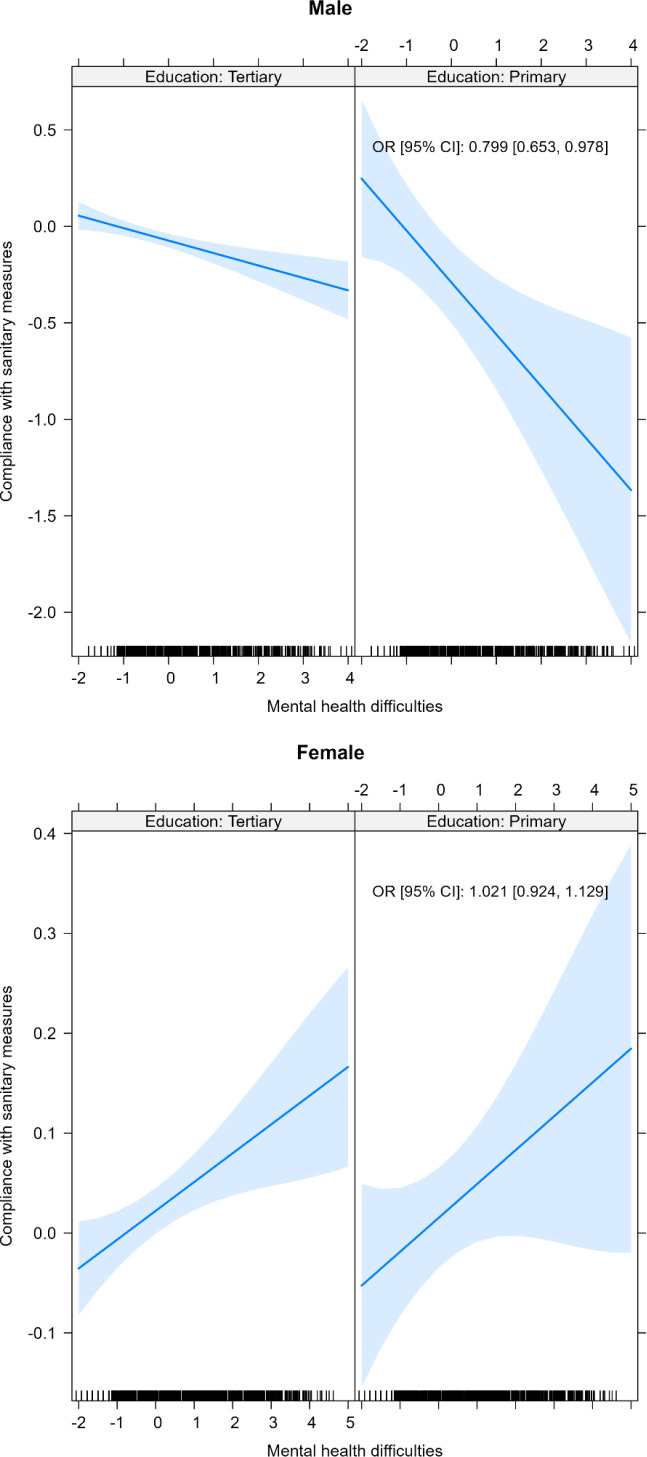 Fig 2
Fig 2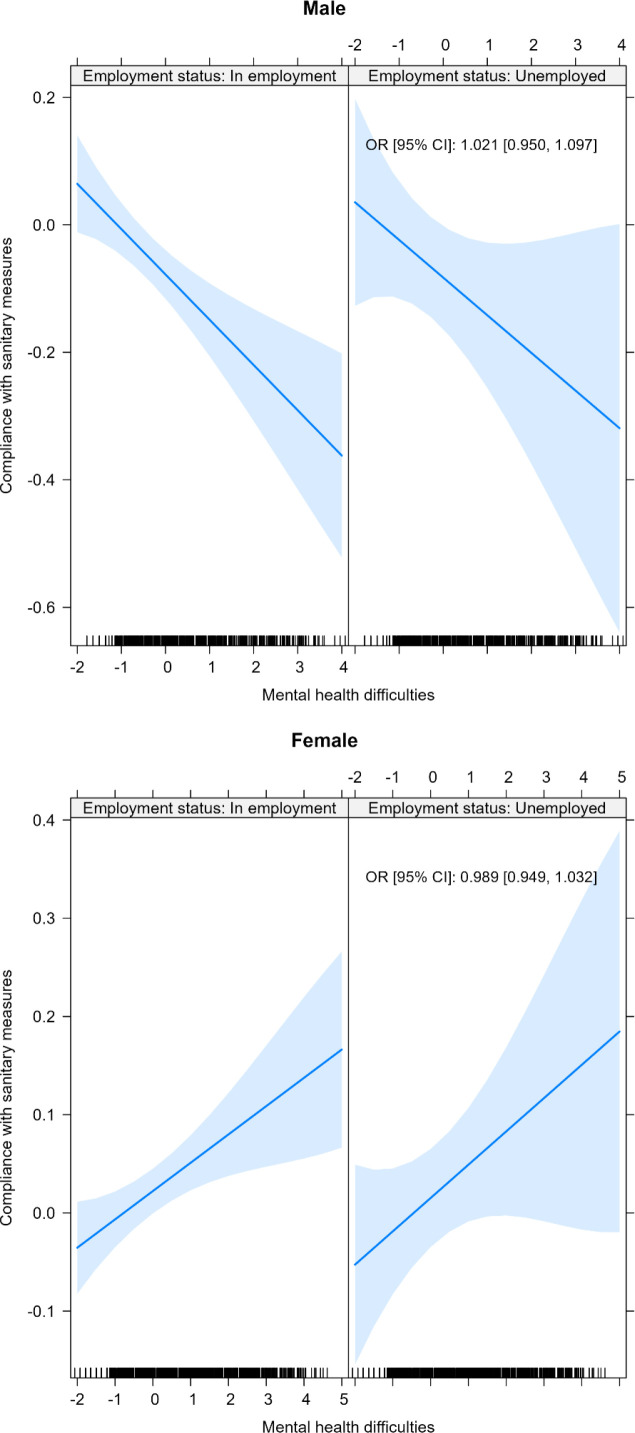 Fig 3
Fig 3- —EU Horizon 2020 H2020-SC1-PHE-CORONAVIRUS-2020-2
- —French National Research Agency (ANR)
- —Interministerial Agency for Drug and Addictive Behaviors (MILDECA)
- —French National Cancer Institute (INCA)
- —Instituto de Salud Carlos III, ISCIII, FPU and the Generalitat de Catalunya
- —King Baudouin Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Healthcare professionals’ stress and burnout · COVID-19 Pandemic Impacts
Introduction
Echoing patterns seen during prior epidemics [1], the COVID-19 pandemic showed widespread adverse impacts on global mental health [2–6]. The implementation of sanitary measures played a crucial role in mitigating the pandemic and preserving population [7]. Once sanitary measures are introduced, compliance is critical and determines their effectiveness and epidemiological impact [8].
Psychological distress, defined as experience of symptoms of depression, anxiety, insomnia, and multiple psychosocial complaints, which do not necessarily correspond to established diagnoses of psychiatric disorders but nevertheless lead to suffering and reduced quality of life, could be related to various aspects of individuals’ health behaviours, including compliance with sanitary measures at times of a health crisis. However the nature of the relationship between psychological distress and compliance with sanitary measures during a pandemic such as COVID-19 is complex from a theoretical perspective and past studies have yielded inconsistent findings. Symptoms of anxiety could lead individuals to be especially cautious and implement all sanitary measures with diligence, as has been shown among persons with mental health problems prior to the occurrence of the COVID-19 pandemic (for instance symptoms of depression), who were especially likely to implement social distancing, even as the pandemic subsided [9]. On the other hand, persons experiencing psychological distress might face socioeconomic difficulties, a factor associated with a reduced level of compliance with sanitary measures [10–12], which was observed during the COVID-19 pandemic [13,14].
Additionally, the COVID-19 pandemic worsened pre-existing gender inequalities. Women were more likely to experience psychological distress, including symptoms of anxiety and depression [15], before the pandemic, and the additional family charges experienced as a consequence of the health crisis (e.g., disproportionate caregiving burden during consecutive lockdowns, school closures) further amplified these pre-existing gender inequalities [16,17]. Employed women were at particularly high risk of having mental health difficulties given that they often carried the burden of domestic responsibilities, such as caring for children and the elderly, as well as changes in work-life balance [16,17]. On the other hand, women aged 35–39 years experienced higher levels of pandemic-induced unemployment, with an especially high risk in low educated women with young children [18].
Sanitary measures introduced to limit COVID-19 spread (e.g., lockdowns and business closures, remote work mandates, social distancing regulations, travel or healthcare access restrictions, school and university closures, and border closures) [19] had uneven economic and social impacts [20]. Whilst these measures were proven to mitigate COVID-19 outcomes, they exacerbated socioeconomic inequalities [21,22] due to heterogeneity in individuals’ ability to work remotely, or in the probability of COVID-19 infection within the household [23]. Individuals with no formal education and those with only primary education were less aware of available mental health care services [24]. Being employed [25] and having a low educational level [25–28] were also associated with non-compliance with sanitary measures–it may be because of other priorities such as securing means of subsistence [25], or the necessity to accept unsafe work conditions or even unstable income sources [25,29–31]. Regarding gender differences, behaviours also differ. More specifically women tend to be more compliant with precautionary measures (e.g., reduced mobility or wearing masks) than men [32].
We anticipated that compliance with sanitary measures during the COVID-19 pandemic would prove challenging for certain population groups. Specifically, we hypothesised that the association between compliance with sanitary measures and psychological distress would differ across genders and that educational level and employment status would further play a role in shaping these behaviours.
Methods
Study design and population
To investigate the relationship between the experience of psychological distress and compliance with sanitary measures, we combined data from multiple datasets collected during the COVID-19 pandemic into an Individual Participant Data (IPD). We employed IPD meta-analysis [33] utilising datasets exclusively sourced from partners within the RESPOND project. We carefully curated target variables and harmonised participating datasets to render the data comparable. Rigorous quality checks were conducted to ensure the reliability and integrity of all included data. This approach enhances the depth and reliability of our findings, enabling robust conclusions to be drawn from the combined datasets contributed by RESPOND project partners.
Data from four observational cohort studies were included: (i) the TEMPO (Trajectoires ÉpidéMiologiques en Population) [34], (ii) MINDCOVID [35], (iii) COVID and I [36], and (iv) the COVID-19 Mental Health Survey (COMET) [37].
The TEMPO cohort began in 2009 in France with the aim of better understanding mental health patterns and addictive behaviours. Starting from 2020, TEMPO participants were contacted to collect data regarding their health status during the COVID-19 pandemic. Nine waves of data were collected using self-administered questionnaires from March 24, 2020 (one week after the beginning of the first lockdown) to the end of July 2021. All COVID-19 study data waves were included in this study.
The MINDCOVID project is a survey of general population adults in Spain. The target population consisted of non-institutionalised Spanish adults (i.e., aged 18 years or older) without Spanish language barriers. Professional interviewers carried out computer-assisted telephone interviews (1–30 June 2020) in a sample drawn using dual-frame random digit dialling. Only the first and second waves of data collection were included in the present study, as compliance with sanitary measures was reported in these two study waves only.
COVID and I is an online survey conducted across Belgium through social media and national news outlets at the beginning of the first wave of the COVID-19 pandemic in 2020. The survey was launched on March 20^th^ 2020, two days after the beginning of lockdown. The survey was aimed at the general population and was available in English, French, and Dutch. Only the fourth wave of data collection in 2021 was included in this study as questions related to compliance with sanitary measures were asked at that wave only.
The COMET study is an international, online longitudinal survey aimed at evaluating the course of mental health symptoms during the COVID-19 pandemic, as well as identifying individuals at greater or reduced risk of mental illness. It includes participants from 14 countries (The Netherlands, Italy, Switzerland, Turkey, Spain, Germany, France, the United Kingdom, Sweden, South Africa, Indonesia, China, Australia and the United States). Participants were recruited starting in May 2020 through a snowball sampling strategy using university mailing lists and different social media platforms. Only the fourth and fifth waves of data collection in 2021 were included in the present study as questions related to compliance with sanitary measures were asked in these study waves only.
Data collection procedures are detailed in S1 Fig and population selection in S2 Fig. Other RESPOND databases (EDAD CON SALUD, HEROES, LORA, MARP, DYNACORE-L) were not included because they did not include information regarding compliance with sanitary measures (EDAD CON SALUD, HEROES, LORA, MARP) or mental health (DYNACORE-L).
Ethics
All participating studies were approved by the appropriate ethics committee and were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
The TEMPO cohort received approval of bodies supervising ethical data collection in France, the Advisory Committee on the Treatment of Information for Health Research (Comité consultatif sur le traitement de l’information en matière de recherche dans le domaine de la santé, CCTIRS) and the French regulatory data protection authority (Commission Nationale de l’Informatique et des Libertés, CNIL, n◦ 908163).
The MINDCOVID study protocol was approved by the IRB Parc de Salut Mar (2020/9203/I) and by the corresponding IRBs of all the participating centres. The study is registered at ClinicalTrials.gov (https://clinicaltrials.gov/ct2/show/NCT04556565).
Covid and I’s ethical review and approval were not required as it is a population-based, online survey with no collection of personal data. Participants were provided with study information and online informed consent was obtained from all study participants.
The COMET study was approved by the ethical review board of the Faculty of Behavioral and Movement Sciences of the Vrije Universiteit Amsterdam (VCWE-2020–077). Personal data are protected according to EU and national laws.
All data included in the present analyses were fully anonymized.
Measures
Outcome.
Compliance with sanitary measures was ascertained using self-reported items (handwashing, social distancing, physical contact, wearing a mask, lockdown, working from home, limiting small and/or large gatherings, curfew, hosting people at home, quarantine, and taking extra precautions with at risk people). These items were harmonised and summed (S1 Table); z-scores were calculated in each study sample.
Exposure
Psychological distress was measured using the following psychological scales: COMET: Patient Health Questionnaire Anxiety and Depression Scale (PHQ-ADS) [38]; COVID and I: General Health Questionnaire-12 (GHQ-12) [39]; MINDCOVID: Patient Health Questionnaire-8 and the Anxiety and Depression Scale (PHQ8-ADS) [40]; TEMPO: Adult Self-Report (ASR)) [41]; these were harmonised using a standard procedure: first, for each scale all items were summed (S2 Table); next corresponding z-scores were calculated. In this way, individual values of each single scale across the four studies were transformed into a measure of the same order of magnitude (numeric, with specific minimum and maximum), making them comparable across samples.
Covariates
Participants’ sociodemographic characteristics were collected across the four cohort studies included, coded consistently using the same names, values, and formats and included: gender (“Female”; “Male”), age, education (“Tertiary”; “Primary”; “Secondary”), employment status (“In employment”; “Unemployed”), and number of children (“No children”; “One”; “Two or three”; “Four or more”).
All variables accounted for in this study had previously been reported as factors associated with compliance with sanitary measures: female gender [28,42–46], age [26,43,44,46–50], educational level [25–28], employment status [51] and the number of children [52].
A “stringency” variable was also included, based on the Stringency Index [53], which incorporates nine metrics: school, workplace, or public transport closures, the cancellation of public events, restrictions on public gatherings, restrictions on internal movements, stay-at-home requirements, public information campaigns, and international travel controls. The score corresponds to the mean score of these nine metrics, with each metric ranging from 0 to 100. A higher number on the Stringency Index represents a stricter response to the COVID-19 pandemic, with 100 indicating the strictest possible measures.
Statistical analysis
To test associations between participants’ psychological distress and compliance with the sanitary measures implemented during the COVID-19 pandemic, individual participant data from relevant studies was merged and analysed. Due to the longitudinal nature of the data, mixed effect models were used to calculate adjusted odds ratios (aOR), and the corresponding 95% confidence intervals (CI). Multivariate mixed effect models were adjusted for the above-listed covariates (please see the “Covariates” subsection). Analyses were conducted individually in each database, as well as in the merged dataset. We did not conduct country-specific analyses of the COMET data, as sample sizes are too small [54]. Data were stratified by gender to consider gender-specific patterns related to the outcome, exposure, and socioeconomic status. Additionally, interactions between socioeconomic status and exposure were explored. P-values of less than 0.05 were considered to be statistically significant. Collinearity of model variables was explored and measured using Variance Inflation Factor (VIF) derivatives, namely generalised VIF (GVIF) and GVIF^(1/(2*Df)) [55–58]. After removing incomplete cases in terms of the outcome and exposure, we included 19,143 longitudinal observations (from 13,635 participants). Incomplete data on covariates, with an average of 5% missing data, were imputed using Multiple Imputations by Chained Equations (MICE) with Fully Conditional Specification (FCS), based on five multiple imputations [59,60]. All statistical analyses were performed using R version 4.2.3 and Rstudio version 2023.6.1.524 [61].
Results
Participants of the four cohorts studied showed many similarities, including a higher proportion of women (68.9%), and higher rates of both tertiary education (83.7%) and employment (83.5%). Participants’ mean age in each cohort ranged from 40 to 46 years. Among TEMPO participants, there was a high proportion of individuals with two or three children (57.9%), while most participants in the COMET, COVID and I and MINDCOVID cohorts, had no children (respectively 56.6%, 40.9%, 54.8%). The mean Stringency Index score ranged from 55 for COMET to 81 for TEMPO (Table 1).
Table 1: Characteristics of COMET, COVID and I, Mind COVID, and TEMPO cohort studies, March 2020–August 2022, n = 13,635.
When data were stratified by gender and adjusting for covariates, the association between psychological distress and compliance with sanitary measures was negative in men (aOR: 0.93, 95%CI: 0.90–0.97) and positive in women (aOR: 1.03, 95%CI: 1.01–1.06) (Fig 1).
Association between psychological distress and compliance with sanitary measures in COMET, COVID and I, Mind COVID, TEMPO studies, and all populations, March 2020–August 2022, n = 13,635 (multivariate mixed models, adjusted odds-ratios (aOR), 95% confidence interval (CI)).All models adjusted for gender (except when stratified), age, education, employment status, number of children, and stringency. Both x and y axes show z scores.
Additionally, we found a statistically significant interaction between psychological distress and primary educational level among men (aOR: 0.82, 95%CI: 0.68–0.99) (Fig 2), but not in other categories of education and employment status (Fig 3).
Interaction between participants’ educational level and psychological distress in relation to compliance with COVID-19 sanitary measures (COMET, COVID and I, Mind COVID, TEMPO studies), March 2020–August 2022, n = 13,635 (multivariate mixed models).All models adjusted for age, education, employment status, number of children, and stringency. Both x and y axes show z scores.
Interaction between participants’ employment status and psychological distress in relation to compliance with COVID-19 sanitary measures (COMET, COVID and I, Mind COVID, TEMPO studies), March 2020–August 2022, n = 13,635 (multivariate mixed models).All models adjusted for age, education, employment status, number of children, and stringency. Both x and y axes show z scores.
Discussion
Main findings of this study
Data collected among the 13,635 participants of the COMET, COVID and I, MINDCOVID and TEMPO cohorts from March 2020 to August 2022, revealed an association between psychological distress and compliance with sanitary measures during the COVID-19 period when stratified by gender. Women experiencing psychological distress showed higher compliance with sanitary measures, whereas the opposite relationship was observed amongst men. Additionally, an interaction between psychological distress and educational level among men was observed, such that compliance with sanitary measures was lowest in those with a low educational level.
What is already known on this topic
The influence of both gender and socioeconomic characteristics on the association between psychological distress and compliance with sanitary measures is not yet well documented. Previous studies suggested that psychological distress has different effects on compliance with sanitary measures in men and women. Indeed, gender disparities in risk-taking behaviours [62] and health-related decision-making patterns during the COVID-19 pandemic have been documented [63]. Globally, men are more likely to engage in risky behaviours and less inclined to seek preventive medical care, or support for health issues [64–66]. During the pandemic, men perceived the consequences of COVID-19 to be less severe compared to women, despite objective evidence suggesting otherwise. Traditional masculinity norms appear to moderate this perception, which, in turn, negatively affects adherence to precautionary measures [67].
What this study adds
Our study has a number of strengths worth highlighting. A significant strength of our study lies in the IPD meta-analytical approach, which enabled us to include four large cohort studies. IPD meta-analyses are recognized for providing a more comprehensive assessment of pooled data when compared to aggregate data analyses [68]. This methodology also allowed us to extract and analyse raw data from each individual study, including diverse spatial and temporal contexts throughout the COVID-19 pandemic, and thus enhance the precision and robustness of our findings by considering various contexts of data collection.
We observed an interaction between psychological distress and educational level in terms of compliance with COVID-19 sanitary measures was observed among men. This suggests an especially low level of compliance with sanitary measures in this group. It is known that bi-directional effects between academic achievement and social withdrawal exist in boys, increasing the risk of psychosocial maladjustment, depression, loneliness and anxiety [69]. It may also be that men and particularly those belonging to low educated groups face a number of challenges in terms of work and daily life, which make it less likely for them to invest in their health. This may partially explain the subsequent difficulty in complying with precautionary health measures in case of a pandemic.
Containment policies have resulted in a reduction of the impact of COVID-19 on population health [70,71]. Sanitary measures were proven to contain the spread of the virus [71,72], showing a linear, inverse relationship between the incidence of COVID-19 and degree of observed prevention measures [73]. During a health crisis, awareness of groups with low compliance to sanitary measures can be of help when intervening proactively, especially considering that shorter lockdown periods can be compensated for by high adherence to health-oriented interventions [8]. It is, then, important to educate the public about the negative consequences of the virus and the effectiveness of sanitary measures [74]. Regarding mental health, recommendations should aim to reduce mental health inequalities between vulnerable groups and the general population using measures targeted adapted to specific contexts [75].
As has previously been recommended, a gender-specific response to a new health risks emphasises the need for targeted public health messaging [32]. In a recent scoping review [63], it was revealed that individuals’ perceptions of COVID-19 health information and recommendations, as well as their decisions regarding health matters, are significantly influenced by their level of education and health literacy. This is particularly important since the effectiveness of containment measures in a case such as a pandemic as COVID-19 relies on widespread public understanding and support. Targeting low educated men with tailored mental health interventions would not only help tackle psychological distress related to the pandemic but also promote compliance with sanitary measures, thus reducing the risk of infection [76]. Mental health interventions for vulnerable groups are currently being tested within the context of the COVID-19 pandemic and its aftermath [77–80].
Study limitations
We need to acknowledge some limitations to our study. First, as the data were self-reported, it may contain biases stemming from social desirability and memory recall issues [81]. Second, some key variables, such as participants’ income [27,44,47,50,82], presence of a chronic illness [83], or COVID-19-related worries [26] were excluded due to their heterogeneity across all included studies. Additionally, we were not able to measure participants’ risk perceptions, which were not systematically assessed in all participating cohorts. However, this selective inclusion was a deliberate choice aimed at maintaining methodological consistency across studies and ensuring rigorous statistical analyses. By focusing on variables shared across different cohorts, we enhanced the internal validity of our study, thereby providing a more reliable synthesis of the available evidence. Both outcome and exposure data were derived from distinct validated scales and questions within each survey, which were subsequently pooled post-collection using methods distinct from the standard approaches for the respective scales. Third, this set of data is not comprehensive as it was not identified and selected systematically; rather, it was included from datasets provided by partners of the RESPOND project. Nevertheless, this approach allowed a harmonised comparison of different datasets.
Conclusion
Our study underscores the need for targeted interventions related to compliance with preventive measures among persons experiencing psychological distress, particularly during health crises like the COVID-19 pandemic. Our findings highlight the importance of tailoring messaging and strategies to address the unique challenges faced by different populations. Targeting specific groups with lower rates of compliance through tailored messaging is essential for effective management of health crises, such as the COVID-19 pandemic. Men experiencing psychological distress, especially those with lower educational attainment, show limited compliance with sanitary measures. This calls for targeted approaches towards men experiencing psychological distress, especially those with lower educational attainment. By promoting individuals’ well-being, taking into account their mental health, gender, and socioeconomic characteristics, we may better prepare for future health crises.
Supporting information
S1 FigData collected in the COMET, COVID and I, Mind COVID and TEMPO studies, March 2020–August 2022, n = 13,635.(DOCX)
S2 FigFlow chart of COMET, COVID and I, Mind COVID, and TEMPO samples, March 2020–August 2022, n = 13,635.(DOCX)
S1 TableItems measuring compliance with sanitary measures against COVID-19 available in COMET, COVID and I, Mind COVID and TEMPO studies, March 2020–August 2022, n = 13,635.(DOCX)
S2 TableMeasures of mental health available in the COMET, COVID and I, Mind COVID and TEMPO studies, March 2020–August 2022, n = 13,635.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shah K, Kamrai D, Mekala H, Mann B, Desai K, Patel RS. Focus on mental health during the coronavirus (covid-19) pandemic: applying learnings from the past outbreaks. Cureus. 2020;12(3):e 7405. doi: 10.7759/cureus.7405 32337131 PMC 7182052 · doi ↗ · pubmed ↗
- 2Talevi D, Socci V, Carai M, Carnaghi G, Faleri S, Trebbi E, et al. Mental health outcomes of the Co Vi D-19 pandemic. Riv Psichiatr. 2020;55(3):137–44. doi: 10.1708/3382.33569 32489190 · doi ↗ · pubmed ↗
- 3Serafini G, Parmigiani B, Amerio A, Aguglia A, Sher L, Amore M, et al. The psychological impact of COVID-19 on the mental health in the general population. QJM Int J Med 2020;113:531–7. doi: 10.1093/qjmed/hcaa 201PMC 733785532569360 · doi ↗ · pubmed ↗
- 4Xiang Y-T, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020;7(3):228–9. doi: 10.1016/S 2215-0366(20)30046-8 32032543 PMC 7128153 · doi ↗ · pubmed ↗
- 5Xiong J, Lipsitz O, Nasri F, Lui LMW, Gill H, Phan L, et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J Affect Disord. 2020;277:55–64. doi: 10.1016/j.jad.2020.08.001 32799105 PMC 7413844 · doi ↗ · pubmed ↗
- 6Witteveen AB, Young SY, Cuijpers P, Ayuso-Mateos JL, Barbui C, Bertolini F, et al. COVID-19 and common mental health symptoms in the early phase of the pandemic: An umbrella review of the evidence. P Lo S Med. 2023;20(4):e 1004206. doi: 10.1371/journal.pmed.1004206 37098048 PMC 10129001 · doi ↗ · pubmed ↗
- 7Paulo MS, Peyroteo M, Maia MR, Pries C, Habl C, Lapão LV. Impacts of public health and social measures on COVID-19 in Europe: a review and modified Delphi technique. Front Public Health. 2023;11:1226922. doi: 10.3389/fpubh.2023.1226922 37719729 PMC 10501783 · doi ↗ · pubmed ↗
- 8Chen J, Vullikanti A, Santos J, Venkatramanan S, Hoops S, Mortveit H, et al. Epidemiological and economic impact of COVID-19 in the US. Sci Rep. 2021;11(1):20451. doi: 10.1038/s 41598-021-99712-z 34650141 PMC 8517017 · doi ↗ · pubmed ↗